





Figures
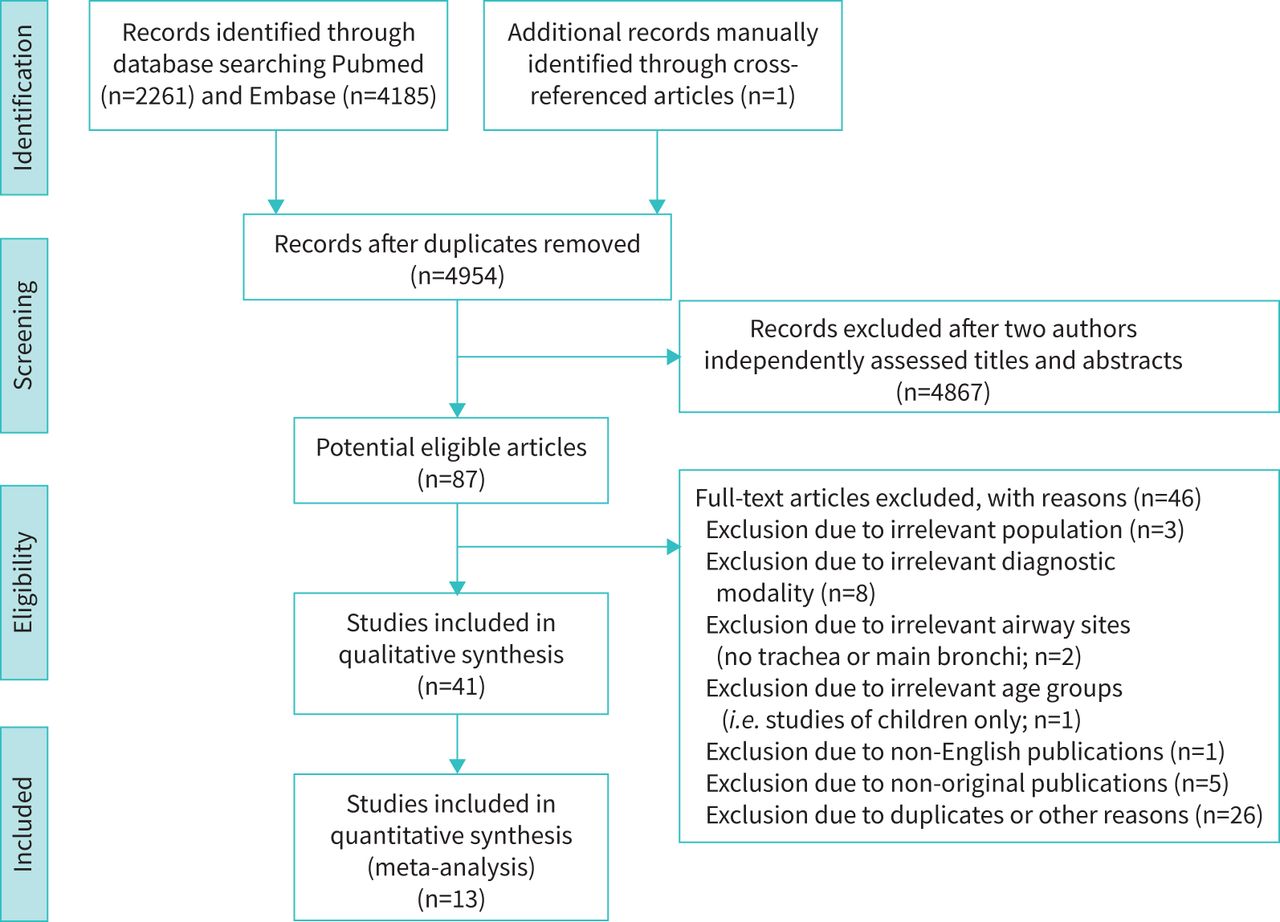
- FIGURE 1
PRISMA flow chart for study selection.
- FIGURE 2
Study cut-off thresholds reported for the diagnosis of large airway collapse, based on diagnostic modality. CSA: cross-sectional area; CT: computed tomography; MRI: magnetic resonance imaging.
- FIGURE 3
Forest plot of the prevalence of large airway collapse in healthy subjects. Random effects meta-analysis was done to estimate the pooled prevalence. Details of included studies, including population, diagnostic modality and threshold, are summarised in table 1.
- FIGURE 4
Forest plot of the prevalence of large airway collapse in patients with chronic obstructive airway diseases (either COPD or asthma). Random effects meta-analysis was done to estimate the pooled prevalence. Details of included studies, including population, diagnostic modality, and threshold, are summarised in table 2. AE: acute exacerbation.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Bronchoscopic studies
First author/year Study purpose and design Population Diagnostic modality Diagnostic criteria Findings Discussion Majid et al. 2014 [19] Prospective single-centre study
Assessing inter- and intra-observer agreement in LAC10 patients (males (n=4), females (n=6); mean age: 65 years, age range: 43–74 years) with various conditions Dynamic flexible bronchoscopy TBM or EDAC ≥50% reduction in the anteroposterior diameter TBM was found in 70% of patients There is intra- and interobserver agreement among pulmonologists and trainees with various levels of experience in the evaluation of LAC Dal Negro et al. 2013 [7] Prospective single-centre study
Assessing the prevalence of both TBM and EDAC202 asthmatics (males (n=91), females (n=111); age: 47.5±13.3 years), and 62 subjects without any obstructive disease (males (n=38), females (n=24); age: 38.9±10.4 years) Dynamic flexible bronchoscopy TBM or EDAC >50% of airway collapse TBM and particularly EDAC prevalence are related to asthma severity The presence of TBM or EDAC should be considered when bronchial asthma persists despite appropriate pharmacological treatment Murgu & Colt, 2007 [18] Retrospective single-centre study
Assessing a multidimensional classification system (FEMOS) for evaluating patients with expiratory LAC18 patients (males (n=13), females (n=5); 4 with EDAC and 14 with TBM) Rigid bronchoscopy LAC, normal <50%, mild, 50–75%; moderate, 75–100%; and severe, 100% and the airway walls make contact EDAC and TBM were found in 22.2% and 77.8%, respectively Using FEMOS, the morphologies and aetiologies of LAC can be identified and stratified objectively based on the degree of functional impairment, extent of disease and severity of airway collapse LAC: large airway collapse; TBM: tracheobronchomalacia; EDAC: excessive dynamic airway collapse.
- TABLE 2
Computed tomographic and magnetic resonance imaging studies
First author/year Study purpose and design Population Diagnostic modality Diagnostic criteria Findings Discussion Bezuidenhout et al. 2019 [51] Retrospective single-centre study
To evaluate patients with TBM after undergoing tracheobronchoplasty18 patients (males (n=5), females (n=13); mean age: 65±12 years) with COPD (n=7), GERD (n=14), OSA (n=8), cardiac disease (n=4) 8-, 16- and 64-MDCT scan LAC ≥70% reduction in the CSA Mean tracheal collapsibility improved by 34% in post-operative CT Dynamic CT could play an important role in assessing response to tracheobronchoplasty Nygaard et al. 2019 [29] Retrospective/prospective single-centre study
To assess TM over time (2 CT scans) in patients with excessive tracheal collapse20 patients with respiratory diseases (males (n=6), females (n=14); mean age: 68 years) high-resolution
MDCT scanTM ≥50% reduction in the CSA Seven patients showed a tracheal collapse progression (>10% difference) between the scans Tracheal collapse regressed in half of the patients over a time period of 2 years Ciet et al. 2017 [31] Prospective single-centre study
Comparison of MRI to MDCT in assessing TBM12 participants (males (n=5), females (n=7); 9 healthy adults and 3 patients with COPD; mean age: 64.5 years, age range: 45–77 years) 1.5-T Signa MRI
64-MDCT scanCriterion was not defined TM was 52% and 77% and BM was 55% and 63% during FVC for healthy and COPD patients, respectively MRI was found to be a technically feasible alternative to MDCT for assessing TBM Nygaard et al. 2017 [30] Retrospective single-centre study
To compare four different image analysis methods for the diagnosis of tracheal collapse using MDCT353 patients (males (n=150), females (n=191), mean age: 60 years, age range: 18–88 years) with respiratory diseases (e.g. COPD, ILD, bronchiectasis) 64-MDCT scan LAC >50% and >80% reduction in the CSA LAC prevalence was ∼15.1% when using >50% as a threshold The different image analysis methods identified LAC in different patients. Thus, the diagnosis of LAC should not solely rely on MDCT images Leong et al. 2017 [6] Prospective single-centre study
To explore the prevalence of ECAC in stable and acute exacerbations COPD (AECOPD) patients40 COPD patients (males (n=19), females (n=21); age: 70.1±8.2 years); 64 AECOPD (males (n=40), females (n=24); age: 70.2±11.6 years); 53 healthy volunteers (males (n=35), females (n=18); age: 56.6±16.9 years) 320-slice dynamic MDCT LAC >50%, >75% and >80% reduction in the CSA were compared ECAC was observed in 35% of COPD, 39% of AECOPD and no healthy individuals when a >50% was used as a criterion ECAC can be present in up to one third of patients with stable COPD, and the abnormality does not seem to be worsened during AECOPD Bhatt et al. 2016 [44] Retrospective multicentre study
Assessing the association of ECAC to lung disease in smokers8820 ex- or active smokers (43.7% had COPD and 16.6% had asthma (males (n=4667), females (n=4153); mean age: 59.7 ±6.9 years)) CT scan ECAC ≥50% reduction in CSA ECAC prevalence was 5% in ex- or active smokers and 5.9% in participants with COPD (n=229/3856) The presence of ECAC was associated with worse respiratory quality of life in current or former smokers Sindhwani et al. 2016 [34] Prospective single-centre study
To assess expiratory wheeze in patients with obstructive airway disorders25 patients (males (n=14), females (n=11), mean age: 62.7±7.81 years) with COPD CT scan TBM/EDAC ≥50% reduction of the airway lumen TBM/EDAC was found in 40% of COPD patients Findings indicate value of screening patients with obstructive airway disease for TBM/EDAC El Sorougi et al. 2016 [33] Prospective single-centre study
To determine the prevalence of TM in COPD patients30 patients with COPD (demographics were not reported) 64-MDCT scan TM ≥50% in the tracheal lumen CSA 20% of COPD patients showed evidence of TM A significant proportion of patients with COPD had features consistent with TM on dynamic CT scanning Weinstein et al. 2016 [52] Prospective single-centre study
To describe the imaging characteristics of people presenting exertional dyspnoea6 military personnel (males (n=5), females (n=1), mean age: 39.5 years, age range: 24 to 53 years) with no underlying lung disease CT scan
Bronchoscopy at rest and during exercise (cycling; n=2).EDAC ≥75% reduction of the airway lumen EDAC was detected on expiratory images during dynamic CT (n=2) EDAC may explain “unexplained” exertional dyspnoea and wheeze in military recruits Represas-Represas et al. 2015 [43] Prospective single-centre study
To investigate the prevalence of EDAC in COPD53 patients (males (n=46), females (n=7), mean age: 65±9 years) with COPD Helicoidal MDCT EDAC >50% reduction in CSA Prevalence of EDAC was 9.4% EDAC in COPD patients is independent of disease severity and may not relate to symptoms O’Donnell et al. 2014 [25]¶ Prospective single-centre study
To determine the tracheal collapse in COPD patients67 patients (males (n=38), females (n=29); age: 65.1±6.5 years) with COPD 64-detector row CT scan Tracheal collapse ≥80% reduction in CSA Average forced expiratory collapse (62±16%) was greater to end-expiratory collapse (17±18%) COPD patients display a wide range of tracheal collapse at end-expiration Wielpütz et al. 2014 [53] Prospective single-centre study
To assess the feasibility of low-dose MDCT3 patients (3 males; mean age: 63.3 years) with COPD 4D MDCT scan TM criterion was not reported EDAC (n=1), sabre-sheath trachea and TBM (n=1), as well as tracheal stenosis (n=1) were demonstrated Low-dose MDCT may have equal diagnostic impact as bronchoscopy for tracheal instability Boiselle et al. 2013 [54] Prospective single-centre study
To assess the tracheal collapse in morbidly obese, non-morbidly obese and normal weight COPD patients100 patients (males (n=52), females (n=48),
mean age: 65±7 years) with COPD64-detector CT scan LAC criterion was not reported Expiratory collapse was directly associated
with BMI (p=0.002)Obesity is positively correlated with the degree of expiratory tracheal collapse
among COPD patientsO’Donnell et al. 2012 [40]# Prospective single-centre study
To explore the association between forced expiratory tracheal collapse and age or sex81 healthy volunteers (males (n=41), females (n=40); age: 47±17 years) 64-detector-row CT scan Tracheal collapse≥80% reduction in CSA The mean % collapse was similar for males (55±23%) and females (52±17%). The mean % collapse was correlated to age (r2 = 0.40, p< 0.001) in males Age and sex should be considered when assessing forced expiratory airway collapse for suspected TM Boiselle et al. 2012 [24]¶ Prospective single-centre study
To determine the prevalence of tracheal collapse in COPD patients100 patients (males (n=52), females (n=48); age: 65±7 years) with COPD 64-detector-row CT scan Tracheal collapse ≥80% reduction in CSA Prevalence of TM was found in 20 participants (20%) TM is observed in a subset of patients with COPD, but the magnitude of collapse is independent of disease severity Boiselle et al. 2010 [32] Prospective single-centre study
To assess the reproducibility of MDCT in measuring TM in healthy volunteers over time14 healthy volunteers (males (n=6), females (n=8), mean age: 48.7 ±13.8 years) 64-MDCT scan TM criterion was not reported 1st and 2nd year measures of tracheal collapse were strongly associated (r2=0.98, p<0.001) MDCT measurements of forced expiratory
tracheal collapse in healthy volunteers is highly reproducible
over timeLitmanovich et al. 2010 [26]# Prospective single-centre study
To assess the forced expiratory bronchial collapsibility in healthy volunteers51 healthy volunteers (males (n=25), females (n=26); age: 50±15 years) 64-detector row MDCT scan Expiratory reduction in CSA of >50% and >80%, were both used 73% of participants met the criterion (>50%) in one or both bronchi The current data suggest the need for more rigorous criteria for the diagnosis of BM Wagnetz et al. 2010 [28] Prospective single-centre study
To establish the use of a novel MDCT for the evaluation of TM6 patients (males (n=5), females (n=1); mean age: 53 years, age range: 37 to 70 years) with suspected TM (medical history was not reported) 320-row MDCT scan and fibreoptic bronchoscopy TM/TBM≥50% reduction in CSA All patients demonstrated TM/TBM with varying degrees of airway collapse (50% to >90% of the CSA) The 4D MDCT, isotropic, isovolumetric and isophasic, of the central airway is promising for the diagnosis of TM/TBM Boiselle et al. 2009 [14]# Prospective single-centre study
To assess the tracheal collapsibility in healthy volunteers51 healthy volunteers (males (n=25), females (n=26); age: 50±15 years) 64-detector row MDCT scan Expiratory reduction in CSA of >50% 78% of healthy volunteers exceeded the current diagnostic criterion for TM This study emphasises the need for a more rigorous diagnostic criterion to prevent overdiagnosis of TM McDermott et al. 2009 [39] Prospective single-centre study
To determine the prevalence and severity of TM in adults with CF40 patients (males (n=22), females (n=18); mean age: 28±8, age range: 18–54) with CF and 10 controls Dynamic cine MDCT with 64-detector row TM >50% or >75% reduction in CSA during cough TM was found in 69% of patients with CF during forced expiration and in 29% during coughing TM depicted at dynamic cine MDCT is a highly prevalent finding in patients with CF Inoue et al. 2009 [45] Retrospective single-centre study
To evaluate the frequency of TBM associated with PE56 patients (males (n=55), females (n=1); mean age: 68.9 years, age range: 49–87 years) with PE MDCT scanner with two-detector row TBM ≥50% decrease in CSA Four (7.1%) patients were diagnosed as having TM or BM TBM might be under- diagnosed in some patients with PE when using the standard criterion (e.g. ≥50%) Ochs et al. 2009 [46] Retrospective multicentre study
To investigate the prevalence of TM in an emphysema cohort431 patients (males (n=267, mean age: 64 years, range: 41 to 76), females (n=164, mean age: 62 years, range: 41 to 76)) CT scan LAC ≥50%, and >70% in the CSA Prevalence of TM was found in 13.4% participants based on ≥50% criterion A large degree of tracheal collapse can be found at end-expiration in patients with emphysema Ferretti et al. 2008 [27] Prospective single-centre study
To compare dynamic and end-expiratory imaging to assess LAC in patients with suspected TBM70 patients (males (n=43), females (n=27); mean age: 57 years, age range: 12–79 years) with respiratory conditions (e.g. COPD) 16-detector row helical CT scan TBM was not defined TBM was not found at the end of expiration, but its prevalence was 13% during dynamic expiration Dynamic expiratory CT demonstrates a greater degree of LAC than the end-expiratory acquisition in patients with suspected TBM Lee et al. 2007 [50] Retrospective single-centre study
To compare the dynamic expiratory CT against bronchoscopy for detecting airway malacia29 patients (males (n=12), females (n=17), mean age: 60 years, age range: 36 to 79 years) with COPD and relapsing polychondritis MDCT helical scan LAC >50% reduction in CSA CT findings were concordant with bronchoscopy in 97% of patients CT is a highly sensitive method for detecting airway malacia and could serve as an effective, noninvasive test for diagnosing LAC Boiselle et al. 2006 [20] Prospective single-centre study
To describe the technical aspects of using 64-MDCT during coughing17 patients (males (n=6), females (n=11), age range: 62.4 years) with suspected TM 64-MDCT scan TM >50% reduction in CSA during coughing 64-MDCT during a coughing protocol was technically successful in 94% of patients 64-MDCT is technically feasible and has the potential to make significant contributions to the noninvasive diagnosis of TM Lee et al. 2006 [55] Retrospective single-centre study
To assess the prevalence of expiratory CT abnormalities, including malacia18 patients (males (n=3), females (n=15), mean age: 47 years; age range: 20–71 years) with relapsing polychondritis Helical MDCT LAC >50% reduction in CSA CT abnormalities were present in 94% and airway malacia in 72% of patients Dynamic expiratory CT should be considered a standard component of airway evaluation in patients with relapsing polychondritis Nishino et al. 2006 [36] Prospective single-centre study
To evaluate the frequency and severity of BM46 patients (males (n=10), females (n=36), mean age: 64 years, age range: 44–84 years) with bronchiectasis Volumetric high-resolution 4- or 8-detector CT LAC ≥50% reduction in the CSA Prevalence of BM was found in 70% of patients at end-expiration Air trapping in bronchiectasis might be greater in bronchiectasis patients with BM compared to those without Baroni et al. 2005 [38] Retrospective single-centre study
To compare the dynamic- and end-expiratory CT in assessing LAC14 patients (males (n=11), females (n=3), mean age 53 years old and age range: 19–79 years) with various conditions Eight-detector row helical CT scan LAC ≥50% reduction in the CSA Collapse was greater in dynamic expiration than in end-expiration (p<0.004) The reliance on end-expiratory imaging alone might result in a high level of false-negative results Baroni et al. 2005 [37] Prospective single-centre study
To describe the role of pre- and post-operative dynamic CT in patients undergoing tracheoplasty5 patients (males (n=4), woman (n=1); mean age: 62, age range: 56–78) 8-MDCT helical scan TBM ≥50% reduction in the CSA Tracheal collapse was found to be 58.9% pre- and 26.9% post-operatively during dynamic expiration Dynamic expiratory CT is a potentially valuable tool in the pre- and post-operative evaluations of patients undergoing tracheoplasty Nishino et al. 2005 [35] Prospective single-centre study
To investigate the frequency of BM associated with sarcoidosis18 patients (males (n=6), females (n=12); mean age: 47 years, age range: 29–64 years) with pulmonary sarcoidosis High-Resolution CT LAC >50% reduction in CSA BM was found in 61% of patients BM is frequently associated with sarcoidosis Heussel et al. 2004 [42] Prospective single-centre study
To assess the respiratory lumen diameter, change in the tracheal level during continuous respiration38 subjects, 23 patients with COPD (age: 59 years, age range: 41–68 years) and 15 healthy adults (age: 62 years, age range: 48 to 74 years) Cine-MRI LAC >50% reduction in CSA A pathological collapse occurred in 33% of volunteers and in 69.6% of patients with COPD The airway collapse is significantly larger in patients with COPD compared to volunteers Hasegawa et al. 2003 [21] Retrospective single-centre study
To determine the frequency of TM incidentally detected on CT pulmonary angiography (CTPA)163 (73
males (n=73), females (n=90); mean age: 60 years) with suspected pulmonary embolismSingle detector CT and MDCT (with 4 and 8 detectors) TM ≥50% decrease in tracheal lumen Prevalence of TM was found in 10% of the participants with suspected pulmonary embolism TM is a relatively common finding in CTPA when assessing patients with suspected pulmonary embolism Zhang et al. 2003 [3] Prospective single-centre study
To compare standard- and low-dose CT images assessing tracheal lumen10 patients (males (n=5), females (n=5), mean age: 56 ±11 years) with bronchoscopically proved TBM Multi-section helical MDCT scan LAC >50% reduction in the CSA TBM was found in all 10 patients Paired inspiratory and dynamic expiratory CT images is a promising method for diagnosing TBM Aquino et al. 2001 [56] Retrospective and prospective single-centre study
To explore the measurements of the trachea between inspiration and end-expiration on CT10 TM patients (males (n=6), females (n=4); mean age: 60 years, age range: 42 to 84 years) and 23 normal control patients (males (n=15), females (n=8); mean age: 40 years, age range: 27 to 57 years) CT scan Diagnostic criterion for TM was not reported Collapsibility in tracheal CSA was significantly greater in patients with TM (1.9±0.9 cm2) compared to controls (2.4±0.6 cm2) during end-expiration Patients with TM demonstrate a higher airway collapse compared to controls Gilkeson et al. 2001 [4] Prospective single-centre study
To examine the role of dynamic inspiratory-expiratory imaging with MDCT in patients with suspected TBM13 patients (males (n=7), females (n=6); mean age: 49 years and age range: 14–88 years) with respiratory conditions (e.g. asthma, chronic cough, smoking) MDCT scan, bronchoscopy LAC >50% reduction in the CSA All patients showed evidence of TBM of different degrees, 50–75% (n=3) 75–100% (n=7), and 100% (n=3) MDCT with inspiratory-expiratory imaging is a promising method in the evaluation of patients with suspected TBM Heussel et al. 2001 [22] Prospective (including retrospective analysis) single-centre study
To compare CT, MRI bronchoscopy, in the diagnosis of LAC29 patients (males (n=10), females (n=19); mean age: 61 years, age range: 27–82 years) with suspicion of or previously bronchoscopically verified tracheal collapse CT scans (spiral and cine), cine-MRI, bronchoscopy ≥50% collapse of the CSA Bronchoscopy correlated with cine CT. MRI demonstrated similar time curves of tracheal CSA to cine CT Cine CT is able to obtain significantly improved evaluation of respiratory collapse. Cine-MRI promises functional information due to free choice of imaging plane Suto & Tanabe, 1998 [41] Prospective single-centre study
To evaluate tracheal collapsibility during coughing in patients with TM who underwent MRI6 patients (males (n=4), females (n=2); mean age: 40 years, age range: 44 to 68 years) with suspected TBM and 13 healthy volunteers (males (n=10), females (n=3); mean age: 40 years, age range: 17 to 63 years) 1.5-T superconducting MRI system Diagnostic criterion for TM was not reported Collapse was 30±13% and 50±15% in forced expiration, and 38±16% and 75±12% during coughing in healthy and patients with TM, respectively Collapsibility during forced expiration-inspiration and collapsibility during coughing was not significant in patients with TM during MRI Stern et al. 1993 [57] Prospective single-centre study
To define the range of intrathoracic tracheal diameters and CSA during forced respiration10 healthy volunteers (males (n=10), age range: 24–31 years) CT using the model C-100 scanner TM >70% reduction in the CSA Trachea significantly decreased (p<0.001) from end-inspiration (280 mm2) to end-expiration (178 mm2) Intrathoracic tracheal shape, sagittal and coronal diameters, and CSA can vary greatly during a forced respiration #The studies by Litmanovich et al. 2010 and Boiselle et al. 2009 were not analysed as part of the main results as the participants of both studies were included in O'Donnell et al. 2012. ¶The study by Boiselle et al. 2013 was not analysed as part of the main results as the participants were included in O'Donnell et al. 2014. TBM: tracheobronchomalacia; GERD: gastro-oesophageal reflux disease; OSA: obstructive sleep apnoea; MDCT: multi-detector CT; LAC: large airway collapse; CSA: cross-sectional area; EDAC: excessive dynamic airway collapse; CT: computed tomography; TM: tracheomalacia; MRI: magnetic resonance imaging; BM: bronchomalacia; FVC: forced vital capacity; ILD: interstitial lung disease; ECAC: excessive central airway collapse; CF: cystic fibrosis; PE: pulmonary emphysema; CTPA: pulmonary angiography.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00055-2021.SUPPLEMENT
Supplementary material Online_Supplement_LACS










