Article Text

Abstract
Introduction There is a hypothesis that chronic obstructive pulmonary disease (COPD) is an accelerated ageing disease. Frailty is a geriatric syndrome characterised by physical, psychological and social vulnerability, thought to be a feature of ageing. The authors aimed to explore the relationship between frailty and physiological and patient-reported outcomes (PROs) in subjects with stable COPD.
Methods We administered the Kihon Checklist that has been validated for frailty screening. We also assessed patient-reported measurements of health status and dyspnoea using the COPD Assessment Test (CAT), the St. George’s Respiratory Questionnaire (SGRQ), the Hyland Scale, the Medical Outcomes Study 36-item short-form (SF-36), the Baseline Dyspnea Index (BDI) and the Dyspnea-12 (D-12). Pulmonary function was also measured.
Results Of 79 consecutive COPD outpatients, 38 (48.1%), 24 (30.4%) and 17 (21.5%) patients were classified as robust, prefrail and frail, respectively. The total Kihon Checklist score was significantly weakly to moderately correlated with the CAT score (Spearman’s rank correlation coefficient (Rs)=0.38, p<0.01), the SGRQ total score (Rs=0.65, p<0.01), the Hyland Scale score (Rs=−0.54, p<0.01), all subscale scores of the SF-36 (Rs=−0.64 to −0.31, p<0.01), the BDI score (Rs=−0.46, p<0.01) and the D-12 score (Rs=0.41, p<0.01). We found no or only weak correlations between the total Kihon Checklist score and lung function measurements. We found statistically significant between-group (robust, prefrail and frail) differences in most PRO scores. Using stepwise multiple regression analyses to identify the variables that predicted the total Kihon Checklist score, the SGRQ total score alone significantly explained 49.1% of the variance (p<0.01).
Discussion Frailty was significantly correlated with PROs, especially health status, unlike lung function. Frailty should be assessed in addition to PROs separately from lung function as part of multidimensional analyses of COPD.
- Chronic obstructive pulmonary disease (COPD)
- frailty
- patient-reported outcomes (PROs)
- St. George's Respiratory Questionnaire (SGRQ)
- health status
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Chronic obstructive pulmonary disease (COPD)
- frailty
- patient-reported outcomes (PROs)
- St. George's Respiratory Questionnaire (SGRQ)
- health status
Introduction
Chronic obstructive pulmonary disease (COPD) is a common respiratory condition with persistent airflow limitation defined by spirometry, often coexisting with comorbidities that have significant impacts on morbidity and mortality.1 Since it is well known that ageing of the lungs and COPD have many similarities and are sometimes difficult to distinguish from each other, COPD is occasionally considered to be an accelerated ageing disease.2 Furthermore, ageing of the population is thought to be closely related to morbidity of COPD since age is known to be a risk factor for COPD and also a predictor of mortality and hospital admission for exacerbations.3
Frailty is a geriatric syndrome recognised as a clinical state of physical, psychological and social vulnerability that embodies an increased risk of requirement of care.4 5 Fried et al defined frailty as meeting three out of five criteria comprising unintentional weight loss, self-reported exhaustion, low grip strength, slow walking speed and low physical activity.6 Frailty is thought to be one of the defining features of ageing and several concise measurement tools have appeared in the literature as a consequence.5 The Cardiovascular Health Study Index developed by Fried et al has been the most widely used to assess this biological syndrome.6 Alternative tools such as the Frailty Index and Clinical Frailty Scale using the cumulative deficit approach have also been validated.7–9 The Kihon Checklist questionnaire developed by the Japanese Ministry of Health, Labour and Welfare has also been demonstrated to be useful as a screening tool for identifying frail individuals and is widely administrated in clinical practice in Japan (online supplementary table 1).10–12
However, the relationship between frailty and outcomes and markers in patients with COPD has not been clearly established.13 Under the assumption that frailty can be measured by the Kihon Checklist, the primary purpose of the present study is to investigate the relationships between frailty status assessed by the Kihon Checklist and clinical indices regarding physiological outcomes and patient-reported outcomes (PROs) such as health status and disease-specific symptoms, such as dyspnoea, in subjects with stable COPD. The authors intended to determine whether frailty measurement should be included in a multidimensional assessment of COPD in clinical practice.
Methods
Study subjects
We recruited 79 consecutive patients with clinically stable COPD, as defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD)1 between January 2015 and July 2016. Criteria for inclusion in this present study were as follows: (1) age over 50 years, (2) smoking history of more than 10 pack-years, (3) postbronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio of less than 0.7, (4) no obvious abnormal shadows on chest X-rays which could influence lung function, (5) absence of any other active lung disease, (6) absence of uncontrolled comorbidity and (7) no changes in treatment regimen during the preceding 4 weeks. Exclusion criteria were (1) history of asthma and (2) exacerbation of COPD within the preceding 3 months. All patients had more than 6 months of outpatient management before entry into the study to avoid subsequent changes brought about by new medical interventions. The study protocol was approved by the Institutional Ethics Committee of the National Center for Geriatrics and Gerontology (No. 805–2). Written informed consent was obtained from all patients before the study. All eligible patients finished the following examinations on the same day: pulmonary function tests and assessment of frailty and PROs.
Pulmonary function testing
All subjects were asked to come to the site at least 12 hours after cessation of bronchodilator use. Generally, subjects underwent spirometry using a spirometer (CHESTAC-8800; Chest, Tokyo, Japan) more than 60 min after inhaling a dry-powder formula of long-acting bronchodilators under the supervision of an attending physician. Spirometry was performed three times, and largest values were then analysed. The residual volume was measured by the closed-circuit helium method, and the diffusing capacity for carbon monoxide (DLCO) was measured by the single-breath technique.
Frailty assessment using the Kihon Checklist
The Kihon Checklist is a self-administrated questionnaire consisting of 25 items which are yes/no questions covering instrumental (three items) and social activities of daily living (four items), physical strength (five items), nutritional status (two items), oral function (three items), cognitive status (three items) and depression risk (five items).10 However, although one of the questions (question no. 12 in the online supplementary file 1) asks about body mass index (BMI) and is usually scored by participants themselves, this score was calculated using the values obtained from pulmonary function tests and therefore was not self-reported in the present study. The total score of the Kihon Checklist, which is a sum of 25 answers, ranges from 0 (no frailty) to 25 (severe frailty) and we classified patients’ frailty status as robust (0–3), prefrail (4–7) and frail (8–25), as previously reported.12
Patient-reported measurements
Disease-specific health status was assessed with previously validated Japanese versions of the COPD Assessment Test (CAT) and St. George’s Respiratory Questionnaire (SGRQ) (V.2).14–17 The CAT is a questionnaire consisting of eight items scored from 0 to 5 in relation to cough, sputum, dyspnoea, chest tightness, capacity for exercise and activities,sleep quality and energy levels. The CAT scores range from 0 to 40, with a score of 0 indicating no impairment.15 17 The SGRQ consists of 50 items divided into the three components of symptoms, activity and impacts, and the total score is calculated with scores ranging from 0 to 100. Higher scores on the SGRQ indicate a more severely impaired health status.14 16
Generic health status was assessed by the Japanese version of the Medical Outcomes Study 36-item short-form (SF-36), which has been previously validated.18–20 The SF-36 is a measure composed of eight subscales (physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health). We used the SF-36 V.2 with norm-based scoring in which each domain score has a mean of 50 and an SD of 10 in the Japanese general population. Higher scores indicate better health situations. The global health was also assessed by the Japanese version of the Hyland Scale with scores ranging from 0 to 100, where 0=‘might as well be dead’ and 100=‘perfect quality of life’.21 22
To assess the severity of dyspnoea, we used the Japanese versions of the Baseline Dyspnea Index (BDI) and the Dyspnea-12 (D-12).14 23 24 A newer Japanese version of the BDI developed in 2008 was used in this study. The BDI is composed of three categories: functional impairment, magnitude of task and magnitude of effort, rated by five grades from 0 (severe) to 4 (not impaired) for each. The Japanese version of the D-12 consists of 12 items, each with a 4-point grading scale (0–3). The D-12 scores range from 0 to 36, with higher scores denoting more severe dyspnoea. The CAT, SGRQ, SF-36, Hyland Scale, BDI and D-12 were self-administered under site supervision in the aforementioned order (in a booklet form). One of the authors (KN) reviewed the surveys to ensure that subjects did not unintentionally omit any questions.
Statistical analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows V.19. All results are expressed as means ± SD. Relationships between two sets of data were analysed by Spearman’s rank correlation tests. The significance of between-group difference was determined by an analysis of variance, and when a significant difference was observed, Bonferroni tests were used to analyse where the differences were significant. To identify variables that predicted the total Kihon Checklist scores, a stepwise regression analysis was conducted.14 A p value of <0.05 was considered to be statistically significant.
Results
Characteristics of the study subjects and the classification of frailty status
Baseline characteristics of the 79 subjects are presented in table 1. The mean age of the subjects was 74.8 years. The mean FEV1/FVC ratio was 55.4%, ranging from 21.9% to 61.0%. Fifty-two patients were treated with both tiotropium bromide and salmeterol and fluticasone propionate in combination (SFC), 19 with tiotropium bromide alone, 4 with SFC and 4 with no long-acting bronchodilators. Using the classification of severity of airflow limitation in COPD of the GOLD criteria,1 out of 79 patients studied, 24 subjects (30.4%) were in GOLD 1, 40 (50.6%) in GOLD 2, 12 (15.2%) in GOLD 3 and 3 (3.8%) in GOLD 4.
Characteristics of 79 consecutive patients with COPD and Spearman’s rank correlation coefficients between the total Kihon Checklist scores and those of clinical indices
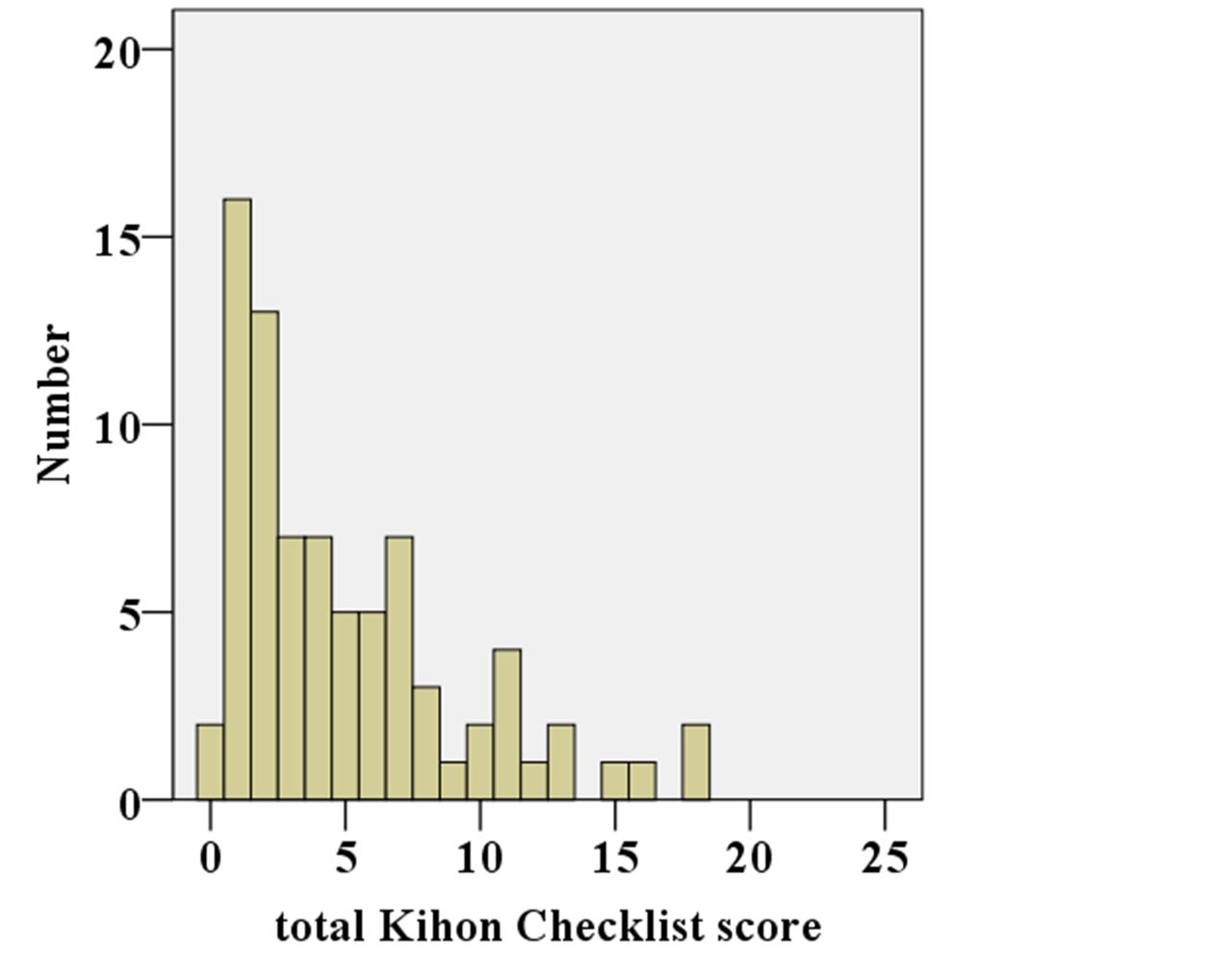
shows the frequency distribution histograms of the total Kihon Checklist score. The bar charts of frequency showed a non-normal score distribution and skewed towards a lower score. On the basis of the total Kihon Checklist score, we classified 38 (48.1%), 24 (30.4%) and 17 (21.5%) subjects as robust, prefrail and frail, respectively.

{kind=link}
Frequency distribution histograms of the total Kihon Checklist score.
Relationship of various outcomes with the Kihon Checklist total score
Table 1 shows the correlation between the total Kihon Checklist score and various clinical indices. As for the physiological indices, VC (L, percentage predicted (% pred)), FVC (L), FEV1 (L) and DLCO (mL/min/mmHg, % pred) had significant weak associations with the total Kihon Checklist score (absolute Rs <0.4, p<0.05). Other lung function parameters had no statistically significant correlations with the total Kihon Checklist score.
The total Kihon Checklist score was weakly to moderately correlated with health status using the CAT score (Rs=0.38, p<0.01), the SGRQ total score (Rs=0.65, p<0.01), all SF-36 subscale scores (Rs=−0.64 to −0.31, p<0.01), and the Hyland Scale score (Rs=−0.54, p<0.01), and with dyspnoea using the BDI score (Rs=−0.46, p<0.01) and the D-12 score (Rs=0.41, p<0.01).
Comparison between robust, prefrail and frail groups
We categorised patients’ frailty status into robust, prefrail and frail using the total Kihon Checklist score. With respect to lung functions, although FEV1 (L) and DLCO (mL/min/mm Hg, % pred) showed statistically significant between-group differences (p<0.05), we found no noteworthy between-group differences in the following indices; FEV1 (% pred), FEV1/FVC (%), total lung capacity (TLC) (% pred), inspiratory capacity (IC) (L), IC/TLC (%) and DLCO/VA (mL/min/mmHg/L) (table 2).
Comparison of clinical indices between robust, prefrail and frail groups classified by the Kihon Checklist
In contrast, we found statistically significant between-group differences in the CAT score, the SGRQ total score, all SF-36 subscale scores and the Hyland Scale score (table 2). In relation to dyspnoea, both the BDI score and the D-12 score showed significant between-group differences.
Predictive factors of the total Kihon Checklist score
We subsequently performed stepwise multivariate regression analysis to identify those variables that predicted the total Kihon Checklist score. We selected several independent variables based on our presumption that they were associated with COPD severity: age (years), cumulative smoking (pack-years), BMI (kg/m2), the SGRQ total score, the BDI score, FEV1 (L), IC/TLC (%), DLCO/VA (mL/min/mmHg/L) and arterial oxygen pressure (mmHg) as explanatory variables. We took the SGRQ total score as disease-specific health status, the BDI score for dyspnoea, FEV1 for airflow limitation, IC/TLC for hyperinflation and DLCO/VA for gas exchange. When entering these variables in a regression model, we found that the SGRQ total score was the only significant predictor and it explained just 49.1% of the variance (p<0.001).
Discussion
We cross-sectionally analysed the relationship between frailty status and various clinical indices in subjects with COPD. We then found out significant associations between patient-reported measurements and the total Kihon Checklist score and their statistically significant between-group differences among robust, prefrail and frail, which contrasted with the case with lung function measurements. In multivariate analysis, the SGRQ total score was the only significant main predictor of the total Kihon Checklist score.
The prevalence of frailty was 21.5% of the subjects (mean age: 74.8 years) in the present study, which is almost compatible with other studies, although direct comparison is difficult due to the differences in both criteria used and populations or settings studied.25 Although the Kihon Checklist, on which our definition of frailty is based, is a widely used measure in Japan, cross-cultural validation will be needed in future.11
Health status assesses the physical, psychological and social impacts of the disease on daily life of the patients. This indicates that there are some conceptual commonalities between health and frailty status. The SGRQ assesses the overall summary of the effects of COPD,26 and the Kihon Checklist is one of the cumulative deficit approaches to assessing frailty by enumerating abnormalities. Therefore, it is not surprising that health status measurements were significantly related with frailty status, and that the SGRQ most significantly explained the Kihon Checklist among various clinical measurements in COPD. Similarly, recent study shows that frailty status was significantly related to health status using the Chronic Respiratory Disease Questionnaire and the CAT, although adjusted analyses were not performed.27 In addition, considering that dyspnoea is one of the most important contributors to health impairments,14 it is plausible that dyspnoea scores were significantly related to frailty in this study. Park et al reported that shortness of breath was the strongest predictor of frailty in patients with COPD.28 FEV1 has been central to the definition of COPD and possible classification of its severity. It has been shown also in the present study that FEV1 decreases from 1.91±0.53 in robust to 1.40±0.49 L in frail participants. FEV1 may be one of the predictors of frailty status unlike other physiological measurement.29
However, the coefficient of determination between the total Kihon Checklist and the SGRQ total score was 0.49, indicating that, in spite of substantial similarities, the Kihon Checklist might provide some different information from the SGRQ. Frailty measured by the Kihon Checklist conventionally reflects general issues of ageing. Although there are associated similarities between COPD and the ageing process, COPD may add more to its ageing process. We previously followed patients with COPD for 5 years, and found that physiological outcomes as well as patient-reported outcomes deteriorated over time, indicating the deteriorative characteristic of COPD.30 Actually, in the present simple analyses, some lung function measurements such as VC, FEV1 and DLCO were only weakly but significantly correlated to the Kihon Checklist, but age was not. In another study, the prevalence of frailty was increased with age and GOLD stage.27 Thus, frailty assessment should be included in the multidimensional assessment of COPD separately from lung function, and further study will be needed to investigate whether and how COPD would precipitate age-related deterioration related to frailty.
We should mention some limitations of the present study. First, although we screened frailty status using the Kihon Checklist, there might be inconsistencies in frailty classification between various screening tools. In addition, we neither evaluated the responsiveness to changes nor examined whether they can predict the future outcomes. Galizia et al reported that the clinical frailty score has been found to significantly predict mortality in subjects with COPD.31 These should be studied in the near future. Second, comorbidities and frequency of COPD exacerbations prior to the study were unfortunately not recorded in this cross-sectional study. These may be related with the prevalence of frailty, as indicated in another study.27 Finally, this study design might exhibit selection bias because we recruited only patients who could attend our outpatient clinic on a regular basis. It is likely that we did not include sufficient numbers of those patients without any subjective symptoms who were unaware of having COPD, or patients who could not regularly attend our clinic due to the heavy physical burden. A small proportion of patients with severe or very severe COPD in the present single-centre study might cause a bias.
In conclusion, we demonstrated that health status among various clinical outcomes most significantly accounted for the frailty status in patients with stable COPD, but that lung function did not. In addition, frailty in COPD seems to involve some mechanism independently of age-related deterioration, reflecting systemic feature of COPD. Frailty should be assessed in addition to PROs separately from lung function as part of multidimensional analyses of COPD.
References
Footnotes
Contributors MK contributed to statistical analysis and writing of the first draft. TO contributed to statistical analysis, the interpretation and editing of the manuscript. SN contributed to the performance of the study and acquisition of data. YH contributed to the interpretation and editing of the manuscript. KN contributed, as the principal investigator, to the study concept and design, analysis of the results and writing of the manuscript. All authors read and approved the final manuscript.
Funding This study was partly supported by the Research Funding for Longevity Sciences (27-10) from the National Center for Geriatrics and Gerontology (NCGG), Japan.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The Institutional Ethics Committee of the National Center for Geriatrics and Gerontology (No. 805-2).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.