





Abstract
Several studies in patients with chronic obstructive pulmonary disease (COPD) have shown that whole-body vibration training (WBVT) has beneficial effects on exercise capacity. However, the acute cardiopulmonary demand during WBVT remains unknown and was therefore investigated in this study.
Ten patients with severe COPD (forced expiratory volume in 1 s: 38±8% predicted) were examined on two consecutive days. On day one, symptom-limited cardiopulmonary exercise testing was performed on a cycle ergometer. The next day, six bouts of repeated squat exercises were performed in random order for one, two or three minutes either with or without WBVT while metabolic demands were simultaneously measured.
Squat exercises with or without WBVT induced comparable ventilatory efficiency (minute ventilation (VE)/carbon dioxide production (V′CO2): 38.0±4.4 with WBVT versus 37.4±4.1 without, p=0.236). Oxygen uptake after 3 min of squat exercises increased from 339±40 mL·min−1 to 1060±160 mL·min−1 with WBVT and 988±124 mL min−1 without WBV (p=0.093). However, there were no significant differences between squat exercises with and without WBVT in oxygen saturation (90±4% versus 90±4%, p=0.068), heart rate (109±13 bpm versus 110±15 bpm, p=0.513) or dyspnoea (Borg scale 5±2 versus 5±2, p=0.279).
Combining squat exercises with WBVT induced a similar cardiopulmonary response in patients with severe COPD compared to squat exercises without WBVT. Bearing in mind the small sample size, WBVT might be a feasible and safe exercise modality even in patients with severe COPD.
Abstract
Whole-body vibration training is a feasible and safe exercise modality even in patients with severe COPD http://ow.ly/FNK5307VSPC
Introduction
Whole-body vibration training (WBVT) is characterized by an external stimulation inducing an oscillation vibration to a subject standing on a vibration platform. A central mechanism of WBVT is elicited by the tonic vibration reflex that provokes involuntary, monosynaptic-triggered muscle contractions, especially in the lower extremities [1, 2]. Several studies have observed beneficial effects of WBVT on balance, muscular power and bone density in subjects with various chronic disorders [3]. Although WBVT itself is not a novel medical exercise therapy, the first study on the effects of WBVT in patients with chronic obstructive pulmonary disease (COPD) was not published until 2012 [4]. Currently there are very few studies available that investigate WBVT in patients with COPD. In a recently published systematic review, our work group identified six studies (including 235 COPD patients) applying WBVT in different approaches and settings (e.g. WBVT versus passive control group, WBVT on top of endurance and strength training, WBVT during acute exacerbation) [5]. It was concluded that WBVT seems to be superior in improving functional exercise capacity in comparison to conventional exercise strategies. The underlying mechanisms of these benefits remain unclear but it is improvements in the neuromuscular system in particular that are speculated to cause these gains in exercise performance [5].
Furthermore, it remains unclear if patients experience greater cardiopulmonary stress during WBVT caused by the greater excitation of the lower extremity muscles. So far only one study [6] has measured heart rate and oxygen saturation in patients with moderate COPD standing on a vibration platform versus a sham WBVT; the authors found no significant differences. However, squat exercises, which are the most common types of exercise on WBVT platforms [5] and imply greater cardioventilatory demand, were not investigated. In addition, a more sophisticated assessment of spiroergometry parameters during WBVT has not yet been performed. Therefore, the primary aim of this study was to evaluate the acute cardiopulmonary demand in patients with severe COPD performing dynamic squat exercises with and without WBVT.
Methods
Study design
Patients admitted to a 3-week inpatient pulmonary rehabilitation programme at the Schoen Klinik Berchtesgadener Land (Schoenau am Koenigssee, Germany) between May 2013 and May 2015 were screened for eligibility. All measurements were performed on two consecutive days at the beginning of the pulmonary rehabilitation programme. The trial was approved by the Ethics Committee of the Bavarian Physician Association (identification number 12 099) and registered at clinicaltrials.gov (NCT01898143).
Study population
Inclusion criteria were a confirmed diagnosis of COPD stage III or IV according to the Global Initiative for Chronic Obstructive Lung Diseases (GOLD) [7] in a stable condition, inexperience with WBVT, and the ability to read and understand the German language and study procedures. Exclusion criteria were severe acute COPD exacerbation necessitating a change in medication or new onset of symptoms persisting for more than 3 days, alveolar oxygen tension (PaO2) during cardiopulmonary exercise testing of <55 mmHg requiring supplemental oxygen, and any contraindication for the use of WBVT (e.g. deep vein thrombosis, activated arthritis, acute discopathy). All participants gave written informed consent before taking part in the study.
To familiarise patients to WBVT, patients participated in one or two exercise practice sessions with the WBVT platform a few days prior to beginning the study intervention.
Intervention day 1: maximal cardiopulmonary exercise testing
Patients performed symptom-limited, maximal, incremental cardiopulmonary exercise testing (CPET) on a cycle ergometer to generate baseline data. CPET was performed in accordance with the guidelines of the American Thoracic Society and American College of Chest Physicians [8]. A mouthpiece with an integrated flow sensor collected breath-by-breath measurements of gas exchange and ventilation.
Intervention day 2: squat exercise protocol
All patients performed a sequence of different exercise bouts during a total duration of about 1 h (figure 1). Patients wore a mask for respiratory gas collection and analyses for the total test duration (figure 2). Testing began with a 10 min cycling session at 60% of peak work rate. This cycling period served as a warm-up procedure and was also used as a reference for comparing cardiopulmonary stress during WBVT with a conventional exercise modality. After 5 min of rest patients performed six short bouts of paced squatting exercises (in random order) for the duration of 1, 2 or 3 min either on the floor or on a side-alternating WBVT-platform (Galileo®, Novotec Medical, Pforzheim, Germany). Patients controlled their squat form and timing while exercising by mimicking a video recording of a model performing squats in the ideal execution form (knee and hip flexion: 90–100°) and timing. The squat exercises were timed so that the patients were in motion for 4 s (2 s concentric and 2 s eccentric) followed by 2 s standing between each repetition, yielding 10 repetitions per minute. An experienced exercise instructor (R.G.) was present and corrected the patients’ movement and controlled for skidding as necessary. After each exercise bout, patients rested for 5 min while seated. Squat exercises during WBVT were performed at a frequency of 26 Hz and a peak-to-peak displacement of 5 mm (parameters that are usually used in WBVT trials including COPD patients [4, 9, 10]). Patients wore flat-soled shoes.

Study flow chart. CPET: cardiopulmonary exercise testing; PWR: peak work rate; WBV: whole-body vibration.

Patient during squat exercises a) with and b) without whole-body vibration training under spiroergometric conditions (the patient provided written consent for photographs).
Hypothesis
The primary hypothesis was that performing squat exercises with WBVT will induce higher cardiopulmonary stress than performing squat exercises on the floor without WBVT.
Outcomes and measures
The ergospirometry system MasterScreen CPX (CareFusion, Hoechberg, Germany) and the software LabManager V5.3.0 (Cardinal Health, Hoechberg, Germany) were used to perform CPET and generate CPET data. Resting and peak measures of all ergospirometry outcomes were calculated as mean values recorded during eight final breaths of each interventional period. Specifically, resting and peak measures of oxygen uptake (V′O2, mL·kg−1·min−1), minute ventilation (VE, L·min−1) and respiratory rate (L·min−1) were recorded. Resting/peak measures of heart rate (beats per minute) and arterial oxygen saturation (SpO2, %) were both measured by pulse oximetry using a Sat 801 pulse oxymeter (HUM, Luenen, Germany). The PaO2 (mmHg) and arterial carbon dioxide tension (PaCO2, mmHg) were determined via capillary blood gas analysis on samples taken from the earlobe. Ratings of perceived exertion for dyspnoea and leg fatigue at the end of each bout of squat exercises were rated using the modified Borg scale (0 to 10 points).
Baseline lung function was measured with a MasterScreen body plethysmograph (Jaeger, Wuerzburg, Germany) in accordance with current guidelines [7, 11]. Peak isometric knee-flexion and extension was measured using a handheld dynamometer (MicroFET2; Hoggan Scientific LLC, Salt Lake City, UT, USA). The 6-min walk test was performed in accordance with the current American Thoracic Society/European Respiratory Society statement [12] and fat-free mass was measured by bioelectrical impedance analysis (NutriGuard MS, Input Data, Poecking, Germany).
Blinding and randomisation
The blinding of investigators or study participants was not possible within the study setting. However, all data analyses were performed by a statistician who was not involved in any other aspects of the study and was blinded to allocation.
A computer-based random number generation program was used to randomly order the six different bouts of squat exercises individually for each patient.
Statistical analyses
Results are presented as mean±sd unless specified otherwise. Dependent group comparisons were performed by Wilcoxon signed rank test. The significance level was set at alpha=0.05 and all tests were two-sided. All analyses were performed using SPSS (version 18.0; SPSS Inc., Chicago, IL, USA).
Results
In total, 67 patients were screened for eligibility. Of these, 53 (79%) did not meet the inclusion criteria (PaO2 during CPET <55 mmHg) and 4 (6%) refused to participate. A final total of 10 patients were included in the study and were able to complete the trial investigations. Patients (age: 62±8 years, 30% women) presented with severe airflow obstruction (forced expiratory volume in 1 s (FEV1): 38±8% predicted), had an impaired exercise capacity (6-min walk test distance: 68±16% predicted) and a low peak work rate (75±29% predicted). Patients presented with a well-preserved fat-free mass of 109±14% of predicted as well as a peak quadriceps force of 96±16% of predicted. In 9 out of 10 patients, CPET was terminated owing to exhaustion due to dyspnoea and/or leg fatigue. In one patient, CPET was stopped by the physician because the patient reached an arterial systolic blood pressure of >250 mmHg [13]. None of the patients showed cardiac arrhythmia or signs of ischaemia in an ECG during CPET. Patient comorbidities included arterial hypertension (n=4), osteoporosis (n=3), type 2 diabetes (n=1) and peripheral vascular disease (n=1). Baseline patient characteristics are listed in table 1.
Patient characteristics
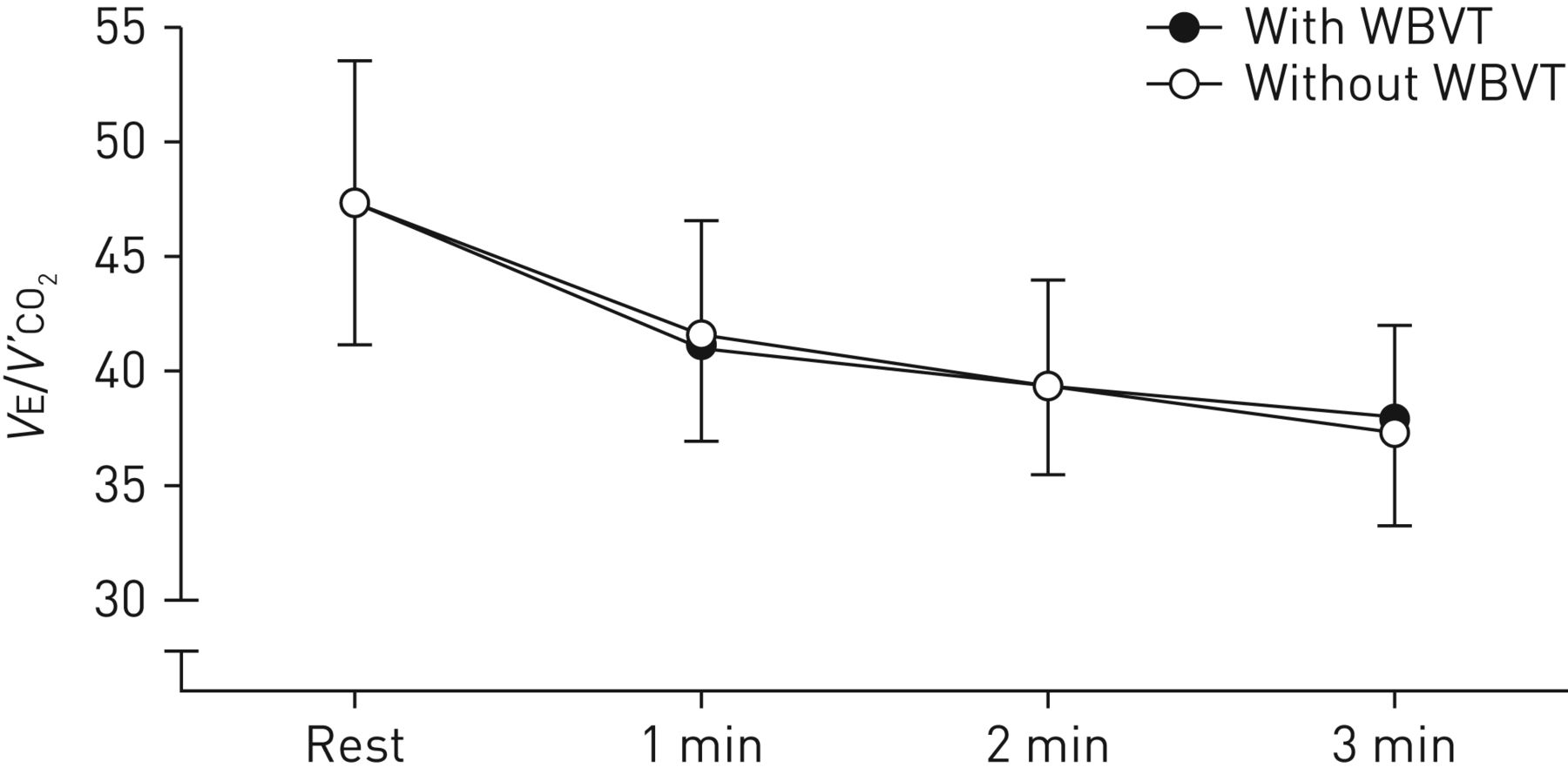
There were no missing values for any of the measured outcome parameters. Main outcomes are listed in table 2. Ventilatory efficiency was not significantly different after 1, 2 or 3 min of squat exercises with or without WBVT (figures 3 and 4). Oxygen saturation showed nominally significant differences during 1 min (with WBVT: 92±3%; without WBVT: 91±3%; p=0.028) and 2 min of exercise (with WBVT: 91±3%; without WBVT: 90±3%; p=0.024), though these differences are not clinically relevant [14]. Respiratory rate was significantly different after 2 min (with WBVT: 26±5 breaths·min−1; without WBVT: 23±4 breaths·min−1; p=0.008) and 3 min (with WBVT: 27±5 breaths min−1; without WBVT: 23±3 breaths min−1; p=0.007). No other variables (oxygen uptake, VE, heart rate and perceived exertion for dyspnoea and leg fatigue) showed significant differences between squat exercise with and without WBVT.
Overview on main outcomes
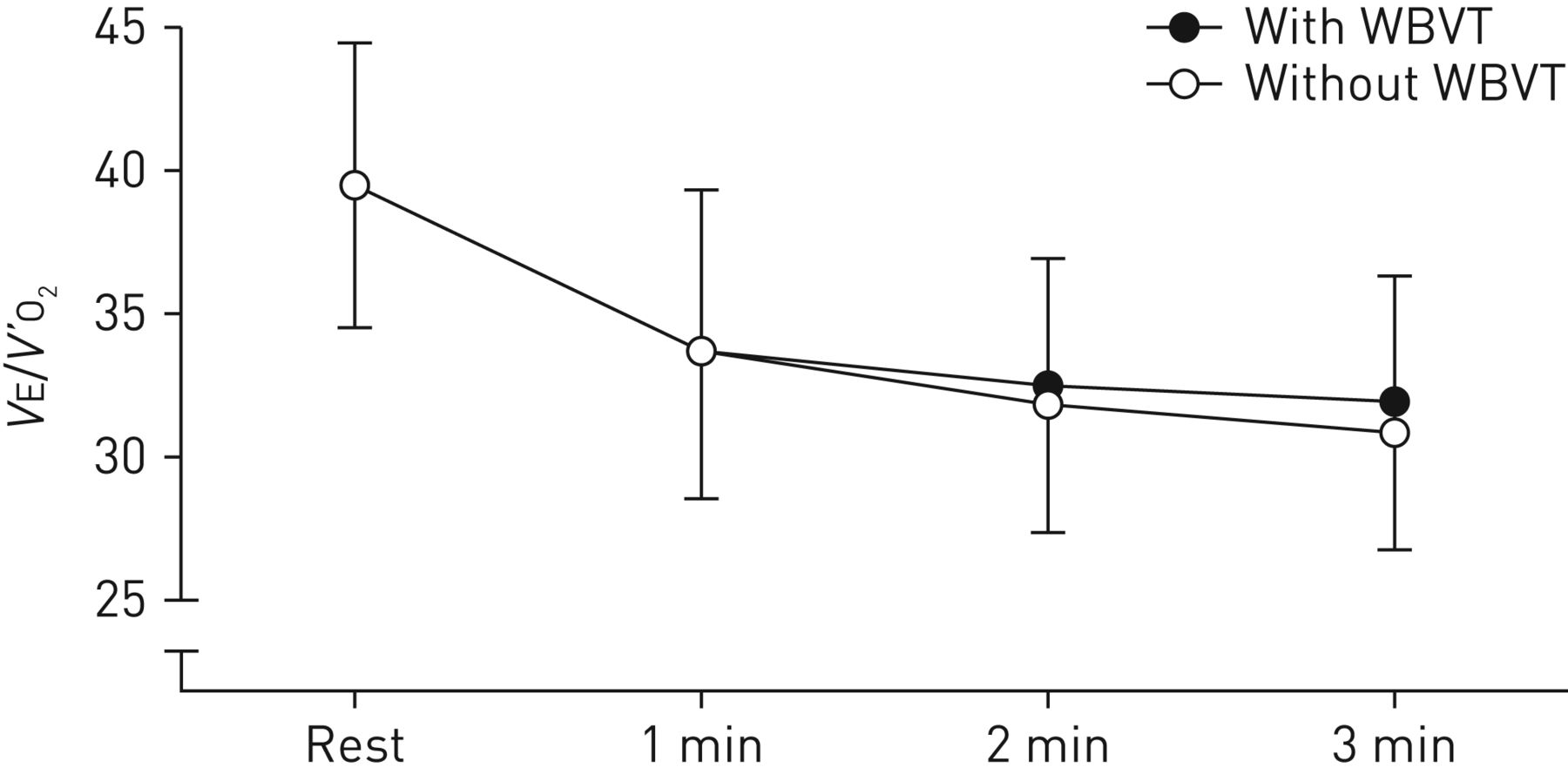
Ratio of minute ventilation to oxygen uptake (VE/V′O2) during squat exercises with and without whole body vibration training (WBVT).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ratio of minute ventilation to carbon dioxide output (VE/V′CO2) during squat exercises with (closed circles) and without (open circles) whole body vibration training (WBVT).
There were no adverse events related to the study intervention.
Discussion
Cardiopulmonary demand during squat exercises on a whole-body vibration training platform
The present study found that squat exercises with WBVT did not alter cardiopulmonary parameters or patient-related symptoms compared to squat exercises without WBVT. This is an important finding because it indicates the cardiopulmonary safety of WBVT even in patients with severe COPD (without significant comorbidities).
Recently, several studies [4, 10, 15–17] have shown that WBVT results in superior exercise performance in patients with COPD. However, it remained unknown whether the cardiopulmonary stress during WBVT was much greater. The aim of the current study was therefore to assess the cardiopulmonary response to a popular therapeutic exercise (squat) with and without WBVT in patients with severe COPD to assess its feasibility and safety.
An earlier study in healthy subjects showed that simply standing on a WBVT platform increases energy expenditure comparable to moderate-intensity walking, and that V′O2 increases with the frequency, amplitude and additional load of WBVT [18]. In a study by Rittweger et al. [19], 12 young healthy subjects performed 3 min of squat exercises with and without WBVT in a similar approach to the current study. V′O2 during squat exercise on the floor was 11±3 mL·kg−1·min−1 compared to 14±3 mL·kg−1·min−1 with WBVT (p<0.05). These absolute values were similar to those observed in the current study (10±1 mL·kg−1·min−1 versus 11±2 mL·kg−1·min−1). However, the relative intensities were only 33% of peak V′O2 in the healthy subjects, whereas in our patients with severe COPD it was 80% of their peak V′O2. Furthermore, in the current study performing 3 min of squat exercise with WBVT resulted in a 10% increase in VE (nonsignificant) and a 20% increase (p<0.01) in respiratory rate compared to exercising on the floor. It is assumed that WBVT recruits previously inactive motor units, which would result in a higher respiratory rate. Also, the vibration stimulus may lead to involuntary spontaneous breathing related to an increase in neural inspiratory drive [20]. However, during exercise there was a physiological decline of ventilator efficiency (VE/V′O2 and VE/V′CO2) as an indicator of an improved ventilation–perfusion relationship and a reduction in dead-space ventilation. This clearly shows that there is no difference in ventilatory requirements between performing squat exercises with or without WBVT. Furthermore, other relevant parameters, including oxygen uptake, minute ventilation and perceived exertion, were not significantly different between squat exercises with or without WBVT. However, the use of further measurement techniques like electromyography or near-infrared spectroscopy might have provided further detailed insights into the metabolic responds during WBVT.
In general, peak V′O2 and VE levels during 3 min of squat exercises with WBVT were moderate. Both values were significantly below the values obtained during 10 min of cycling at 60% of peak work rate, which is a common suggested training intensity [21]. Cardiopulmonary stress during 3 min of squat exercising with WBVT was even lower than that observed in COPD patients during walking on level ground at a moderate speed of 4 km·h−1 [22]. Furthermore, dyspnoea, leg fatigue, heart rate and oxygen saturation were comparable for squat exercises with and without WBVT, indicating that the increase in respiratory rate may not be related to other clinically relevant parameters.
It should further be considered that patients in the current study performed squat exercises at a given pace and range of motion, controlled by study personnel. Patients that perform squat exercises in a more “real-life” training setting might choose their own velocity and number of repetitions and that may influence ventilatory demand [18].
Clinical relevance
This study has shown that adding WBVT to squat exercises does not induce higher cardiopulmonary stress in patients with severe COPD. This finding is of great relevance because it provides important evidence on the feasibility and safety of WBVT.
In the current study, patients also performed 3 min of just standing on the WBVT platform without any squat exercise. This resulted in a significant but only moderate increase in cardiopulmonary parameters. Recent studies have shown that standing on a WBVT platform can be an effective exercise modality to increase exercise capacity in COPD patients during an acute exacerbation [10], in intensive care patients [23] and in patients directly following lung transplantation [24]. In this context, WBVT may be appropriate even for more seriously disabled patients who are physically unable to perform dynamic squat exercises.
The current study has shown that WBVT is feasible and safe in patients with severe COPD. It has also been proven in healthy elderly patients that a dynamic squat exercise training programme can be more effective in improving balance performance and muscular power than simply standing on a WBVT platform [25]. Therefore, a dynamic squat WBVT programme seems to be preferable to isometric WBVT.
Strengths and limitations of this study
Performance of squat exercises was highly standardised (comprehensive briefing of patients prior to the study, squat video instructions and one-to-one guidance from an experienced instructor). This procedure has enabled a reliable comparison between standardised squat exercises with and without WBVT.
However, this study investigated only a small sample size, and larger adequately powered studies should further investigate the cardiopulmonary demand of WBVT in patients with COPD. Different vibration frequencies should also be investigated. Furthermore, only patients with severe COPD but without an indication for supplemental oxygen during exertion were included. Therefore, these findings cannot be extrapolated to speculate on the ventilatory demands during WBVT in patients under supplemental oxygen therapy. However, performing cardiopulmonary procedures in these patients without supplemental oxygen is not possible owing to ethical issues.
Conclusion
Combining squat exercises with WBVT in patients with severe COPD did not affect ventilatory requirements compared to squat training without WBVT. Adding WBVT to squat exercises was well tolerated and did not further increase patient-related symptoms. Although former studies have demonstrated a positive effect of WBVT on exercise capacity in patients with COPD, we did not find an acute increase in cardiopulmonary stress during squat training with WBVT. Although only a small sample size was investigated, WBVT could be an effective, safe and feasible exercise modality in patients with stable severe COPD (without significant cardiovascular comorbidities).
Acknowledgements
Authors’ contributions: RG and KK were responsible for the study concept and design; RG, PR and SW were responsible for the acquisition of data; RG, CN and JWC were responsible for the analysis and interpretation of data; RG was responsible for drafting the article; all authors were responsible for providing scientific discussion and revising the manuscript critically for important intellectual content. RG had full access to all study data and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
This study is registered at clinicaltrials.gov with identifier number NCT01898143.
Conflict of interest: None declared.
- Received September 22, 2016.
- Accepted December 10, 2016.
- Copyright ©ERS 2017
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










