





Abstract
Maternal smoking in pregnancy (MSP) is a large modifiable risk factor for pregnancy related mortality and morbidity and also the most important known modifiable risk factor for asthma.
This review summarises the effects of MSP throughout infancy, childhood and adolescence with regards to asthma (development and severity). Firstly, the direct damage caused by nicotine on fetal lung development, fetal growth and neuronal differentiation is discussed, as well as the indirect effects of nicotine on placental functioning. Secondly, the effects of MSP on later immune functioning resulting in increased infection rate are summarised and details are given on the effects of MSP modulating airway hyperreactivity, reducing lung function and therefore increasing asthma morbidity.
Furthermore, epigenetic effects are increasingly being recognised. These can also result in transgenerational detrimental effects induced by cigarette smoke.
In summary, the causal relationship between MSP and asthma development is well documented and presents a major health problem for generations to come. The high prevalence of MSP is alarming and epigenetic effects of nicotine on immune functioning potentiate this danger. A considerable part of the increase in asthma prevalence worldwide is due to MSP.
Abstract
Smoking in pregnancy increases asthma by interference of lung and placental function and through epigenetic changes http://ow.ly/WkbB301cyaS
Introduction
Since Strachan and Cook [1] published their results on smoking and the association with asthma in children and adolescents, more than 70 longitudinal cohort studies have been performed analysing the effects of MSP and later asthma [2]. MSP has been proven to increase asthma incidence [3] in children and adolescents. Prevention of tobacco smoke exposure during pregnancy has been the one single factor that has consistently been shown to reduce asthma risk in different populations, countries and study settings. Other primary asthma prevention strategies have shown little to no success. Currently, besides prenatal and environmental tobacco exposure (ETS) prevention, only exclusive breastfeeding can be recommended for 4–6 months as a possible strategy to reduce asthma risk (later via infection reduction risk); dietary allergy prevention on the contrary has shown little or no benefit to date [4].
A long-term increase in the prevalence of asthma due to MSP has been documented multiple times and adult onset diseases such as chronic obstructive pulmonary disease may also partly have their origin in MSP [5].
In this review, the most important effects of smoking in pregnancy on asthma in children and adolescents will be summarised, emphasising the fact that cigarette smoking during pregnancy is the single largest modifiable risk for all pregnancy-related morbidity and mortality [6]. The effects of smoking on the fetus can be summarised using the term “fetal tobacco syndrome” [7]; this report however, summarises only the effects of smoking in pregnancy with regards to childhood asthma.
Epidemiology of MSP
The World Health Organization (WHO) report that almost half of all children are exposed to environmental tobacco smoke in public places [8]. The true prevalence of smoking in pregnant woman, however, is difficult to quantify [9, 10]. Under-reporting due to social unacceptability of smoking among pregnant women in pregnancy is likely [11] and discrepancies in reporting of smoking status in pregnancy have been found [12]. Older studies from Sweden report a drop in MSP rates from 29% to 21% from 1991 to 1997 [13]. Similarly, the prevalence of women who smoked at some point in pregnancy declined significantly from 22% in 1997 to 16% in 2005. However, among women younger than 20 years at delivery, pregnancy-related smoking prevalence increased from 37 to 43% [14]. The UK national registry data showed a pregnancy smoking rate of 36% in 2000 [15]. Since then, a trend to lower prevalence rates has been reported [16]. Data from the USA show prevalence of smoking at any time during pregnancy was 8.4%, with 20.6% of women who smoked in the first or second trimesters quitting by the third trimester. Smoking during pregnancy was more prevalent for women aged 20–24 years (13.0%) and the highest rate was found for non-Hispanic American Indian or Alaska Native women (18.0%) [17]. Despite the fact that smoking prevalence has decreased in smoking mothers in most western countries [18], approximately one-third of these women continue to smoke during early pregnancy [5].
To overcome possible under-reporting, anonymous online web-based questionnaires have also been performed. Here, large variations in the prevalence of smoking in woman of childbearing age and also large differences in MSP have been reported by pregnant woman in 15 European countries [19]. Certain characteristics make it more likely for a woman to smoke during pregnancy: Living without a spouse or partner and coming from a low socioeconomic background is known to be associated with continuous smoking during pregnancy [20, 21]. Smoking prevalence rates are particularly high in indigenous populations in Australia [22]. Children from unplanned urban low-income pregnancies [23] are also more often exposed during pregnancy; also, it has been found that children exposed to ETS live a “less healthy life” in terms of breast feeding and antioxidant intake.
Epidemiology of asthma in children
Asthma represents the most common chronic disease among children [24]. There are large variations in the prevalence worldwide [25] with up to 13-fold differences between countries [26]. A statement of the World Allergy Organization (WAO) recently summarised that the prevalence of allergic airway diseases, such as asthma and rhinitis, has increased dramatically to epidemic proportions worldwide and that some of the environmental changes of the last decades are considered to have had negative effects on respiratory health and have enhanced the frequency and severity of respiratory diseases, such as asthma, in the general population [27]. Climate changes and the massive increase in emissions of air pollutants due to economic and industrial growth in the last century have made air quality an environmental problem of primary importance in a large number of regions of the world [27]. Tobacco exposure is a major source of indoor air pollutants [28].
Cigarettes contain >4000 substances, 250 known to be toxic, 50 known as being carcinogenic [29] with known deleterious health consequences [30]. The mother's challenge with tobacco product consumption is that nicotine is highly addictive, and addiction to nicotine prevents many pregnant women who wish to quit smoking from doing so. An additional challenge is that clearance of nicotine and cotinine is increased in pregnant women [1]; therefore, craving occurs earlier, which results in smoking cessation being more difficult than in the un-pregnant state [31].
The baby's challenge with nicotine is that it enters the fetus via the placenta [32]; most nicotine returns to the maternal circulation for elimination but some enters the amniotic fluid via the fetal urine which results in nicotine and cotinine accumulation in the amniotic fluid [33].
Magnitude of effect of MSP on asthma increase
It is well documented that asthma incidence is increased by MSP [34, 35]. Birth cohort studies have found asthma incidence to be higher in mothers who smoked during pregnancy (adjusted HR 1.79 (95% CI 1.20–2.67) [36]. A recent meta-analysis reported MSP to significantly increase asthma risk in children of all age groups [2]. The authors found pooled odds ratios of 14 studies showed an increase in wheeze in children aged 2 years and younger (OR 1.41 (95% CI 1.19–1.67)), an increase in asthma risk in children aged 2 years and younger (OR 1.85 (95% CI 1.35–2.53)) and the risk of asthma in children aged 5–18 years was significantly increased (OR 1.23 (95% CI 1.12–1.36)) [2].
Maternal second-hand smoke exposure during pregnancy also significantly increases the asthma risk in preschool children (OR 1.42 (95% CI 1.06–1.91)) [37] and in school children (OR 1.34 (95% CI 1.01–1.76)) [38].
Pathophysiology of MSP exposure on the fetus
The effect of MSP can be divided in those effects caused directly by the toxins in utero and by indirect effects via the damage caused in the placental unit.
Smoking causes damage of the feto-placental unit; these detrimental effects are already seen early in the course of pregnancy. Thickening of the basement membrane, increase of tissue and morphological changes in the placenta are seen in the first trimester [33], and decreased vascularisation [39] results in nutrient delivery decrease [40]. The reduced nutrient supply is likely to be the reason for the increase in the occurrence of growth restriction in MSP, which was recently reported as adjusted odds ratio of 1.9 (95% CI 1.69–2.13) and smoking accounted for 13.9% (95% CI 11.2–16.5) of the cases of growth restriction occurring in the population with a dose–response relationship; older pregnant women and those with a previous history of preterm delivery have an increased susceptibility [41].
With regards to the lung development, many effects of various toxins in tobacco smoke are still unknown and the effects of the various toxins in cigarette smoke have not been analysed systematically. Most research has focused on the effects of nicotine in pregnancy on the child [42]. One important effect of nicotine is its effect on the structural development of the lung, with aberrant development of the fetal lung structure having been shown in experimental models [5]. The alveoli are bigger and a potential mechanism for reduced lung function is a reduction in the number of alveolar–bronchiolar attachment points, resulting in reduced alveolarisation [43]. In another animal study [44], pregnant mice were exposed to nicotine pre- and post-natally with post-natal lung function measurements showing that pre-natal nicotine exposure between gestation day 14 to post-natal day 7 led to a decrease in forced expiratory flow in offspring, modulated through the α7 nAChR receptor. Also, offspring of smoke-exposed guinea pigs have reduced numbers of alveolar–bronchiolar attachment points [45]. Hence, in animal models, it has repeatedly been shown that fetal exposure to nicotine reduces the surface complexity of the lung parenchyma, increase collagen accumulation, up-regulates surfactant protein gene expression and induces neuro-endocrine cell hyperplasia in fetal lungs [43]; this explains lung function changes [46].
Another effect is premature ageing of the lungs also documented in animal models. Here, a combination of reduced glycolysis and AMP increase induces cell death [47]. Furthermore, glucose is an essential source of energy in lung tissue and it has been shown that nicotine results in sustained suppression of glycogenolysis and glycolysis in lung tissue [48]. A study showed glucose levels to be significantly lower in lungs of rat offspring exposed to nicotine in utero and also during lactation [43].
Finally, it has been shown that MSP increased levels of oxidative stress markers in the mother and offspring [49]. One study in humans found vitamin C supplementation in smoking pregnant women to result in better air flow and less wheezing through the first year of life [50]. However, by introduction of antioxidants, the balance of normal developmental signals can be disrupted which again may interfere with neuro-differentiation [51]; therefore, caution is needed before general recommendations can be given. Further research is needed to fully understand the complex mechanism of lung damage due to MSP [52]. The reported effects of nicotine, however, are a clear indication that nicotine and, therefore, also the use of nicotine replacement therapy by pregnant or breastfeeding females is not without risk and cannot be recommended as an appropriate and safe smoking cessation strategy for pregnant woman. Interestingly, children exposed to MSP are more likely to experiment with tobacco themselves. Children exposed to more than half a pack per day during gestation have been found to have a 5.5-fold increased risk for early experimentation [53]. Without doubt, peer group and social environment also play a major role [53]. Whether this increase is due only to imitation of adult behaviour, peer group smoking or is part of neuronal changes occurring in the developing brain [54], needs to be clarified; however, this is not the main focus of this review.
Early life influences: preterm birth, reduced lung function and risk of infection
Preterm birth
Smoking in pregnancy increases the risk of preterm birth [55] by 1.2–1.6 compared with non-smokers [56] and there is a stronger association with “very preterm” infants (<32 weeks gestational age). A dose–response relationship was found between number of cigarettes smoked and pregnancy duration [57] and there is a clear association with birth complications, such as premature rupture of the membranes [58].
Lack of lung maturation and long-term lower lung function values tracking from infancy to adulthood have been documented in children born preterm [59, 60]. Preterm infants show decreased lung function at 1 year of age [61] and often increased airway hyper-responsiveness [62]. Other authors have reported no evidence that antenatal smoking exposure increases airway hyper-responsiveness, rather that it may be associated with a diminished response to both bronchoconstrictors and bronchodilators in infants [63]. Furthermore, prematurity is often accompanied with therapies such as mechanical ventilation and antenatal corticosteroids. Both prematurity and antenatal steroids have shown to be associated with an increased incidence of childhood asthma [64]. Prematurity is associated with an increased asthma risk, an older meta-analysis found odd ratios of 1.36 (95% CI 1.30–1.43) [65]. A more recently published article found a higher degree of prematurity to be directly associated with asthma disease severity with very preterm infants having increased adjusted odds ratio of 3.1–6.2 [66]. Exposure to corticosteroids during pregnancy, such as steroids given as part of antenatal care in case of imminent premature birth (for earlier lung maturation), was associated with a risk of asthma in childhood between 3–5 years of age with an adjusted hazard ratio of 1.19 (95% CI 1.03, 1.39), with no association noted after 5 years of age [67].
Intrauterine growth retardation
MSP is associated with an increases risk of intrauterine growth retardation (IUGR) [68], and this growth retardation is also a risk factor for poor lung function [69]. Concurrent prematurity and IUGR is a risk factor for impaired lung function at follow-up [70]. A recent study investigated the role of IUGR as predictor of lung function at school age and found that the forced expiratory volume in 1 s (FEV1) was 5.7% (95% CI −10.2 to −1.3) lower in preterm children with IUGR than in the preterm-born children with appropriate in utero growth.
Lung function in term infants
Detrimental effects of MSP on childhood lung function have consistently been reported for the last 20 years [71]. Lung function at birth is already reduced with MSP [46]. Furthermore, in term children, lower lung function in infancy is a recognised risk factor for airflow obstruction in young adults [72]. The lung function reductions caused by MSP in school-age children are reported in the single digit range; one study for example reported on average, spirometric data of FEV1/forced vital capacity (FVC), forced expiratory flow at 25–75% of FVC and peak expiratory flow rate (PEFR) to be 1.1%, 4.7%, and 3.2% lower respectively in children who had been exposed to MSP. Reduced PEFR (−3.0%, (95% CI −4.4–−1.4), mean mid expiratory flow (−4.6% (95% CI −7.0–−2.3), and forced expiratory flow at 75% of FVC (−6.2%, (95% CI −9.1–−3.1) have also been found [73]. Furthermore, MSP has long-term effects on lung function deficits; it has been found that children suffering from asthma later in life seem to be especially vulnerable to lung function deficits in the presence of MSP and ETS [74]. Children with MSP and early onset asthma have FEV1 decreases of −13.6% (95% CI −18.9–−8.2) [75].
Risk of infection
Smoking in pregnancy is further associated with increased morbidity with viral respiratory illnesses [76]. ETS increases the risk of respiratory infections, the combination of preterm birth and MSP is responsible for the two- to fourfold increased risk of wheezing illnesses observed during the first year of life in infants whose parents smoke [77].
A recently published study of 11 141children, found the reason why wheezing in childhood is socially patterned: in this representative UK cohort, adjustment for maternal smoking during pregnancy and breastfeeding removed the socioeconomic inequalities in common wheezing phenotypes and the authors conclude that policies to reduce the social gradient in these risk factors may reduce inequalities in wheezing and asthma [78]. MSP and prematurity have a joint effect on the numbers of episodes of early childhood wheezing. One study found maternal smoke exposure and prematurity to cause an increased risk of recurrent wheezing with odds ratio 3.8 (95% CI 1.8–8.0) with a significant interaction between prematurity and maternal smoking upon episodes of wheezing [55]. Moreover, the individual's risk of early childhood wheeze in connection with exposure to early maternal smoking seems to be modified by tumour necrosis factor and glutathione S-transferase P1 polymorphisms [79] with odds ratios for developing early wheeze related to early maternal smoking ranging from non-significant in some rare polymorphisms 2.4 (95% CI 1.6–3.7).
Another influencing factor for early childhood infections and later asthma risk is breastfeeding. The protective effect of breastfeeding on infant wheezing and other adverse respiratory outcomes is known [80]. However, children of mothers smoking in pregnancy are less likely to breastfeed, which again increases the risk for wheezing episodes in early life [81]. A potential role of infection in the development of the asthma syndrome later in life has also been suggested, but the underlying mechanisms are complex, poorly understood and most likely a combination of host factors and increased susceptibility under certain detrimental conditions such as MSP cause the increase of asthma in the presence of early childhood infections [82].
In one study, calculation of relative risks, the presence of the three risk factors, recurrent LRTI, MSP and breastfeeding for less than 3 months, showed a strong association with asthma with a risk ratio of 5.79 for any asthma at ages 1, 2, 4 and 10 years, hence preventing smoking during pregnancy would have a great impact on reducing asthma prevalence in children [81].
Later influences: immune system modulation, steroid efficacy and epigenetics
Smoking produces oxidative stress very early in life [49]. MSP causes changes in placental cytokine production [83] and studies suggest an increase in atopic diseases as well as asthma [84] in later life. An Australian birth cohort study showed effects of MSP even though to adolescence [85] with some altered immune measures at age 14 years. MSP was strongly related to reduced lung function and an increased risk for current asthma, current wheeze and exercise-induced wheeze; however, in this study not for bronchial hyperreactivity or atopy. Besides increasing the risk of asthma, diagnosis also the rate of emergency room visits during the previous year due to wheeze were more common in children exposed to MSP (OR 3.4; 95% CI, 1.4–7.8).
Critical knowledge gaps still exist including gene–environment interactions and how an imbalance in immune system can affect asthma incidence or exacerbation later in life [34]. Changes in the in utero and external environment with parental smoking or nicotine exposure, may reduce the capacity of the offspring to protect themselves against environmental stressors [86].
Maternal smoking, but also ETS, diesel exhaust and traffic-related particles, heavy metals, antibiotics, environmental oestrogens and other endocrine disruptors all influence immune system maturation [87]. These toxins are thought to have the ability to activate or silence certain immune regulating genes and then have a major impact on the current individual immune response. These toxins are some of various factors that have been made responsible for the rise in childhood allergy and adverse outcomes following developmental immunotoxicity (DIT; problematic exposure of the developing immune system to xenobiotics and physical environmental factors) [88]. Changes in the immune response, with an overall T helper type 1 (Th1)/type 2 (Th2) imbalance and an increase towards a Th2 response has been demonstrated in the presence of environmental chemicals and pollutants [88]. MSP alters [89] immune function of cord blood cells, indicating that maternal exposure to air pollution before and during pregnancy may increase the child's risk of developing health conditions later in life, including asthma.
Another phenomenon involved in MSP and later childhood asthma are the epigenetic effects; these effects can directly influence gene expression through environmental challenges and influences. Recently, MSP has been suggested as a factor that can activate or silence certain immune genes via epigenetic pathways; Epigenome-wide association studies have identified a number of differentially methylated placental genes that are associated with MSP, the differential methylation patterns of several genes have been confirmed to also exhibit altered gene expression patterns [90]; a link between differentially methylated gene loci, MSP and adverse infant health outcomes have therefore been found [38].
Recently, the Pregnancy and Childhood Epigenetics (PACE) consortium performed a meta-analysed across 13 cohorts and identified numerous loci involved in response to maternal smoking in pregnancy with persistence into later childhood [91]. Future research is needed to investigate the mechanistic roles that these differentially methylated genes may play in mediating the association between MSP and disease [90]. Also in a rat model, epigenetic mechanisms have been found, where detrimental effects of nicotine have been documented to reach to third-generation offspring, demonstrating the transgenerational transmission of the asthma phenotype following perinatal nicotine exposure [92]. In humans, effects of MSP on later generations has been documented, with grand-maternal smoking increasing the risk the asthma in their grandchildren in two studies [93, 94], whereas it had no impact in one other report [95].
There is evidence that perinatal differences in immune function of allergy-prone newborns extend beyond previously recognised differences in effector T cell (Th1/Th2) function, to also include differences in neonatal regulatory T cell and Th17 function and, moreover, that these pathways are also epigenetically regulated [96].
Studies have also shown that the capability of toxins such as ETS to induce asthma and asthma symptoms may be modified by genetics. Some of the genes modifying the effect of ETS and air pollution in the individual may have been identified. When these detoxification enzymes are genetically defective or missing, then the capability of the lung to metabolise hazardous substances is dramatically diminished [97]. With regards to these observations, it has been found that children with certain genotypes, such as the glutathione S-transferase mu 1 null genotype are genetically more susceptible to the effects of in utero tobacco exposure [98]. Also, the risk for asthma and wheeze was found to be greater for children with the Arg16Arg genotype or 2 copies of the Arg16-Gln27 diplotype [99].
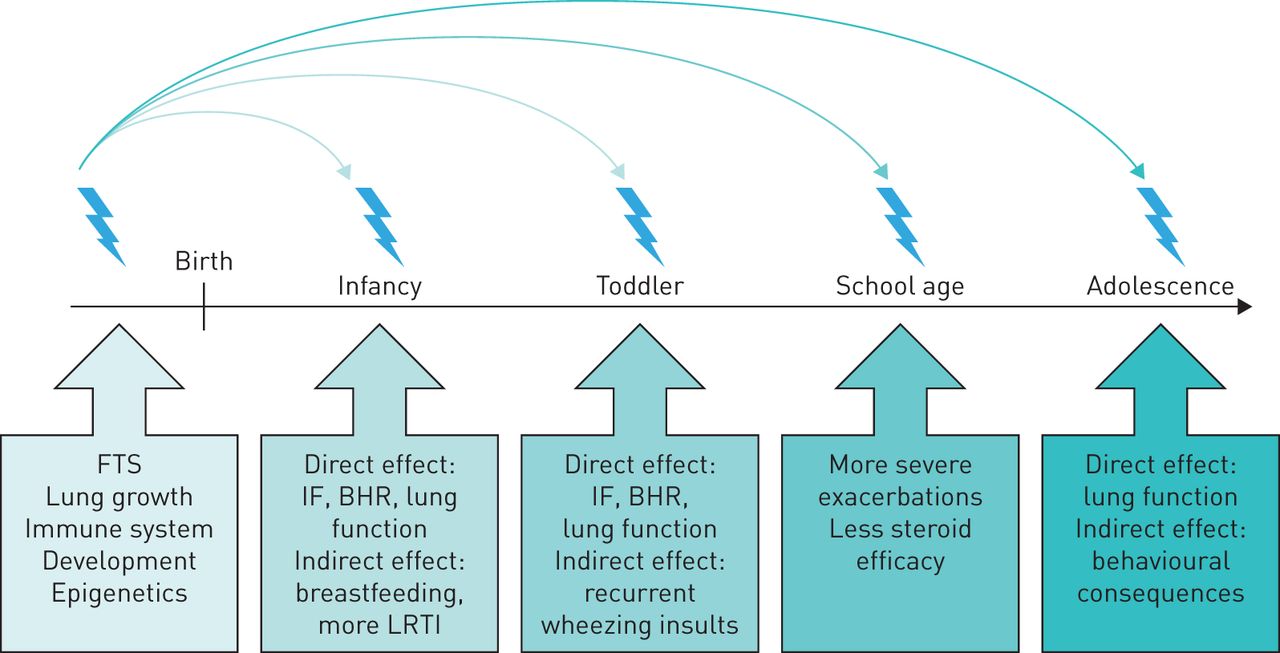
Recently, reports have found lower efficacy of inhaled corticosteroids in asthmatic children exposed to MSP [100] irrespective of current ETS. MSP appears to even increase the risk of wheeze and asthma among children who are not exposed to maternal smoking after birth [101]. Asthma was most strongly associated with MSP, but postnatal exposure showed independent associations with a range of other respiratory symptoms [102]. The most important long term influences of MSP on infants, toddlers, school-age children and adolescents reported in this review are summarised in figure 1.

{kind=link}
Summary of effects of maternal smoking in pregnancy (MSP) from infancy to adolescence. FTS: fetal tobacco syndrome; IF: immune function; BHR: bronchial hyperreactivity; LRTI: lower respiratory tract infection.
Summary: asthma prevention via MSP reduction
MSP can have persistent effects on lung development, lung function and respiratory health later in life. Greater awareness regarding the major impact of this risk factor is still needed [77, 103]. Smoke-free policies result in a reduction of smoking in public, reduction of ETS exposure of pregnant woman and most likely also in a direct reduction of MSP and these policies have shown great success: they are associated with substantial reductions in preterm birth and reductions in hospital attendance for asthma [104]. Asthma prevention [74] via avoidance of tobacco smoke must be recommended to caregivers of all infants and children and, in particular, those with a high risk of asthma [105]. Avoiding MSP will reduce the risk of development of asthma [36].
Footnotes
Conflict of interest: None declared.
- Received March 26, 2016.
- Accepted June 5, 2016.
- Copyright ©ERS 2016
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References











Jump To
- Article
- Abstract
- Abstract
- Introduction
- Epidemiology of MSP
- Epidemiology of asthma in children
- Magnitude of effect of MSP on asthma increase
- Pathophysiology of MSP exposure on the fetus
- Early life influences: preterm birth, reduced lung function and risk of infection
- Later influences: immune system modulation, steroid efficacy and epigenetics
- Summary: asthma prevention via MSP reduction
- Footnotes
- References
- Figures & Data
- Info & Metrics