Article Text

Abstract
Background and objective While paracetamol exposure in pregnancy and early infancy has been associated with asthma, it remains unclear whether this is confounded by respiratory tract infections, which have been suggested as an alternative explanation. We undertook a systematic review and meta-analysis of longitudinal studies that reported the association between paracetamol exposure during pregnancy or infancy and the subsequent development of childhood asthma (≥5 years).
Methods Two independent researchers searched the databases EMBASE and PUBMED on 12 August 2013 for relevant articles using predefined inclusion and exclusion criteria. Study quality was assessed and results were pooled using fixed effect models or random effect models when moderate between-study heterogeneity was observed. We explicitly assessed whether the observed associations are due to confounding by respiratory tract infections.
Results Eleven observational cohort studies met the inclusion criteria. Any paracetamol use during the first trimester was related to increased risk of childhood asthma (5 studies, pooled OR=1.39, 95% CI 1.01 to 1.91) but there was marked between-study heterogeneity (I2=63%) and only one of these studies adjusted for maternal respiratory tract infections. Increasing frequency of use of paracetamol during infancy was associated with increased odds of childhood asthma (3 studies, pooled OR=1.15, 95% CI 1.00 to 1.31 per doubling of days exposure), but in these same three studies adjusting for respiratory tract infections reduced this association (OR=1.06, 95% CI 0.92 to 1.22).
Discussion The association during early pregnancy exposure was highly variable between studies and exposure during infancy appears to be moderately confounded by respiratory tract infections. There is insufficient evidence to warrant changing guidelines on early life paracetamol exposure at this time.
- Allergy
- Epidemiology
Statistics from Altmetric.com
What is already known on this topic
Use of paracetamol in pregnancy and early life has been implicated as a cause of asthma, leading some to question the continued use of paracetamol.
Paracetamol is commonly used to treat respiratory tract infections, a known risk factor for childhood asthma.
It remains unclear if paracetamol causes asthma, or whether the observed association is due to confounding by respiratory tract infections.
What this study adds
This review demonstrated that the association between paracetamol exposure in pregnancy and childhood asthma varies greatly between studies for unknown reasons.
While paracetamol use in infancy is associated with an increased risk of asthma later in childhood, this appears to be confounded by respiratory tract infections.
Introduction
Asthma is a chronic condition affecting some 300 million people worldwide and is characterised by episodes of breathlessness, chest tightness and reduced quality of life.1 There has been an increase in global levels of asthma and observational studies have tried to identify the causes of this rising prevalence.2 Increasing pollution levels,3 obesity, dietary change,4 ,5 and the hygiene effect6 have been identified as possible risk factors, although the evidence to support these remains controversial.7–9
Paracetamol, a widely used analgesic and antipyretic, has historically been considered to be safe in both pregnancy and young children. However, paracetamol has recently been identified as a possible cause for the current asthma epidemic.10 Paracetamol replaced aspirin as analgesic of choice in the 1990s when aspirin was found to be associated with Reyes syndrome.11 An ecological study demonstrated that increasing use of paracetamol was associated with increasing prevalence of asthma.12 Cohort studies have also demonstrated that paracetamol exposure is associated with an increased incidence of asthma.13–15 Induction of asthma by paracetamol is biologically plausible, as paracetamol has been found to deplete glutathione, a key airway antioxidant.16 Given this accumulating evidence of association, the high burden of disease caused by asthma, and the prevalence of use of paracetamol, the continued use of paracetamol, particularly in paediatric medicine has been questioned.17
An alternative explanation for the paracetamol/asthma association is that it is due to confounding by indication. Fever and pain caused by respiratory tract infections leads to increased paracetamol use,18 and it is well established that early life respiratory tract infections, particularly those caused by rhinoviruses and respiratory syncytial viruses,19 are associated with asthma. Furthermore, both recurrent maternal colds20 and febrile infection21 during pregnancy have been associated with increased risk of asthma in the child. The uncertainty concerning the paracetamol–asthma association has led to numerous calls for randomised control trials (RCTs) to be conducted,22–24 however a search of clinical trials websites reveals that no RCTs are currently underway to assess whether use of paracetamol in pregnancy or infancy causes asthma. Given the ethical and logistical concerns, an effective trial to address this issue may never be conducted, making balanced interpretation of the results from high quality cohort studies essential.
The purpose of this review was to evaluate the available evidence from cohort studies on the association between paracetamol exposure and asthma in childhood. To do this, we have: (1) included only studies of childhood asthma after the age of 5 years, as diagnosis of asthma before this age is problematic25; and (2) examined the evidence that any association could be due to confounding by respiratory tract infections by comparing crude and adjusted associations separately, both of which previous reviews on this topic have failed to do. Lower ORs after adjusting for respiratory tract infections would suggest that the association between paracetamol and asthma is confounded by respiratory tract infections.
Methods
We performed a systematic review of published studies and a meta-analysis of longitudinal studies, either observational or controlled trials, according to the MOOSE26 and PRISMA27 guidelines.
Search strategy
A systematic search for journal articles written in English was conducted using the medical databases EMBASE from January 1971 to August 2013, and PUBMED from January 1967 to August 2013. The search strategy in PUBMED was developed from the MeSH terms ‘acetaminophen’ and ‘asthma’, while the search strategy in EMBASE was developed from the terms ‘paracetamol and asthma’ according to the interfaces of the databases, that is, PUBMED using MeSH headings and EMBASE using advanced search options (see online supplement). Search results were compared to previous systematic reviews for completeness.
Inclusion/exclusion criteria
Prospective and retrospective longitudinal studies of incident asthma were included, while cross-sectional and case–control studies were excluded. To assess the effect of paracetamol exposure on the incidence of asthma, only studies that examined exposure to paracetamol during pregnancy and/or during the first 2 years of life, and included asthma outcomes after age 5 years were included in the review. The neonatal period up to the first 2 years of life is a critical stage for lung development,28 and exposures during this time window have the potential to have a substantial impact on respiratory health.
Outcome ascertainment needed to be established by doctor diagnosis, medical records or structured questionnaires. Finally, studies had to include some measure of association to be included in the meta-analysis, for example ORs. Non-English studies and studies not reporting original data (eg, reviews) were also excluded.
Data extraction
Two researchers (MC and Dian Xu) independently reviewed titles and abstracts, and where necessary full articles, to determine if they met the inclusion criteria as described above. There was agreement on all articles with regard to the inclusion criteria. For each study, information regarding authorship, year of publication, study population, country of study, study design, outcomes assessed was extracted. In addition the timeline at which measurement for paracetamol exposure took place was included in the data. If more than one category of paracetamol exposure was reported, all categories were included in the extracted data. Finally, information relating to confounding variables adjusted for in the studies was also extracted. Measures of association (ORs) and their 95% CIs were extracted using data reported in the publications. Where measures of associations were presented as risk ratios, these were taken as approximations of ORs provided the incident risk was less than 20%.29 Authors for one study30 were contacted and asked to re-analyse their data and present ORs.
Study quality assessment
Two authors (AJL and MC) used the Newcastle–Ottawa quality assessment scale (NOS) (online supplementary table S1) for cohort studies to guide the assessment of the quality of included studies. We chose only those domains that were most appropriate to the current topic.
Cohort studies evaluating the association between paracetamol and asthma in childhood
Statistical analysis
The odds of asthma in childhood after paracetamol intake during pregnancy or infancy were compared to the odds of asthma in childhood without exposure to paracetamol during the same time period. Both the unadjusted and adjusted estimates were extracted for each study, as well as what was adjusted for. The extracted estimates were stratified according to: (1) population exposed (expectant mother or infant); (2) trimester of pregnancy; (3) adjustment for respiratory tract infections; and (4) increasing use of paracetamol use and any use of paracetamol (for infancy analyses). Adjusted analyses combined different potential confounders including respiratory tract infections. Homogeneity between studies was assessed using the I2 statistic.31 Fixed effect (inverse variance) meta-analysis models were used when there was minimal evidence of heterogeneity in all subgroups, while random effect models were used if the I2 value was between 30% and 80% for one or more effect estimates. All analyses were conducted using Stata V.12.
Results
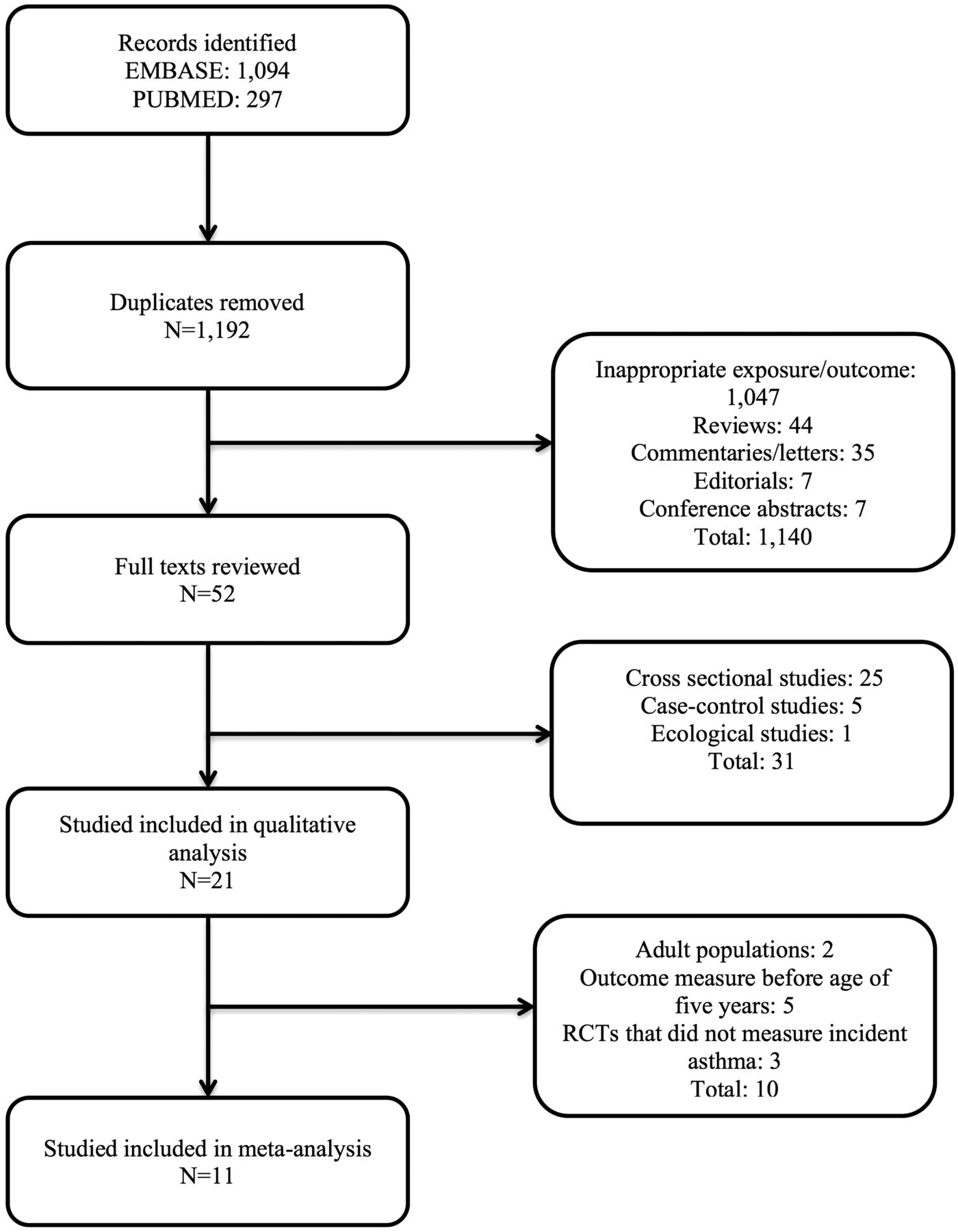
A total of 1192 citations were identified, and of these, 1140 studies were discarded after reviewing the titles and abstracts (figure 1, and see online supplementary table S2 for citations of all excluded studies), leaving 52 articles for full text review. A total of 31 studies were excluded on the basis of study design. Five cohort studies,23 ,32–35 that measured wheeze outcomes before the age of 5 years, two cohort studies that measured paracetamol exposure during adulthood,36 ,37 and three RCTs,38–40 that did not measure incident asthma were subsequently excluded. Of the remaining 11 studies (representing 10 cohorts) included in the meta-analysis, all were observational cohort studies, five measured paracetamol exposure during pregnancy,13 ,41–44 one measured exposure during both pregnancy and infancy,14 and five measured exposure during infancy15 ,30 ,45–47 (table 1). The age at which outcome of asthma was measured ranged from 5 to 10 years. Assessment of exposure was generally performed in an adequate manner, while adjustment for early childhood respiratory infections was more uniformly performed by those studies evaluating paracetamol exposure during infancy than pregnancy. More details concerning the quality assessment of the include studies can be found in the online supplementary table S1.

Flow chart of study identification.
Association between paracetamol exposure during pregnancy and asthma in the child
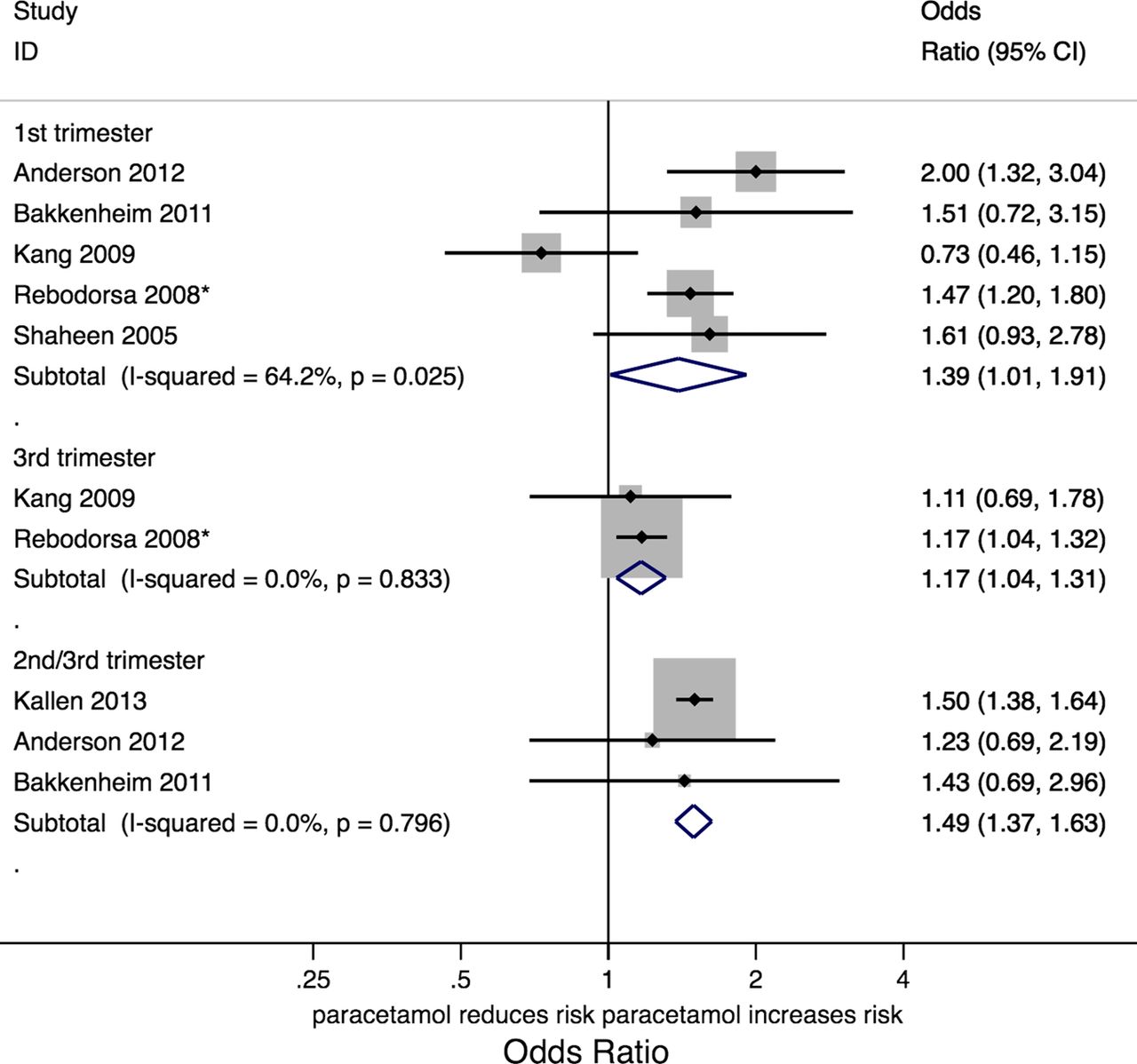
In the five studies reporting paracetamol exposure during the first trimester of pregnancy, there was an increased odds of asthma in children (pooled OR=1.39, 95% CI 1.01 to 1.91), however there was high between-study heterogeneity of this effect (I2=64.2%, p=0.03; figure 2). Only two studies examined paracetamol exposure during the second trimester of pregnancy and the results were quite disparate (OR=1.06, 95% CI 0.92 to 1.22 for one study43; and OR=2.15, 95% CI 1.18 to 3.91 for the other44; I2=80%, figure 3). A weak association between paracetamol exposure during the third trimester of pregnancy and childhood asthma was shown by two studies (pooled OR=1.17, 95% CI 1.04 to 1.31, figure 2), while the three other studies that examined paracetamol exposure during the second and third trimester showed a stronger association (pooled OR=1.49, 95% CI 1.37 to 1.63, figure 2). There was significant heterogeneity among the three studies that assessed associations with paracetamol use through the entire pregnancy (Andersen et al,13 OR=1.65, 95% CI 1.17 to 2.32; Rebordosa et al,43 OR=1.22, 95% CI 1.11 to 1.34; Kang et al,42 OR=0.74, 95% CI 0.5 to 1.09; I2=89%), so results were not pooled (figure 3).
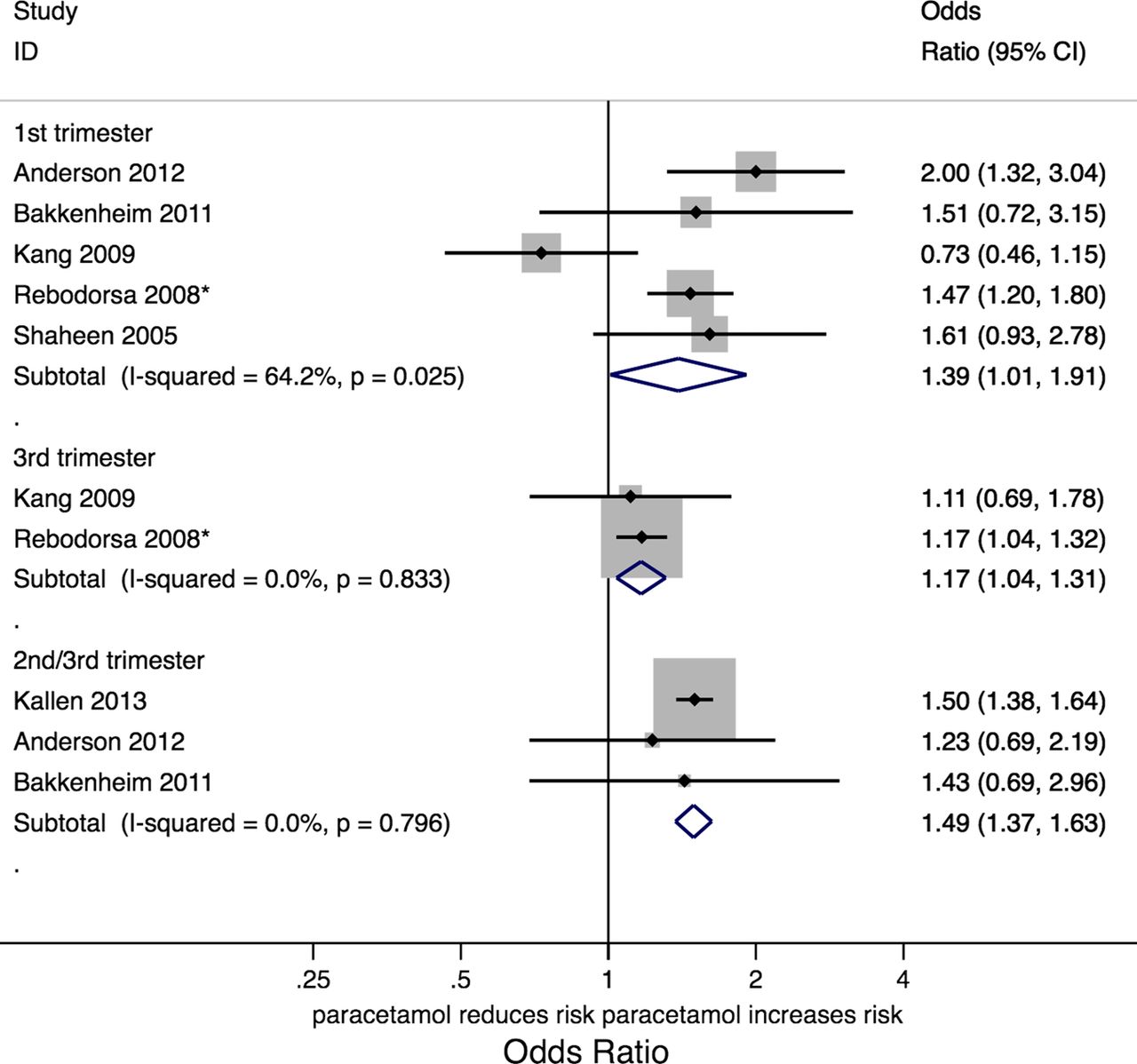
Crude association between paracetamol intake (any vs none) at various stages in pregnancy and asthma in childhood. Effects estimated using a random effects model. *Risk ratios used as approximations of ORs. p Value: test for homogeneity.

Crude association between paracetamol intake (any vs none) during second trimester and any use in pregnancy and asthma in childhood. *Risk ratios used as approximations of ORs.
Only one study adjusted for respiratory tract infections during pregnancy.44 It was found that adjusting for a range of factors, including respiratory tract infections, attenuated the association between paracetamol exposure in both early and late pregnancy and asthma in the child (see online supplementary figure S1). As a substantial number of variables were adjusted for, it is not clear what proportion of this attenuation of association was due to confounding by respiratory infections.
Association between paracetamol intake during infancy and asthma in childhood
Of the six studies that compared paracetamol intake up to the first 2 years of life and asthma outcomes, three classified paracetamol exposure according to frequency of intake (all expressing the results as per doubling of days of intake) (table 1). In the crude analysis there was a weak positive association between paracetamol intake during infancy and asthma in childhood (figure 4).

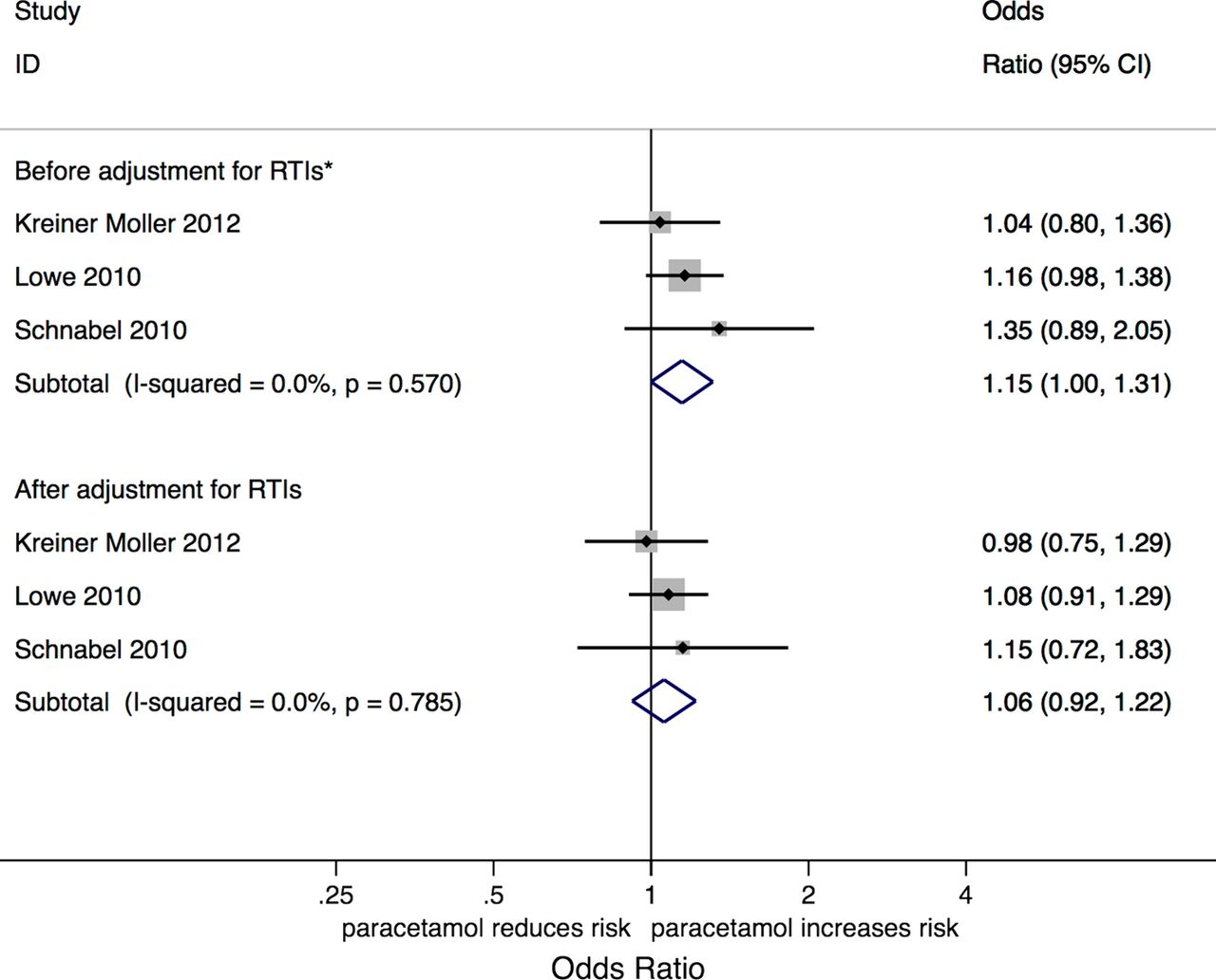
Association between frequency of paracetamol intake during infancy (expressed per doubling of days of exposure) and asthma in childhood before and after adjustments for respiratory tract infections. Effects estimated using fixed effects model. *Kreiner-Møller et al45—no adjustments. Lowe et al46—infant's sex, parental history of asthma, and presence of older siblings at time of birth. Schnabel et al30—gender, age at follow-up, parental history of asthma, study region. p Value: test for homogeneity.
Four studies compared asthma outcomes between children that did not take any paracetamol during the first 2 years of life and those that took any paracetamol during the same period; a weak positive association between any paracetamol intake and asthma was observed (pooled OR=1.22; 95% CI 1.11 to 1.34, see online supplementary figure S2).
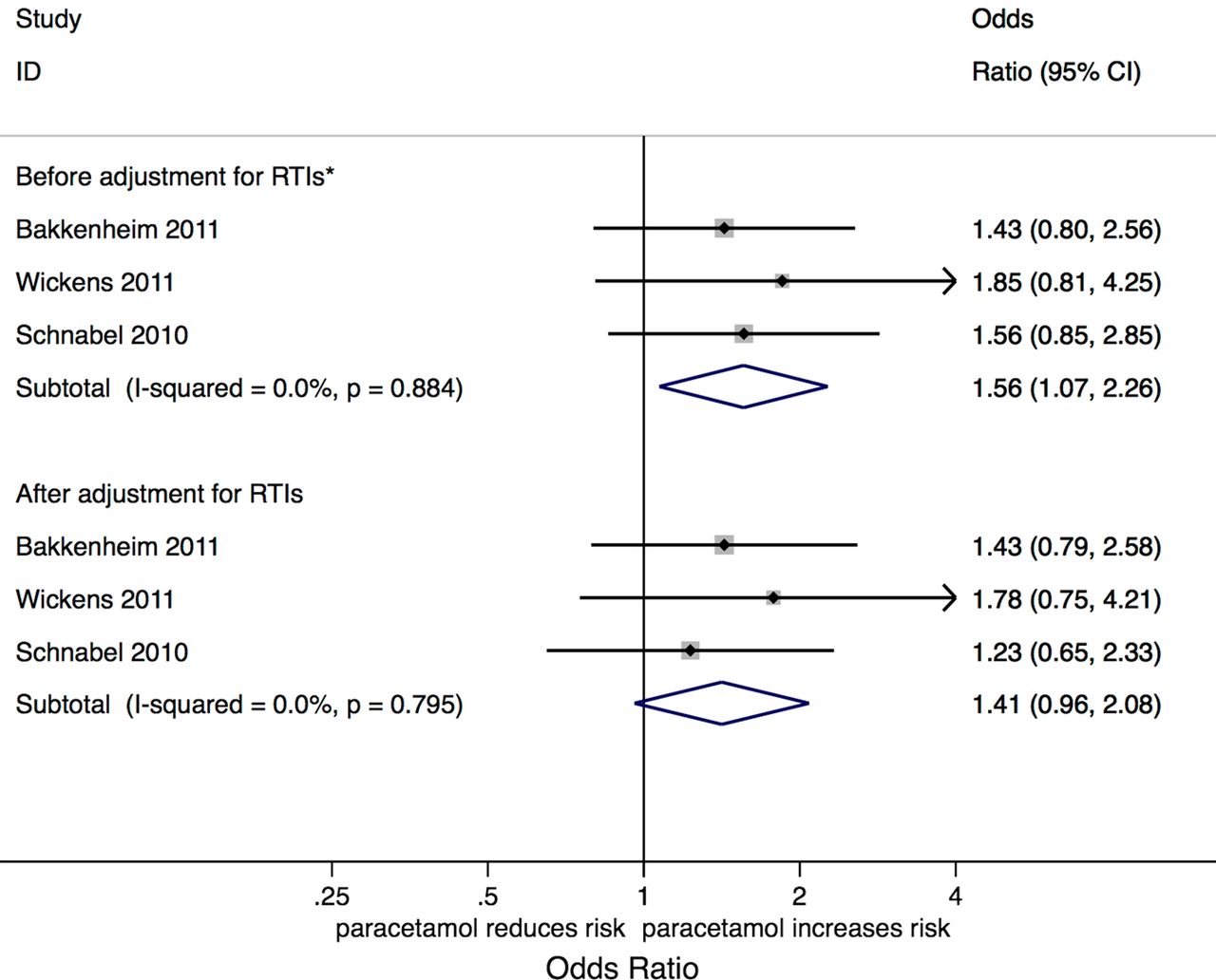
All but one of the studies47 examining the days of paracetamol exposure during infancy adjusted for respiratory tract infections in the child. However, it should be noted that some studies adjusted for other variables in addition to respiratory tract infections, which might have influenced the results. Adjusting for respiratory tract infections caused a moderate attenuation of the association between frequency of paracetamol intake and childhood asthma (unadjusted pooled OR=1.15, 95% CI 1.00 to 1.31; adjusted pooled OR=1.06, 95% CI 0.92 to 1.22; figure 4). Adjustment for respiratory tract infections also reduced the strength of association between any versus no paracetamol intake in infancy, in the three studies that reported both crude and adjusted results (crude pooled OR=1.59, 95% CI 1.13 to 2.23; adjusted pooled OR=1.41, 95% CI 0.96 to 2.08; figure 5). There was no heterogeneity within these pooled results for paracetamol intake during infancy.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between paracetamol intake during infancy (any vs none) and asthma in childhood before and after adjustments for respiratory tract infections. Effects estimated using fixed effects model. *Variables adjusted for before adjustment of respiratory tract infection (RTI): Schnabel et al30—gender, age at follow-up, parental history of asthma, study region; Bakkeheim et al14—gender; Wickens et al15—unadjusted. Variables adjusted for with RTI: Wickens et al15—gender, parental history of asthma, siblings, antibiotic use, maternal smoking, household smoking, location, New Zealand deprivation index, birth weight, maternal age. p Value: test for homogeneity.
Discussion
Overall, the evidence from this systematic review suggests an association between paracetamol exposure during infancy and increased risk of asthma in childhood.
However, we also found some evidence that the association between paracetamol and asthma attenuated after adjusting for respiratory tract infections during infancy, supporting the concept that these associations are, at least in part, due to confounding by indication. This was particularly evident from the analysis of increasing frequency of paracetamol exposure in infancy, where all of the studies adjusted for respiratory tract infections separately.30 ,45 ,46 While there was an association between increasing frequency of paracetamol exposure and asthma before adjusting for respiratory tract infections (OR=1.15, 95% CI 1.00 to 1.31), this association essentially disappeared when adjusted for respiratory tract infections (adjusted OR=1.06, 95% CI 0.92 to 1.22), making it unlikely that that paracetamol is a clinically important risk factor for asthma. In contrast, it was unclear whether respiratory tract infections of the mother during pregnancy changed the estimates, as only one study adjusted for maternal respiratory tract infections,44 but did so whilst simultaneously adjusting for a number of other potential confounders.
Strengths and weaknesses
This review summarises the current evidence on the association between paracetamol exposure and asthma from observational cohort studies. Among the observational study designs, cohort studies provide the strongest evidence of an association between exposure and outcome as cohort studies minimise the possibility that recall bias or reverse causation could have influenced the findings. However, as with all results based on observational studies, we cannot exclude the possibility of confounding having biased the results.48 One of the main concerns raised is that the association between paracetamol and asthma may be due to confounding by respiratory tract infections. Unlike some of the previous systematic reviews49–51 on this topic, we have explicitly addressed this issue and have found evidence to support the presence of moderate confounding by respiratory tract infections. Unfortunately, we could not fully assess the confounding effect of respiratory tract infections on the association between paracetamol exposure and asthma outcomes, as some studies did not adjust for these infections, while others did not report the individual effect of adjusting for respiratory infections.
We have attempted to standardise both the asthma outcome and exposure classification in this review as much as is feasible. Specifically we have only assessed asthma outcome after the age of 5 years, as diagnosis of asthma prior to this age is very difficult. In contrast, all previous reviews49–51 have tended to combine early life wheeze and asthma as outcomes. We have also pooled results according to specific paracetamol exposure windows (trimester and infancy), whereas previous reviews have combined different exposure classifications. Given the varying results seen for exposure during pregnancy it appears to be quite important to do so.
There were only a limited number of studies for each exposure period, which created a number of limitations. First, the small number of studies and included participants reduced the statistical power of the review and has led to imprecision in some of the pooled estimates of associations. Second, quantitative assessment of publication bias could not be undertaken because of the small number of studies within each exposure classification. As with all systematic reviews there is a possibility of publication bias, and this could have resulted in an overestimate of the association between paracetamol exposure and asthma. However gross publication bias does not seem likely because studies reporting both positive and negative relationships have been published.
While the results for the associations between exposure during infancy and childhood asthma were quite consistent, there was marked heterogeneity among the studies looking at the associations with exposure during pregnancy. We considered using meta-regression techniques to identify the discrepant findings, but there was an insufficient number of studies to do so.
While the study by Kang et al42 showed discrepant results from the other studies, it seems to be of high quality. Some of the heterogeneity between Kang et al and the remaining studies may be due to differences in the ascertainment of the exposure to paracetamol, and the wide variation in the proportion of expectant mothers taking paracetamol during pregnancy. The lowest prevalence of exposure to paracetamol during pregnancy was reported in Bakkeheim et al (6%),14 where exposure was retrospectively recalled on the maternity ward. In contrast, Kang et al42 observed that 69% of mothers took paracetamol during pregnancy; use of paracetamol was ascertained both at 24 weeks gestation and within 1 month of birth, using detailed questioning. In addition, Kang et al included a high proportion of pregnant women with asthma (47%), in part because they recruited all mothers with asthma and only a random sample (62%) of mothers without asthma. These differences may have influenced this study's findings
Confounding by respiratory tract infections
All studies that adjusted for early life respiratory tract infections found a reduction in the association between paracetamol exposure and subsequent childhood asthma. It remains unclear if maternal infection during pregnancy could confound the association between maternal paracetamol exposure and asthma outcome. Only one study has adjusted for maternal infections,44 and when these authors did so, they also adjusted for a range of other factors at the same time.
To untangle effects of respiratory tract infections, the strongest evidence comes from those few observational studies that have examined the effect of paracetamol given for non-respiratory indications. To date, only two studies30 ,46 have done this and significantly, both have failed to identify an increased risk of asthma associated with paracetamol given to infants for non-respiratory reasons. Future studies are required to confirm that the association between paracetamol and asthma is confounded by respiratory tract infections, and they should include assessment of the indication for paracetamol use.46
Existing RCT evidence
Conducting RCTs offers the potential to produce the most definitive evidence to confirm or refute whether paracetamol may harm children's respiratory health.
We identified three RCTs in the literature, but none of these studies evaluated the effect of paracetamol and the incidence of asthma; instead the study population was children with existing asthma. Lesko and Mitchell38 randomised participants to receive either paracetamol or ibuprofen and monitored for adverse effects; they found, in a subgroup analysis, higher asthma-related hospitalisations among users of paracetamol than ibuprofen. However, it is not clear whether this is due to a protective effect of ibuprofen against severe exacerbations of asthma or an increased risk due to paracetamol. This study was not designed specifically to assess the effect of these medicines on asthma, and combined asthma and bronchiolitis as outcome measures. Kodgule et al39 examined airway resistance between children randomised to receive paracetamol or placebo and found that paracetamol increased airway resistance. Soferman et al40 assessed the effect of a single therapeutic dose of paracetamol in 42 asthmatic children and matched healthy controls, and found that paracetamol did not and they should include assessment of the indication for paracetamol use.
Conducting an RCT to determine if paracetamol intake influences incidence of asthma would be difficult to undertake. A placebo control arm in such trials is likely to be met with ethical restrictions and participants in the placebo arm are unlikely to be compliant. A possible solution would be to use an ibuprofen control arm, but any effects seen might be due to a reduction in the risk caused by ibuprofen rather than an increase in risk caused by paracetamol. It would appear that the results of such a trial are years, if not decades, away from being available, and may never be conducted. This makes balanced interpretation of the results from high quality cohort studies essential.
Comparison with previous systematic reviews
Unlike previous reviews,49–51 we found weak evidence to support an association between paracetamol use in childhood and incident asthma. This difference in findings is due, in part, to the studies included in this review in comparison to past reviews. The review by Etminan et al51 combined the findings of the cohort studies with cross sectional studies, with the latter dominating the overall findings, whereas in this review we only included cohort studies. In addition, our review also included three studies13 ,41 ,45 that had not been published at the time of previous reviews by Etminan et al51 and Eyers et al,50 or were missed30 due to a lack of a systematic review by Garcia-Marcos et al.49 Furthermore, we focused on asthma measured after the age of 5 years rather than wheeze symptoms. Finally, we examined the effect of adjusting for respiratory tract infections and found that doing so reduced the strength of association between frequency of paracetamol exposure in infancy and childhood asthma.
Conclusion
The evidence of an association between early life paracetamol and asthma is often overstated, and there is currently insufficient evidence to support changing guidelines in the use of this medicine. Further well designed clinical trials and/or cohort studies are required to definitely answer this question. Respiratory tract infections appear to confound this association and it is essential that this be accounted for in future observational studies. Future studies should also assess the effect of paracetamol exposure on lung function outcomes given that paracetamol is proposed to induce oxidative stress on the airway.
Acknowledgments
We thank Dian Xu for assisting with reviewing titles and abstracts of potential articles for inclusion and for checking data extraction.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors All authors contributed to the conception of the work. MC developed the search strategy and selected eligible papers. MC and AJL wrote the first draft and all authors contributed to subsequent interpretation and drafting the manuscript. All authors have given final approval of the version to be published and agree to be accountable for all aspects of the work.
Funding AJL, SCD and MM are supported by the National Health and Medical Research Council (NHMRC). MC received a scholarship from Australian Awards to study a Master of Science (Epidemiology) at the University of Melbourne.
Competing interests None.
Provenance and peer review Commissioned; externally peer reviewed.