





Figures
- FIGURE 1
Structure of the nontuberculous mycobacteria lung transplant Delphi study.
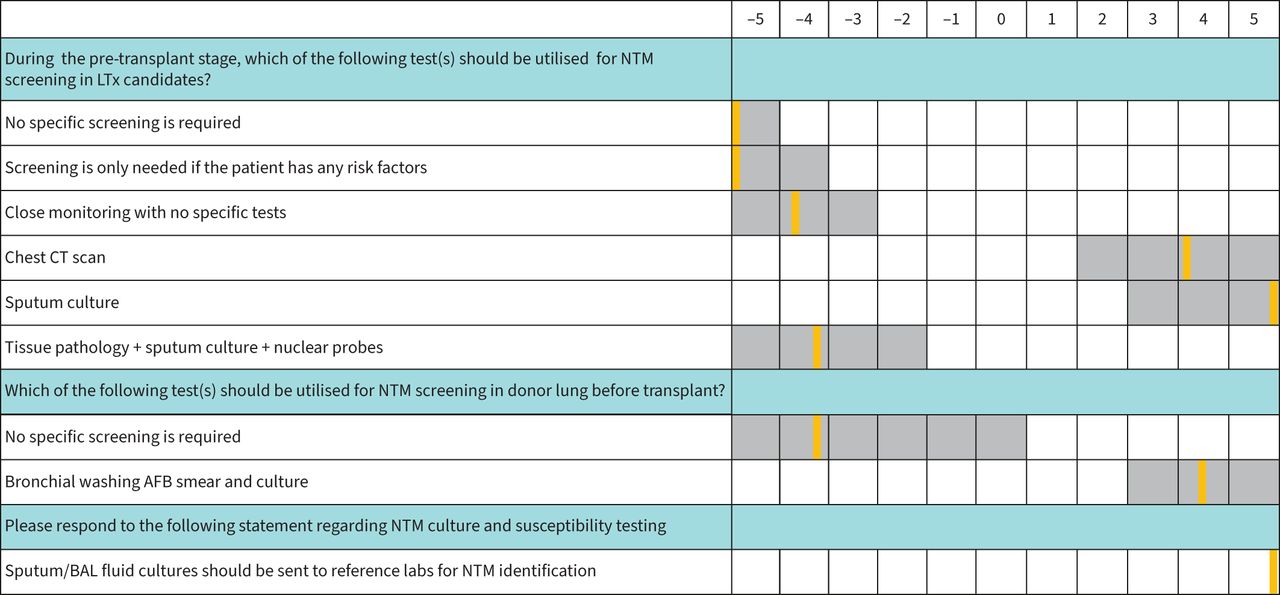
- FIGURE 2
Summary of consensus on statements addressing diagnostic modalities for pre-transplant nontuberculous mycobacteria (NTM) pulmonary disease. The grey and orange colours represent the range and median on a Likert scale of 11 points (5 to −5). A median rating >4 or <−4 indicates for or against the given statement, respectively. LTx: lung transplant; CT: computed tomography; AFB: acid-fast bacilli; BAL: bronchoalveolar lavage.
- FIGURE 3
Summary of consensus on statements addressing transplant listing criteria in patients with nontuberculous mycobacteria (NTM) pulmonary disease. The grey and orange colours represent the range and median on a Likert scale of 11 points (5 to −5). A median rating >4 or <−4 indicates for or against the given statement, respectively. MAC: Mycobacterium avium complex; LTx: lung transplant.
- FIGURE 4
Summary of consensus on statements addressing pre-transplant management of nontuberculous mycobacteria (NTM) pulmonary disease. The grey and orange colours represent the range and median on a Likert scale of 11 points (5 to −5). A median rating >4 or < −4 indicates for or against the given statement, respectively. MAC: Mycobacterium avium complex; LTx: lung transplant.
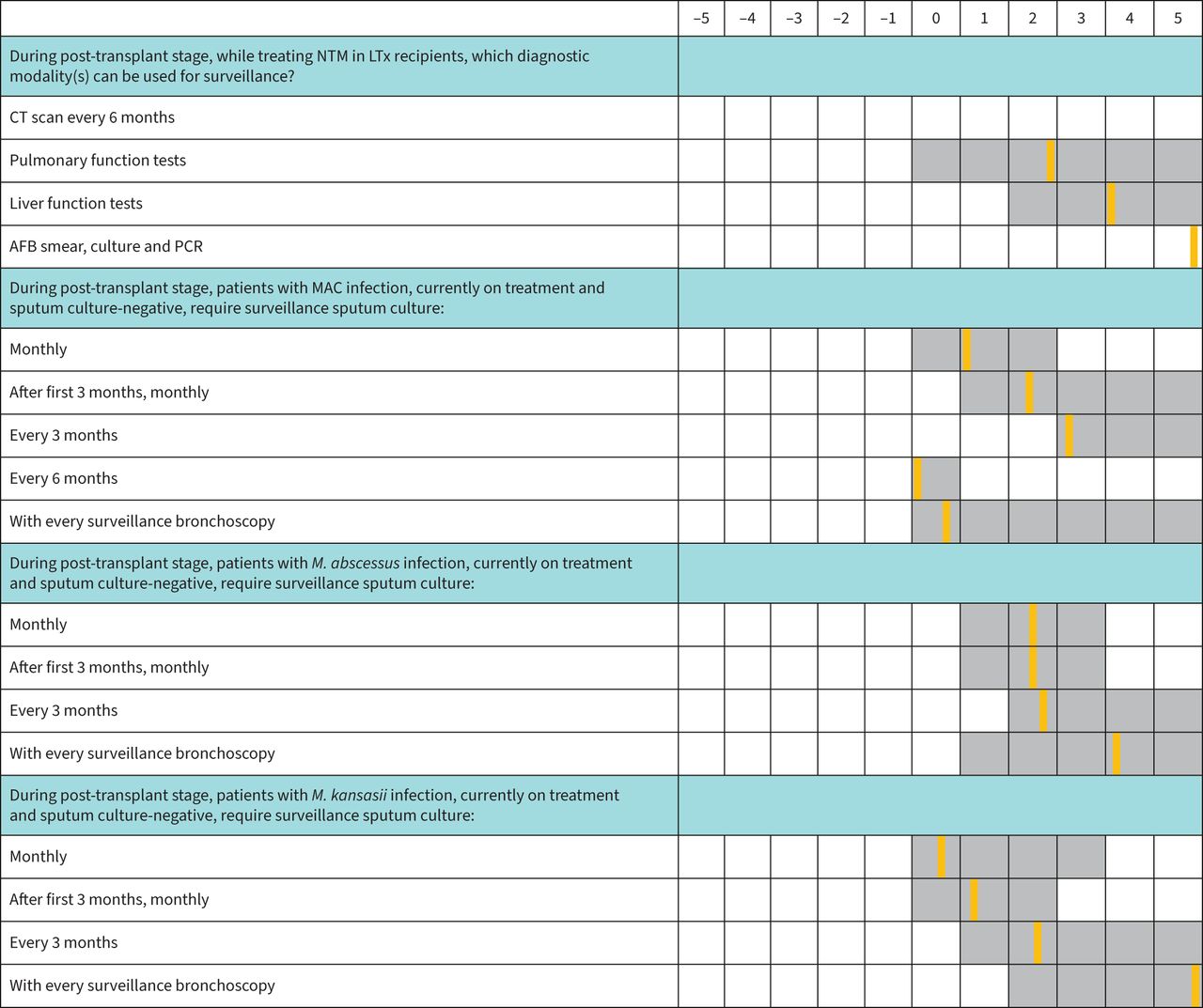
- FIGURE 5
Summary of consensus on statements addressing post-transplant surveillance for nontuberculous mycobacteria (NTM) pulmonary disease. The grey and orange colours represent the range and median on a Likert scale of 11 points (5 to −5). A median rating >4 or < −4 indicates for or against the given statement, respectively. LTx: lung transplant; CT: computed tomography; AFB: acid-fast bacilli; MAC: Mycobacterium avium complex.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Summary of key recommendations by experts
Diagnostic modalities for pre-transplant NTM pulmonary disease Chest CT scan and sputum culture are suggested for NTM screening in LTx candidates. Bronchial washing AFB smear and culture are suggested for NTM screening in donor lung before LTx. Sputum/BAL fluid cultures should be sent to reference labs for NTM identification and susceptibility testing. Transplant listing criteria in patients with NTM pulmonary disease Experts have different opinions about patients with MAC infection who are currently on treatment and sputum culture-negative. Some suggest LTx without further waiting, others recommend culture negativity for the past 6 or 12 months. Experts did not agree that LTx is contraindicated irrespective of culture status. Patients with M. abscessus infection who are currently on treatment and sputum culture-negative can be listed for lung transplant if the sputum culture has been negative for the past 12 months. Patients with M. kansasii infection who are currently on treatment and sputum culture-negative can be listed for lung transplant if the sputum culture has been negative for the past 6–12 months. Patients with a history of treated MAC and M. abscessus infection currently not on treatment and sputum culture-negative should be listed for lung transplant if treated 12 months ago, and 6 months ago in the patients with M. kansasii. In patients with past history of M. abscessus infection and currently negative sputum culture who are candidates for single LTx, to prevent NTM infection in allograft perform bilateral LTx. Pre-transplant management of NTM pulmonary disease Azithromycin, rifampin, amikacin and rifabutin are suggested as empiric antibiotic regimen in NTM non-cavitary disease pending speciation. The preferred antibiotic regimens in non-cavitary MAC include: ethambutol, rifampin, azithromycin and clarithromycin. The preferred antibiotic regimens in non-cavitary M. abscessus include: azithromycin and amikacin. The preferred antibiotic regimens in non-cavitary M. kansasii include: azithromycin, ethambutol and rifampin. The recommended frequency of antibiotic therapy for MAC and M. abscessus is daily treatment. Post-transplant surveillance for NTM pulmonary disease AFB smear, culture, PCR and liver function tests can be used for surveillance while treating NTM in LTx recipients. Patients with M. abscessus and M. kansasii infections currently on treatment and negative sputum culture require surveillance sputum cultures with every surveillance bronchoscopy. Post-transplant management of NTM pulmonary disease Clarithromycin and azithromycin are the most commonly preferred empiric antibiotic regimens (no identification yet) in non-cavitary disease. Some panellists suggest no empiric treatment. The preferred antibiotic regimens in non-cavitary MAC include: ethambutol, rifampin, azithromycin and clarithromycin. In macrolide resistant patients, rifabutin and ethambutol are recommended. The preferred antibiotic regimens in non-cavitary M. abscessus include: azithromycin, amikacin and imipenem. The preferred antibiotic regimen in non-cavitary M. kansasii is rifabutin. In the post-transplant stage, a dose reduction of immunosuppressive treatment is recommended if M. abscessus is isolated. NTM: nontuberculous mycobacteria; CT: computed tomography; LTx: lung transplant; AFB: acid-fast bacilli; BAL: bronchoalveolar lavage; MAC: Mycobacterium avium complex.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00377-2022.SUPPLEMENT










