





Figures
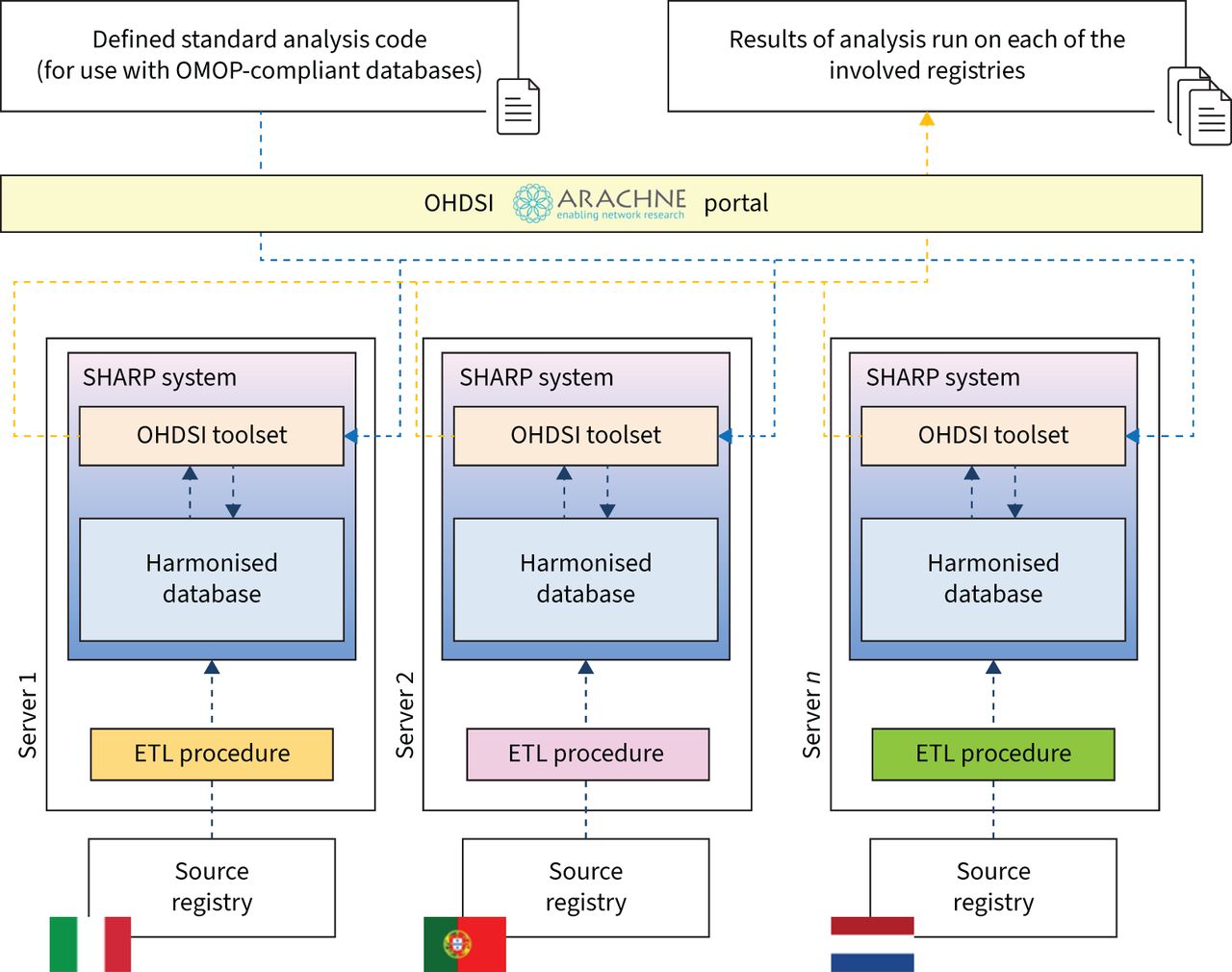
- FIGURE 1
Architecture of the federated analysis platform. Field names of the different national registries are mapped to concepts in the Observational Health Data Sciences and Informatics (OHDSI)/Observational Medical Outcomes Partnership (OMOP) Common Data Model. An Extract, Transform, Load (ETL) procedure is created to automate the mapping from the local database into a unified format; the harmonised data are made available for local analysis using the OHDSI toolset or R code; an identical analysis is run on each registry; the results are combined using federated analysis tools. SHARP: Severe Heterogeneous Asthma Research collaboration, Patient-centred.
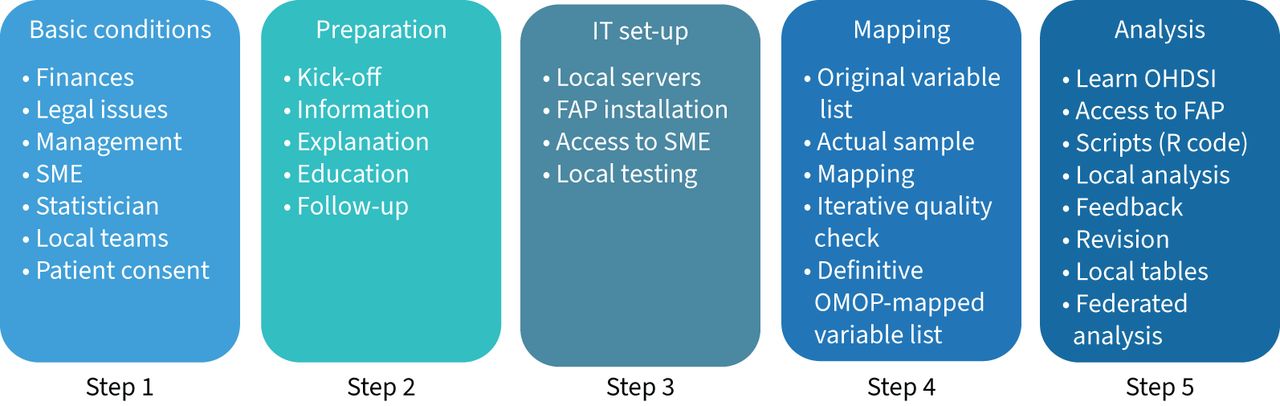
- FIGURE 2
Schematic summary of steps to be taken for a successful harmonisation process of local nonstandardised disease registries to the Observational Health Data Sciences and Informatics (OHDSI)/Observational Medical Outcomes Partnership (OMOP) Common Data Model for federated analyses. SME: small and medium-sized enterprise; IT: information technology; FAP: federated analysis platform.


{kind=link}
{kind=link}
Tables
- TABLE 1
Blueprint for harmonising disease registries using the Observational Heath Data Sciences and Informatics (OHDSI)/Observational Medical Outcomes Partnership (OMOP) Common Data Model (CDM)
Topic Recommendations Basic conditions • Selection of a legal body for CRC • Securing sufficient financial resources for ≥3 years • Appointment of a full-time dedicated project manager • Establishment of a contract with an SME specialising in OHDSI, OMOP CDM and mapping • Establishment of a contract with a hands-on statistician with programming skills • Written confirmation from each registry that patients have given written consent to use their medical data for (international) clinical research • Identification for each local registry of named individuals in the following roles: registry owner, legal officer, clinical expert, source data expert IT contact/administrator, translator of medical terminology and platform/system user • Conclusion of collaboration agreements between CRC and registries Conceptual aspects • Production of a document and a PowerPoint presentation explaining the OHDSI/OMOP CDM and the federated approach to all stakeholders • Organisation of a plenary kick-off meeting with all stakeholders • Organisation of regular team meetings for each registry to monitor progress Technical aspects • Provision/hire of a dedicated Linux server for each registry (local data centre or cloud environment) for the installation and set-up of the FAP, with access to a local copy of the source database • Provision to all required parties of access to the Linux registry servers • Testing of the functioning of the FAP on local Linux servers by SME Mapping aspects • Checks source data quality • Provision of registry data dictionary to SME by source data experts • Provision of a representative, but anonymised registry data sample by local team to smoothen the ETL process and avoid “black box mapping” • Assistance by clinical experts in optimising the mapping • Provision by SME to statistician(s) of a codebook of the variables mapped Analytical aspects and quality control • Learning by statistician(s) on the principles of OHDSI and OMOP CDM • Provision by SME of access to the FAP for statistician(s) • Creation by statistician of scripts in R (or OHDSI tools) for the production of descriptive summary statistics • Execution by local analyst in each country of the pre-written R script via the FAP • Checks by clinicians on the validity of the output and provision of feedback to statistician and SME • Revision by source data expert and SME of any mapping issues • Creation of a second round of data summaries and a repeat of the quality control process • Production of final OHDSI/OMOP CDM tables Research studies • Creation of research protocol, and approval by CRC, local clinical experts and registry owners • Identification of dedicated local teams for each registry, comprising clinical experts, source data experts and data analysts • Creation of a formal analysis plan by statistician, for review and approval by representatives of all participating registries • Creation by statistician of analysis scripts in R (or OHDSI tools) • Execution by local data analysts of pre-written scripts in R (or OHDSI tools) using the FAP • Fostering of collaboration between best practices for statisticians and data analysts via workshops to discuss issues such as imputation rules, filters and exclusions • Production of final statistical tables and graphics for each registry singly, according to the analysis plan • Meta-analysis by statistician of summary statistics from all registries • Writing and submission of manuscript CRC: clinical research collaboration; SME: small and medium-sized enterprise; IT: information technology; FAP: federated analysis platform; ETL: Extract, Transform, Load.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00168-2022.SUPPLEMENT










