





Abstract
Smoking induced inflammation leads to distal airway destruction. However, the relationship between distal airway dysfunction and inflammation remains unclear, particularly in smokers prior to the development of airway obstruction.
Seven normal controls and 16 smokers without chronic obstructive pulmonary disease (COPD) were studied. Respiratory function was assessed using the forced oscillation technique (FOT). Abnormal FOT was defined as elevated resistance at 5 Hz (R5). Parameters reflecting distal lung function included frequency dependence of resistance (R5–20) and dynamic elastance (X5). Inflammation was quantified in concentrated bronchoalveolar lavage utilising cell count differential and cytokines expressed as concentration per mL epithelial lining fluid.
All control subjects and seven smokers had normal R5. Nine smokers had elevated R5 with abnormal R5–20 and X5, indicating distal lung dysfunction. The presence of abnormal FOT was associated with two-fold higher lymphocyte and neutrophil counts (p<0.025) and with higher interleukin (IL)-8, eotaxin and fractalkine levels (p<0.01). Reactivity of R5–20 and X5 correlated with levels of IL-8, eotaxin, fractalkine, IL-12p70 and transforming growth factor-α (r>0.47, p<0.01).
Distal airway dysfunction in smokers without COPD identifies the presence of distal lung inflammation that parallel reported observations in established COPD. These findings were not evident on routine pulmonary function testing and may allow the identification of smokers at risk of progression to COPD.
Abstract
Isolated dysfunction in distal airways identifies pulmonary inflammation in asymptomatic smokers with normal airflow http://ow.ly/8bVk305aVkj
Introduction
The diagnosis of chronic obstructive pulmonary disease (COPD) is dependent on the identification of reduced airflow using spirometry (Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria). However, spirometry may be normal early in the disease process. Furthermore, the GOLD guidelines have removed the “at risk” stage 0, since many smokers do not progress to COPD as defined by clinical and spirometric data. This may, in part, reflect the inability of spirometry to detect dysfunction in the distal lung where lung units are lost early in disease [1]. It is recognised that these airways represent a “quiet zone” where considerable disease might be present before airflow limitation is identifiable using standard pulmonary function assessment [2].
Multiple tests have been used to identify small airway abnormalities in smokers; however, the relationship with COPD pathogenesis remains unclear. This study is based on the hypothesis that if small airway dysfunction is an early manifestation of a disease process that may evolve to COPD, it should be associated with inflammation at the site of injury (e.g. the distal lung). To test this hypothesis small airway function and distal lung inflammation were evaluated in smokers who did not meet criteria for COPD. Investigation of immunological derangements associated with distal airway dysfunction in the setting of normal spirometry may provide insight into pathophysiological mechanisms present at disease onset.
Methods
This investigation utilised forced oscillation testing (FOT) and its response to bronchodilator in smokers who did not meet GOLD criteria for COPD, but had focal emphysematous changes found incidentally upon chest computed tomography (CT) screening. These subjects were selected because the anatomical abnormality found suggested potential onset of disease at an early stage when COPD was not present. In vivo measurements of cell and cytokine levels in epithelial lining fluid (ELF) were correlated with respiratory function as assessed using FOT.
Subjects
23 subjects (seven normal controls and 16 smokers) underwent pulmonary function evaluation and bronchoscopy. Normal controls were asymptomatic nonsmokers (<2 pack-years) without history of lung disease. Smokers were enrolled from our lung cancer screening cohort.
Although all smokers had radiographic evidence for emphysema, findings were generally focal and mild in severity without hyperinflation. Post-bronchodilator spirometry revealed forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ≥70% in all but three subjects where values were 67–68%. In addition, based on absence of symptoms, none of these subjects met GOLD criteria for COPD. The smokers were divided into smoker normal FOT and smoker abnormal FOT groups, based on presence of abnormal oscillometry without knowledge of measured inflammatory cytokines. Exclusion criteria were interstitial lung disease, lung nodules, use of inhaled or oral steroids, regular use of anti-inflammatory drugs, malignancy, significant hepatic, renal or cardiovascular disease, diabetes mellitus and alcohol use. Medical history and details of medication use and respiratory symptoms were obtained. Participants provided signed informed consent and the study was approved by the institutional review board of New York University and Bellevue Hospital (New York, NY, USA).
Respiratory physiology
Spirometry, plethysmography and diffusing capacity (Vmax; SensorMedics, Yorba Linda, CA, USA) were performed according to published guidelines [3]. Data were compared with published normative values [4–6].
All subjects underwent FOT (pre- and post-bronchodilator) using the Jaeger Impulse Oscillation System (Jaeger USA; Yorba Linda, CA, USA) during tidal breathing with support of the cheeks [7]. Trials with stable tidal and end-expiratory volume were analysed. Since 150 impulses are analysed over a 30-s measurement, coherence >0.7 at 5 Hz and >0.85 at 10 Hz were required [8]. Reproducibility between trials (variability <10%) was required.
FOT parameters included resistance at oscillating frequencies of 5 Hz (R5) and 20 Hz (R20), frequency dependence of resistance between 5 and 20 Hz (R5–20), dynamic elastance as assessed by reactance at 5 Hz (X5), reactance area and resonant frequency. The smoker normal FOT and smoker abnormal FOT groups were defined based on a global FOT parameter of respiratory resistance (R5). Conservative limits of normal were selected that approximate 150% of mean values in normal subjects [9–14]. Data obtained in our laboratory in 80 asymptomatic nonsmoking subjects with normal spirometry and without lung disease fell within these limits.
In vivo distal lung inflammation
All subjects underwent nasal bronchoscopy 1 week after pulmonary function testing. The bronchoscope was passed without suctioning until wedged in the lingula and right middle lobe sequentially for bronchoalveolar lavage (BAL). 150 mL of sterile saline was injected for each lavage. Cell count and differential from the BAL fluid was obtained after centrifugation. 39 cytokines were measured in concentrated BAL using Luminex with Human Cytokine Panel I (Millipore, Billerica, MA, USA). Since analytes in ELF are diluted with sterile saline during BAL, a concentration step was performed via dialysis and lyophilisation, using albumin as an internal control. After ∼75-fold concentration, all six immunoglobulins and 28 out of 39 cytokines were within measurable levels. Cytokines levels that were below detectable limits were not included in the analyses (interferon (IFN)-α, IFN-β, interleukin (IL)-10, IL-13, IL-17, IL-2, IL-3, IL-4 and tumour necrosis factor-β). Urea levels in BAL and plasma were used to calculate the concentration of cells, immunoglobulins and cytokines in ELF [15].
Statistical analyses
Data are presented as median (interquartile range). Comparisons among groups were made using the Kruskal–Wallis test, with subsequent post hoc Mann–Whitney U-testing between pairs. Statistical correlation of FOT parameters and inflammation was assessed via Pearson correlation after log-transforming inflammatory cytokine and immunoglobulin data. p-values <0.05 were considered statistically significant. Since obesity has been shown to have an effect on FOT parameters [10], we performed multivariate linear regression analysis to adjust data for body mass index (BMI). Where appropriate, adjustment for multiple comparisons was performed using the false discovery rate procedure [16, 17]. SPSS Statistics (version 20.0; IBM, Armonk, NY, USA) was used for all analyses.
Results
Subject characteristics
Clinical characteristics of the three subject groups are shown in table 1. The normal control group was younger than either of the smoker groups (p=0.003) and, by design, had no smoking history. The smoker normal FOT group did not differ from the smoker abnormal FOT group with respect to demographics, smoking history, symptoms or inhaler use. None of the smokers had respiratory symptoms consistent with chronic bronchitis (daily cough with sputum production for 3 months in two consecutive years).
Subject demographics and characteristics
Table 2 shows results of pulmonary function evaluation in the three groups. The normal control group demonstrated normal spirometry, lung volumes, plethysmographic resistance and diffusing capacity. The smoker abnormal FOT group demonstrated lower pre-bronchodilator FEV1/FVC compared with the normal control group; this difference was not apparent post-bronchodilator. In addition, both smoker groups demonstrated higher values for total lung capacity compared with the normal control group, but the measured values remained in the normal range. Comparison between the two smoker subgroups showed trends for difference in median values for pre-bronchodilator FEV1 and specific conductance that did not reach statistical significance, since the interquartile ranges were similar. Thus, differences were not demonstrable between the smoker subgroups with respect to pre- or post-bronchodilator spirometry, lung volumes, plethysmographic resistance or diffusing capacity.
Lung function
In addition, table 2 shows results for oscillometry measurements. For the normal control group, all FOT parameters were within the normal range [9–13]. The smoker normal FOT group also demonstrated normal values for resistance and reactance parameters that did not differ from the normal control group. In contrast, while the smoker abnormal FOT group was defined by an abnormal R5, abnormalities were also noted in R5–20 and X5, indicating dysfunction in the lung periphery that was not evident on spirometry.
Figure 1 shows pre- and post-bronchodilator measurements of FEV1, R5, R5–20 and X5 for all subjects within each group. The FEV1 response to bronchodilator was variable within subjects in all three groups. The normal control and smoker normal FOT groups did not demonstrate a change in FEV1 post-bronchodilator. A statistically significant increase in FEV1 was noted in the smoker abnormal FOT group, but an increase >12% was evident in only a single individual. The normal control and smoker normal FOT groups did not demonstrate bronchodilator response of any of the FOT parameters. However, the smoker abnormal FOT group demonstrated significant bronchodilator response for all FOT parameters (R5 p=0.011; X5 p=0.008; R5–20 p=0.02). FOT parameters remained abnormal in approximately half of this subgroup.

Comparison of pre- and post-bronchodilator data for spirometric and oscillometric parameters. Dotted lines denote the limits of normal. Paired comparisons revealed that the normal control and smoker normal forced oscillation technique (FOT) groups did not demonstrate bronchodilator response of either forced expiratory volume in 1 s (FEV1) or any of the FOT parameters. a) A statistically significant increase in FEV1 was noted in the smoker abnormal FOT group, but an increase >12% was evident in only a single individual. In addition, the smoker abnormal FOT group demonstrated significant bronchodilator response for b) resistance at 5 Hz (R5; p=0.011), c) dynamic elastance as assessed by reactance at 5 Hz (X5; p=0.008) and d) frequency dependence of resistance (R5–20; p=0.022).
In vivo distal lung inflammation
The relationship between presence of distal airway dysfunction and lower airway inflammation is illustrated in figures 2 and 3. Figure 2 illustrates neutrophil and lymphocyte cell counts expressed as concentration per mL ELF. Inflammatory cell counts did not differ between normal control and smoker normal FOT groups. However, the smoker abnormal FOT group had more than two-fold higher median neutrophil and lymphocyte cell counts, compared to the smoker normal FOT group (2.5 (1.7–3.9) versus 1.3 (1.2–1.6)×105 cells·mL-1, p=0.016 versus 10.1 (5.9–16.4) versus 3.7 (1.3–6.8)×105 cells·mL-1, p=0.022, respectively). Levels of three chemoattractant cytokines (IL-8, eotaxin and fractalkine) were significantly higher in the smoker abnormal FOT group compared to the other groups with normal distal airway function (figure 3, p<0.01 for all comparisons). Table 3 shows the correlations that were statistically significant (after adjustment for multiple comparisons) between inflammatory markers and spirometry and FOT parameters (full correlation matrix is available in online supplementary table S1). A statistically significant correlation with FEV1 was not evident for lymphocytes or neutrophils and was only present for IL-12 p70. R20 correlated with neutrophils but not with any chemokine. In contrast, FOT markers of distal airway function (R5–20 and/or X5) correlated with levels of neutrophils, eotaxin, IL-8, fractalkine, IL-12 p70, macrophage inflammatory protein-1α and growth-regulated oncogene.
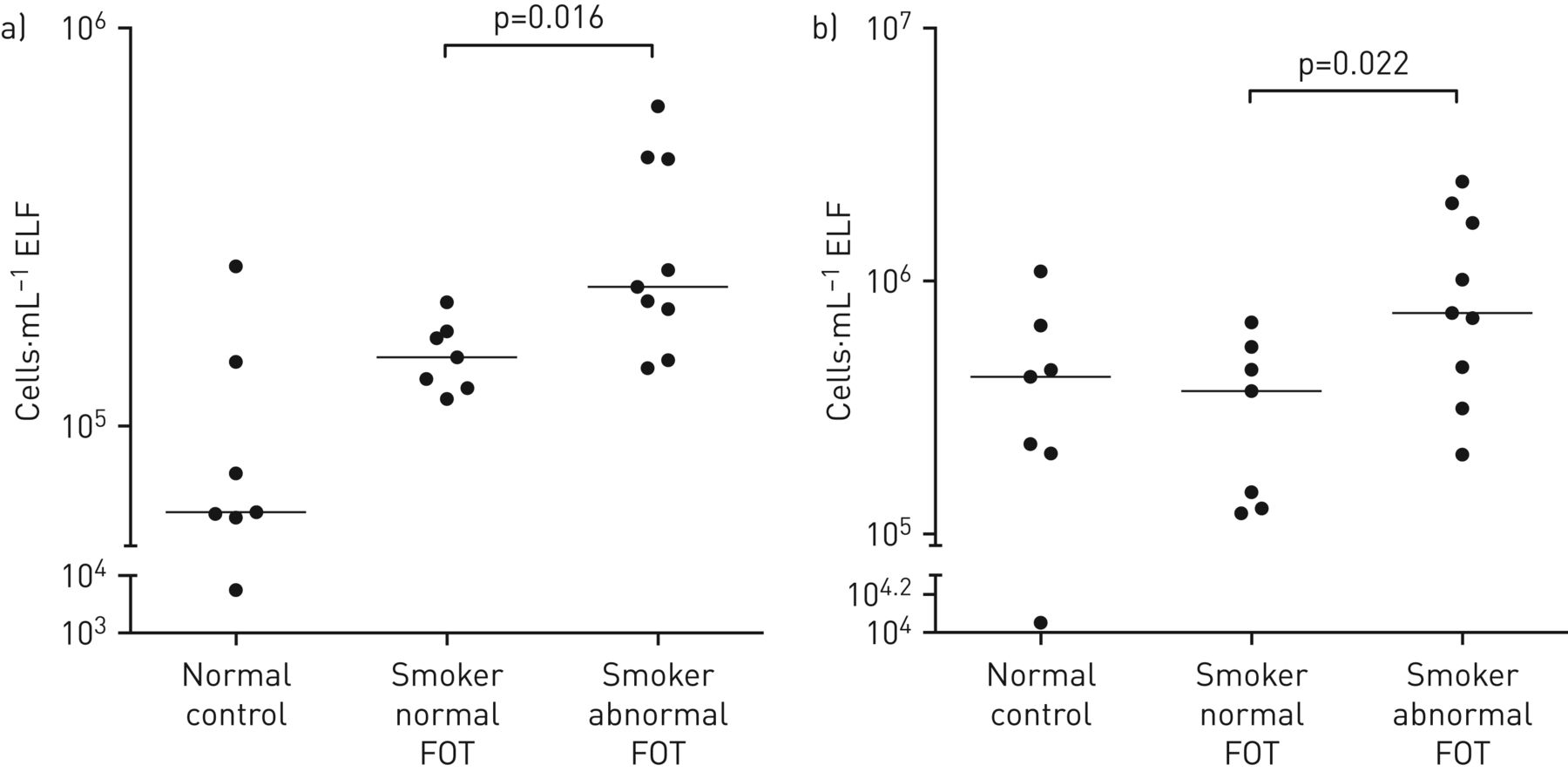
Evaluation of inflammatory cell count in the three groups. Cell counts in epithelial lining fluid (ELF) were plotted on a logarithmic scale for the normal control, smoker normal forced oscillation technique (FOT) and smoker abnormal FOT groups. a) Neutrophil and b) lymphocyte counts were higher in the smoker abnormal FOT group compared with both the smoker normal FOT group (p=0.016 and 0.022, respectively) and the normal control group (p=0.009 and 0.021, respectively).

Concentration of inflammatory cytokines in epithelial lining fluid (ELF) were plotted for the normal control, smoker normal forced oscillation technique (FOT), and smoker abnormal FOT groups. Statistically higher levels of a) interleukin (IL)-8; b) eotaxin; and c) fractalkine were noted in the smoker abnormal FOT group, compared with the smoker normal FOT group (p=0.004, 0.002 and 0.003, respectively).
Correlation between in vivo inflammation and lung function
Airway reactivity and distal lung inflammation
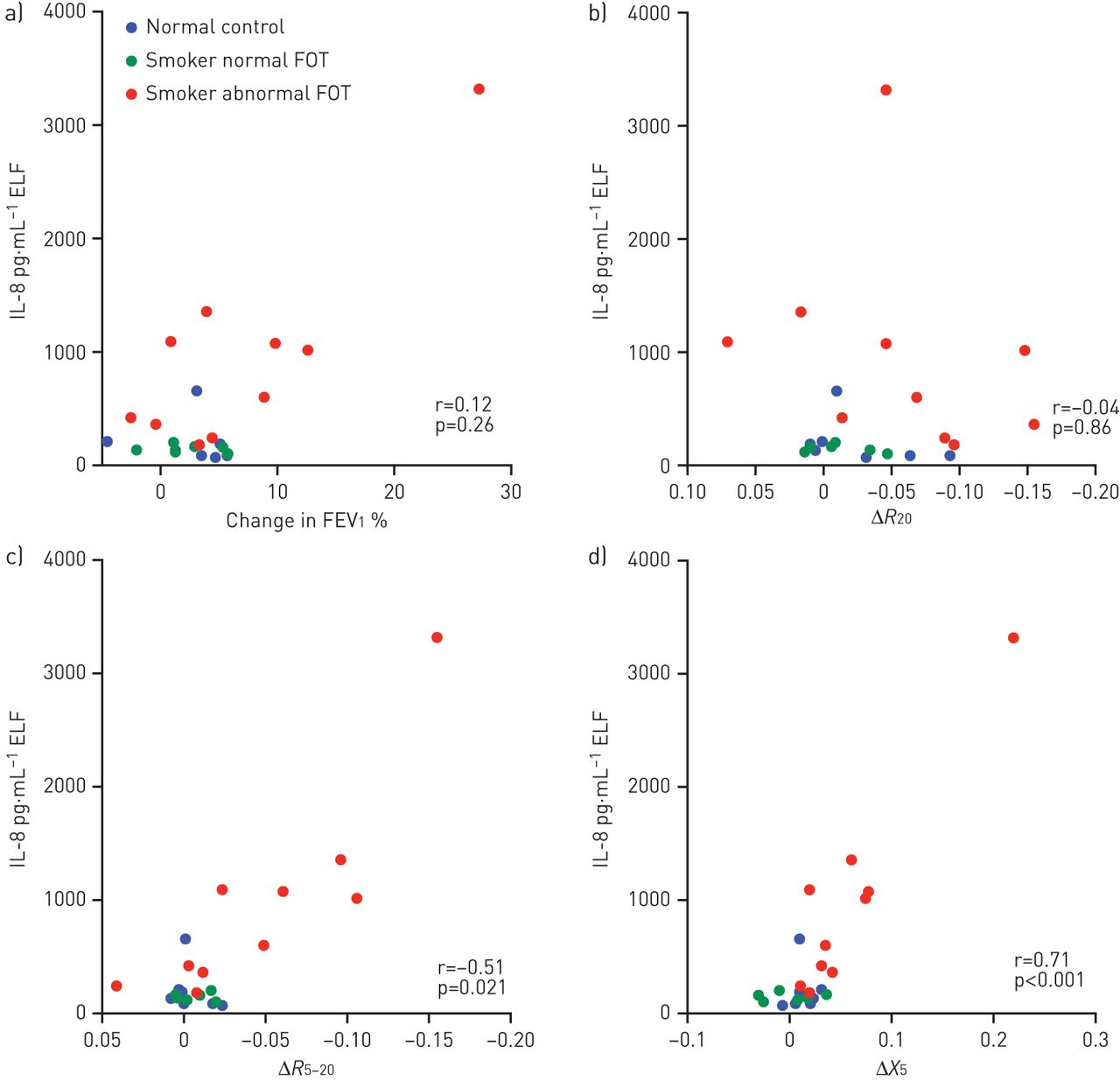
Airways responsiveness has been proposed as an important factor in COPD pathogenesis [18]. Therefore, we evaluated the correlation between magnitude of airway reactivity and degree of in vivo distal lung inflammation. Table 4 shows the statistically significant correlations (after adjustment for multiple comparisons) between inflammatory markers and bronchodilator response when assessed for spirometry and FOT parameters (full correlation matrix is presented in online supplementary table S2). The bronchodilator response FEV1 or R20 did not correlate with either inflammatory cell counts or chemokine levels. In contrast, the bronchodilator response of R5–20 and X5 were correlated with levels of five chemokines in ELF. These correlations remained significant in multivariate models that included BMI and baseline lung function. Correlations were observed for chemokines reflecting multiple immunological pathways including chemoattractant cytokines (IL-8, eotaxin and fractalkine), growth factors (transforming growth factor-α), and T-helper (Th) type 1 cytokines (IL-12 p70). A representative example (IL-8) is illustrated in figure 4. A clear separation is visible between data obtained in the smoker abnormal FOT group, compared with the other subject groups.
Correlation between in vivo inflammation and physiological bronchodilator response

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between bronchodilator response of physiological parameters and concentration of interleukin (IL)-8 in epithelial lining fluid (ELF). Bronchodilator response of a) forced expiratory volume in 1 s (FEV1) and b) resistance at 20 Hz (R20) did not correlate with the level of IL-8 in ELF. In contrast, the bronchodilator response of c) frequency dependence of resistance (R5–20) and d) dynamic elastance as assessed by reactance at 5 Hz (X5) correlated with the level of IL-8 in ELF (r=−0.51, p=0.021 and r=0.71, p<0.001, respectively).
Discussion
This study demonstrates that in asymptomatic smokers a distinct physiological behaviour, consistent with distal lung dysfunction, is associated with subclinical distal lung inflammation. Despite presence of emphysema, these findings occurred at a point during disease progression when post-bronchodilator spirometry remained normal and subjects were asymptomatic and, therefore, a clinical diagnosis of COPD could not be established using GOLD criteria [19]. The pattern of inflammation indicated activation of innate and cellular immune responses. Furthermore, the elevated inflammatory biomarkers in these asymptomatic subjects with distal lung dysfunction have been shown to predict disease progression in patients with established COPD [20, 21]. Thus, investigation of distal lung mechanics in asymptomatic smokers may identify a subgroup of subjects at risk for progression to COPD.
In COPD, lung damage starts in airways of small calibre, producing irreversible tissue destruction and airflow obstruction [22, 23]. Micro-CT of surgical specimens from GOLD stage I patients showed airway narrowing and loss of small conducting airways [24]. However, the contribution of these distal airways to total resistance is minimal and detection of early abnormalities by routine spirometry is limited [25]. Therefore, the spirometric abnormalities required for the diagnosis of COPD occur only later in the course of disease. Based on these considerations, we evaluated FOT markers of distal lung function in smokers who might be at risk for progression to COPD, in accordance with renewed interest in distal lung mechanics in patients with established COPD [26–28].
It has been suggested that abnormal distal lung function might identify clinically relevant phenotypes of COPD [26]. Thus, we investigated the correlation between functional abnormalities of the distal lung and inflammatory biomarkers in the distal lung. In this study, a subgroup of smokers demonstrated physiological abnormalities characterised by frequency dependence of resistance and abnormal dynamic elastance. Frequency dependence of resistance correlates with frequency dependence of compliance and may reflect focal areas of increased small airway impedance with resultant nonuniform distribution of airflow [29]. Although upper airway shunt, glottis closure and chest wall abnormalities may also produce frequency dependence of resistance, these factors cannot explain the observed bronchodilator responsiveness of FOT parameters. Moreover, the correlation with increased subclinical inflammation in the distal lung reinforces our interpretation that the pattern of FOT abnormality reflects distal lung dysfunction. Of importance, this correlation between functional abnormality and inflammation required investigation of distal lung function beyond that which is obtainable from routine evaluation (spirometry, lung volumes and diffusion).
The importance of bronchial responsiveness in COPD pathogenesis has been a matter of debate since the Dutch hypothesis was introduced in 1961 [18]. By convention, responsiveness of spirometric parameters has been the major tool used to investigate airway reactivity. This study extends prior observations by investigation of bronchodilator-elicited reactivity in the distal lung. Bronchodilator responsiveness of distal airway function (R5–20 and X5) was noted in all smokers with abnormal FOT. A predominant smooth muscle mechanism may explain return of distal airway function to the normal range while persistent abnormality suggests potential airway remodelling. In addition, the association between inflammatory markers and distal lung bronchodilator reactivity identifies a phenotype of increased distal lung inflammation. The presence of this correlation prior to the development of fixed obstruction on spirometry is in accord with onset of disease in the distal lung [20, 22]. In addition, the correlation between the degree of distal airway reactivity and magnitude of distal lung inflammation supports a role for airway reactivity in COPD pathogenesis.
The pattern of inflammation observed in subjects with distal lung dysfunction was characterised by elevated inflammatory cells (neutrophils and lymphocytes) as well as elevated chemoattractants (IL-8 and eotaxin) and inflammatory cytokines (fractalkine). These findings are compatible with observations of neutrophilic inflammation in small airways of subjects with early COPD [20, 22] that leads to release of neutrophil elastase and parenchymal destruction [30]. A prior study has demonstrated elevated neutrophils, lymphocytes, IL-8 and eotaxin in sputum obtained from subjects with COPD [31]. In addition, in the present study, fractalkine was elevated, which may indicate activation of lymphocytes, dendritic cells and monocytes/macrophages [32, 33]. Fractalkine is involved in differentiation of Th17 cells [32]. Importantly, levels of IL-17A and IL-22 are increased in sputum of individuals with COPD [34, 35], and Th17 cells have been identified in bronchial biopsies of patients with COPD [36]. Although earlier studies were able to identify subgroups within COPD cohorts with abnormal oscillometry [26–28], this study extends prior observations by correlating oscillometric abnormalities in asymptomatic smokers to in vivo lung inflammation at the site of injury (ELF). In our study, subjects with the most abnormal distal airway function demonstrated activation of innate and adaptive immune responses with a pattern that parallels observations from peripheral airway biopsies in subjects with established COPD [37].
Correlations observed between distal lung reactivity and inflammatory cytokines provide additional insight into disease pathogenesis. The correlations were independent of the baseline abnormality, highlighting that bronchodilator reactivity is an additional clinically relevant marker of distal lung inflammation. These associations included eotaxin, a well-established cytokine associated with bronchial reactivity [38]. Although elevated eosinophils were not observed, as might be expected in asthma [39], elevation of other neutrophilic chemoattractant and Th1 cytokines suggest a different mechanism for bronchodilator responsiveness in COPD. These observations indicate that, in asymptomatic smokers prior to COPD diagnosis using GOLD criteria, both baseline and bronchodilator behaviour of the distal lung are associated with activation of multiple innate immune pathways.
This study is a cross-sectional investigation of asymptomatic smokers with focal mild emphysema incidentally noted on CT performed for cancer screening. The size of the study cohort was limited by the complexity and invasive nature of the assessments. Despite the small number of subjects, a consistent association was demonstrated between physiological behaviour and in vivo inflammation. Progression to clinically evident COPD could not be evaluated and will require longitudinal investigation of larger cohorts. A difference in age was noted between the normal controls compared with the two smoker subgroups. However, the differences in inflammatory cells and mediators were noted in the smoker abnormal FOT group compared with the smoker normal FOT group, despite nearly identical ages. Furthermore, the observed abnormalities in these asymptomatic smokers could reflect concomitant asthma, bronchiolitis or respiratory infection. However, these alternative explanations are unlikely in the absence of clinical symptoms or recent exacerbations. Lastly, while it is biologically plausible to link inflammation with the observed physiological abnormalities, these correlations do not establish causality between these independent measures. Nevertheless, this study serves as a proof of concept, suggesting that the identification of a subset of asymptomatic smokers with a higher degree of lung inflammation may be relevant for developing earlier and more aggressive interventions aimed at halting or attenuating disease progression even before there is significant airflow obstruction or symptoms. Future trials with anti-inflammatory treatment might be warranted in this population.
Subjects were selected for study with the presence of focal mild emphysema on CT, but without COPD based on GOLD criteria. An incidental finding of emphysema is common in smokers [40]. Although the clinical significance of incidentally noted emphysema remains unclear, it was used for study entry since the anatomical abnormality suggests the potential onset of disease at an early stage when COPD was not present according to GOLD criteria. It should be noted that although the radiographic finding was localised to selected region(s), the oscillometry technique assesses global measures of the entire respiratory system, and the field sampled by the BAL technique generally did not correspond to the anatomical location of emphysema noted. These considerations suggest more widespread functional derangements than those demonstrated by the imaging data. The presence of distal airway dysfunction in these asymptomatic smokers with incidental findings of emphysema was associated with pulmonary inflammation despite absence of COPD according to GOLD criteria.
Conclusions
Two novel approaches were used to correlate distal airway function and inflammation in asymptomatic smokers prior to the development of fixed obstruction on spirometry. Abnormalities in distal airway function as assessed by oscillometric frequency dependence of resistance and reactance are associated with increased in vivo lung inflammation. These functional abnormalities were not identifiable on the basis of routine pulmonary function parameters. Thus, the present study demonstrates that distal lung dysfunction and bronchodilator reactivity are physiological expressions of a phenotype characterised by distal lung inflammation that parallels reported observations in established COPD.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary tables 00066-2016_Supplementary_Tables
Disclosures
Footnotes
This article has supplementary material available from openres.ersjournals.com
Support statement: This study was supported by US National Institute for Occupational Safety and Health grant 200-2011-39413 and US National Institutes of Health grants K23 AI102970 and UL1 TR000038. Funding information for this article has been deposited with the Open Funder Registry.
Conflict of interest: Disclosures can be found alongside this article at openres.ersjournals.com
- Received June 3, 2016.
- Accepted October 10, 2016.
- Copyright ©ERS 2016.
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










