





Abstract
Tuberculosis (TB) diagnostics are centralised, requiring long-distance transportation of specimens in most resource-limited settings. We evaluated the ability of OMNIgene.SPUTUM (OM-S) to obviate cold-chain transport of TB specimens.
A two-arm (same-day and after 5 days sample processing) study was conducted to assess contamination rates and Mycobacterium tuberculosis viability in OM-S-treated samples against the standard decontamination procedure (SDP) in Mozambique, using Lowenstein Jensen (LJ) and mycobacterial growth indicator tube (MGIT) culture and molecular bacterial load assay.
270 specimens were processed using OM-S and SDP in same-day and 5-day arms. Contamination was lower in OM-S-treated than SDP-treated cultures: 12% versus 15% and 2% versus 27% in the same-day and 5-day arms, respectively. M. tuberculosis recovery in OM-S-treated LJ cultures was 10% and 56% higher in the same-day and 5-day arms, respectively, than SDP-treated cultures, but lower in MGIT (52% and 28% lower in the same-day and 5-day arms, respectively). M. tuberculosis viable count was 1log estimated CFU·mL−1 lower in 5-day OM-S-treated sputa. OM-S was more effective at liquefying sputum with a shorter sample processing time: 22 min for culture.
OM-S is simple to use and has demonstrated a high potency to suppress contaminants, maintenance of viability at ambient temperatures and higher M. tuberculosis recovery, particularly in the solid LJ cultures. Optimisation of OM-S to achieve higher MGIT culture positivity and shorter time to result will increase its application and utility in the clinical management of TB.
Abstract
OMNIgene.SPUTUM obviates cold-chain transport by removing contaminants and keeping viability at ambient temperature http://ow.ly/z38U30hJEnF
Introduction
Tuberculosis (TB) remains a global health threat. Considering the World Health Organization (WHO) 2035 vision to eliminate TB, new approaches for effective management of the disease have never been more urgent [1]. Culture is the gold standard for TB diagnosis and treatment monitoring, and is the main method for drug sensitivity testing (DST) [2, 3]. The stringent biosafety requirements of TB culture have led to overcentralisation of culture services in most low- to medium-income countries [4]. This means that specimens referred for culture often take days or weeks to reach reference laboratories. For example, Mozambique, a country with a high TB burden with a population of 28 million people spread over an area of 801 590 km2, is currently served by only three TB culture laboratories, one of which is a national reference laboratory. This translates to one laboratory per 9.3 million people per 267 196 km2. Even when Mozambique responds to the current WHO framework for universal DST and establishes three more culture laboratories, this ratio will still be as high as a single culture laboratory per 5 million people in an area of 26 753 km2 [5]. In such a situation, the need for an effective sample transportation system cannot be overemphasised.
The current recommendation for TB culture processing is that samples should be transported under cold conditions (2–8°C) and should reach the laboratory and be processed within 24 h or 48 h if coming from distant collection centres [6]. While in high-resource settings this may be achieved with efficient courier systems and resources to afford cold-chain transport, it is far from reality in low-resource settings. Cold conditions are believed to suppress growth of contaminant organisms and preserve the viability of Mycobacterium tuberculosis for culture and other downstream diagnostic methods [6]. Given the shortage of cold-chain sample transportation and considering that specimens must often be shipped in high-temperature, high-humidity environments, alternative effective and affordable means of sample transport are urgently needed.
The novel reagent OMNIgene.SPUTUM (OM-S; DNA Genotek, Ottawa, ON, Canada) liquefies and decontaminates sputum, and preserves M. tuberculosis viability during transport. OM-S is simply added at 1:1 ratio to sputum at the point of collection, and the specimen is then transported at ambient temperature to the processing laboratory. The combined functions of OM-S simplify transport as well as the processing of sputum samples for downstream TB diagnostic assays [7, 8]. Failure to remove contaminants allows growth of non-M. tuberculosis organisms, which can generate false-positive results, particularly in automated liquid culture systems such as the mycobacterial growth indicator tube (MGIT; Becton, Dickinson and Company, Franklin Lakes, NJ, USA). When a culture is contaminated, that culture must either be repeated with a fresh decontamination procedure or else a new sample must be requested from the patient [6]. This increases costs and prolongs time to diagnosis and treatment. A pre-analytical tool that effectively removes contaminating flora from sputum and preserves viable M. tuberculosis would benefit clinical diagnosis and management of TB disease. Viable M. tuberculosis is required for culture and for molecular assays, such as molecular bacterial load assay (MBLA) which quantifies viable M. tuberculosis in sputum [9–11], molecular DST [12] and genomics [13]. Unlike PrimeStore transport medium, which eliminates viability by killing M. tuberculosis and is only suitable for downstream molecular assays, OM-S maintains viability important for culture and culture-based DST [14]. Previous evaluation reports demonstrate compatibility of OM-S-treated samples with using Lowenstein Jensen (LJ), MGIT and Xpert, with TB detection results comparable to standard of care in these tests [7, 8, 15].
This study evaluated the performance of OM-S for TB sputum decontamination and preservation of M. tuberculosis viability at ambient temperature compared to standard sputum processing (N-acetyl-l-cysteine (NALC) and sodium hydroxide (NaOH)) in Mozambique. Our study probed beyond qualitative detection and ascertained OM-S impact on M. tuberculosis viable count, using the novel MBLA, time to culture positivity and operational utility.
Methods
Study design and sample processing
The study was conducted between October 2015 and August 2016, using the Mozambique National TB Reference Laboratory in Maputo city as a central processing laboratory. The aim of the study was to evaluate OM-S for sputum liquefaction, decontamination and preservation of M. tuberculosis viability. 139 patients were recruited from two peripheral TB clinics (Chamanculo General Hospital, 6 km away and Boane Health Centre, 40 km away) and one TB diagnostic study centre (APOPO) in Maputo city and province, 6 km away. Smear-positive sputa from new TB cases or cases having received <1 month anti-TB treatment were included in the study. Use of smear-positive sputa ensured the presence of M. tuberculosis in the sample prior to viability assessment with the different treatments.
The investigation was designed to maximise assessment of OM-S versus standard decontamination procedure (SDP) for culture, which is the homogenisation of sputum with NALC/NaOH for 15 min at room temperature. Patients' samples were assigned to one of two study arms: the same-day (SD) arm (samples processed within 7 h of reaching the laboratory) tested short-term exposure to OM-S, and the 5-day (5-day) arm (samples incubated for 5 days at room temperature prior to processing) mimicked the longer transit times required for specimens to reach many reference laboratories. Experience in Mozambique and other high TB burden countries in Africa is that cold-chain transport is never a reality, resulting in the transport at ambient temperature of the majority of samples from further afield.
Same-day arm (n=78)
At the healthcare centre, each raw sputum sample was divided into equal fractions. One had an equal (1:1) volume of OM-S added to it on site, and the other (control sample destined for SDP) was not treated. OM-S-treated samples were transported to the central laboratory at ambient temperature, and a refrigerated cold box was used for control samples. The accurate addition of equal volume of OM-S at collection site or central lab was assured by using a graduated 50 mL centrifuge tube.
On arrival at the laboratory, 1 mL of each sample was preserved in 1:4 guanidine thiocyanate (GTC) (Promega, Southampton, UK) solution with 1% β-mercaptoethanol v/v (Sigma Aldrich, Gillingham, UK) and stored at −80°C for MBLA. Prior to preservation in GTC, the OM-S-treated sample was centrifuged at 3000×g for 15 min to remove OM-S and the sediment was resuspended in 1 mL PBS. The remaining portion of each OM-S-treated sample was centrifuged for 15 min at 3000×g. The sediment was resuspended in 1 mL PBS, and this was used to inoculate MGIT and LJ cultures (see details later). The control sputa were decontaminated in NALC/1.5% NaOH at 1:1 volume to the sample for 15 min at room temperature. An equal volume of PBS was then added, followed by centrifugation at 3000×g for 15 min. The supernatant was removed and the sediment was resuspended in 1 mL PBS. Fresh NALC/NaOH solution was prepared daily.
5-day arm (n=57)
Raw sputum samples were collected and transported to the central laboratory. One had an equal (1:1) volume of OM-S added at the laboratory, and the other (control) was not treated; both were incubated at room temperature (recorded daily; range 29–34°C) for 5 days, after which the control sample was subjected to SDP. The OM-S and SDP samples were processed for MGIT, LJ and MBLA as described for the same-day study arm.
Culture
MGIT tubes were inoculated with 500 μL of resuspended sediment and then incubated at 37°C in the BACTEC 960 MGIT system. LJ slants were inoculated with 200 μL of resuspended sediment and kept at 37°C in a standard incubator. TB-positive cultures were confirmed by the presence of acid-fast bacilli on Ziehl–Neelsen staining and presence of antigen MPT64. Absence of acid-fast bacilli cording, and growth on blood agar within 24 h was recorded as contamination. Time to culture positivity (TTP) was recorded in days for MGIT and in weeks for time to colony appearance on LJ agar. Colony density on LJ slants was scored as countable (1–200 colonies) and uncountable (>200 colonies). A negative result was declared if the MGIT tube was negative at 42 days or no growth was detected on LJ at 8 weeks.
MBLA
On the day of testing, samples were removed from the −80°C freezer, thawed at room temperature, spiked with 100 μL of the internal extraction control and then centrifuged for 15 min at 3000×g to form a sediment [16]. RNA was isolated using the Fast Prep RNA pro blue kit (MP Biomedicals, Santa Ana, CA, USA), following the manufacturer's instructions.
Duplex reverse transcriptase qPCR targeting both M. tuberculosis and the internal control was performed on a RotorGene 5plex platform (Qiagen, Manchester, UK) using primers and TaqMan dual-labelled probes (all primers and probes; MWG Eurofins, Ebersberg, Germany). The optimal PCR cycling conditions were as reported by Honeyborne et al. [10]. Cycle threshold values were translated to bacterial load values using a standard curve customised for the site's quantitative PCR platform and recorded as estimated colony forming units per mL (eCFU·mL−1) [16]. In every PCR run, positive and negative (no template) controls were run alongside samples.
Operational assessment
Sample processing time and associated apparatus were recorded. Extent of sputum liquefaction was noted by user inspection of reagent–sputum mixtures and the ease of pipetting. The manufacturer's price of OM-S was recorded and used to calculate the cost per sample, that is, the number of samples processed divided by the price of the reagent. The cost of SDP was calculated based on the Global Fund to Fight AIDS, Tuberculosis and Malaria (subsidised) prices of constituents for decontaminating a 5-mL sputum sample. The costings do not include estates charges, utility costs, labour or technician's time.
Analysis
All analyses were done using GraphPad Prism v.6 (GraphPad Software, La Jolla, CA, USA) and Excel for Mac 2011 (Microsoft, Redmond, WA, USA). Differences between the OM-S and SDP treatment groups with respect to TTP and bacterial load were analysed using the Mann–Whitney U-test. Spearman's rank correlation was used to assess the correlation between MGIT TTP and bacterial load for each group. Positivity, negativity and contamination rates were calculated for each assay as ratio to the number of samples tested.
Ethics approval
The study was approved by the medicine ethics committee on behalf of the university teaching and research ethics committee for the University of St Andrews (MD11983) and by the Instituto Nacional de Saude institutional review board and national ethics committee for Mozambique (97/CNBS/16).
Results
Samples
Of the 270 total OM-S-treated and SDP-treated specimens, 176 (78 pairs, 65%) were processed in the same-day arm and 114 (57 pairs; 42%) were processed in the 5-day arm. The average room temperature was 34°C in the summer months of the study (October 2015 to March 2016) and 29°C in the winter months (April to July 2016).
Decontamination efficiency
On average, the culture contamination rate was lower in the OM-S-treated samples than those treated with the SDP, 12% versus 15% in the same-day arm and 2% versus 27% in the 5-day arm. Decontamination efficiency of the SDP was poorer in the untreated sputa (control) incubated at ambient temperature for 5 days, resulting in 21% and 32% contaminated MGIT and LJ cultures, respectively. In contrast, only 2% MGIT and 4% LJ cultures of OM-S-treated sputa were contaminated after 5 days of incubation (table 1).
Comparison of culture contamination rates for the two treatment groups in each study arm
Recovery and detectability of TB
Measured by the number of TB-positive cultures, the rate of M. tuberculosis recovery for OM-S-treated LJ cultures was 10% (79% versus 69%) and 56% (84% versus 28%) higher than SDP-treated LJ cultures in the same-day and 5-day arms, respectively. In contrast, M. tuberculosis recovery in OM-S-treated MGIT was 52% (31% versus 83%) and 28% (47% versus 75%) lower than in SDP-treated MGIT culture in the same-day and 5-day arms respectively. Interestingly, both treatment arms showed high TB detectability (96–100%) with MBLA, a viable count assay (table 2).
Rates of Mycobacterium growth indicator tube (MGIT), Lowenstein Jensen (LJ) positivity and negativity by treatment group in each study arm
For the positive LJ cultures, colony density scoring showed no significant difference between OM-S and SDP treatment. In the same-day arm, 74% (n=54) SDP versus 83% (n=58) OM-S LJ cultures had countable colonies with the remaining 26% and 17%, respectively, being uncountable. The cultures with countable colonies were 87.5% in both OM-S (n=48) and SDP (n=16), and the uncountable colonies were 12.5% in both OM-S and SDP in the 5-day arm.
TTP and bacterial load
Compared to SDP, the median TTP was longer in OM-S-treated MGIT cultures: median (range) TTP 5 (2–12) days versus 9 (1–40) days in the same-day arm (p=0.007) and 7 (1–29) days versus 17 (4–35) days in the 5-day arm (p<0.0001) (figure 1).

Difference in Mycobacterium growth indicator tube (MGIT) times to culture positivity (TTP) for the two groups in each study arm. Bars represent median values. SDP: standard decontamination procedure; SD: same-day arm; OM-S: OMNIgene.SPUTUM procedure; 5D: 5-day arm.
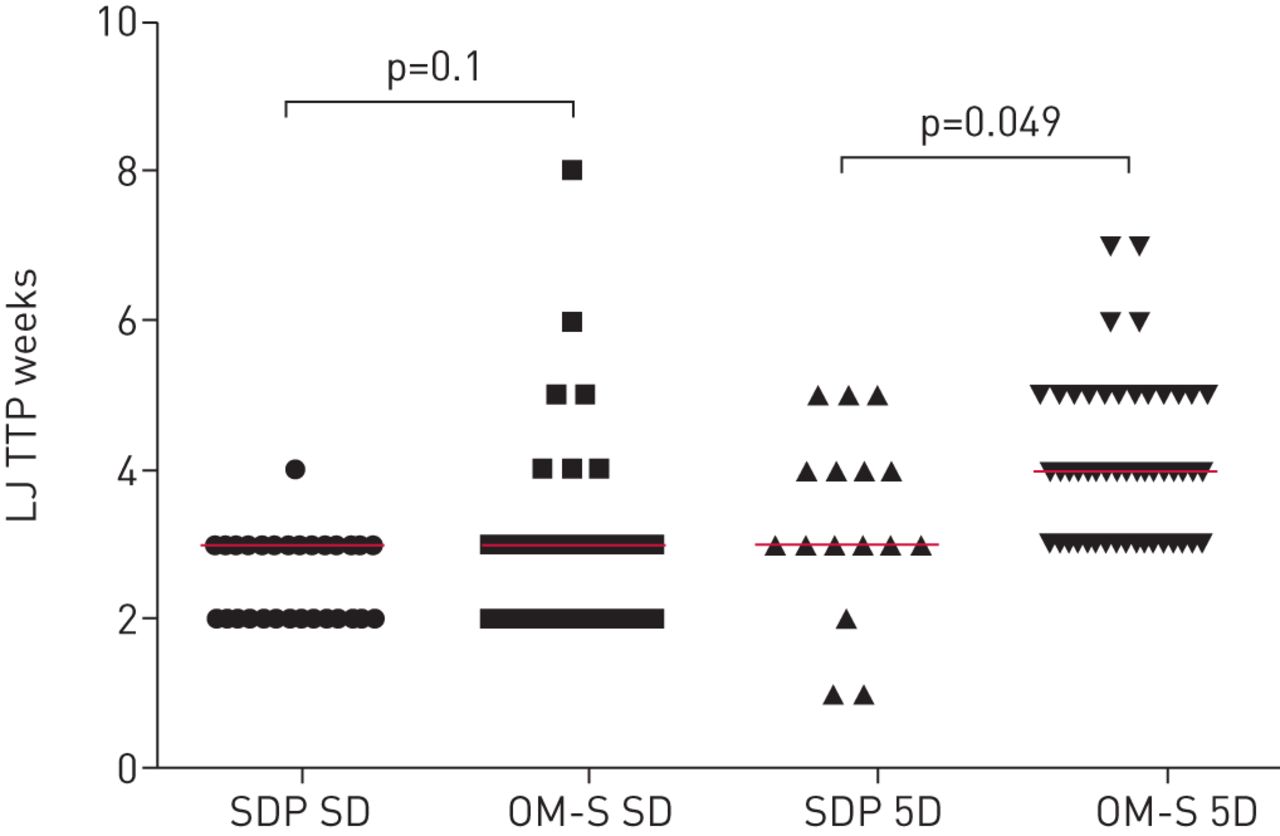
Time to LJ culture positivity of the OM-S-treated sputa (median (range) 3 (2–8) weeks) was not significantly different from the SDP-treated samples (3 (2–4) weeks) in the same-day arm. In contrast, OM-S TTP was 1 week longer (4 (3–7) weeks) than SDP TTP (3 (1–5) weeks) in the 5-day arm; however, the difference was marginally significant (p=0.049) (figure 2).

Difference in Lowenstein Jensen (LJ) times to culture positivity (TTP) for the two groups in each study arm. Bars represent median values. SDP: standard decontamination procedure; SD: same-day arm; 5D: 5-day arm; OM-S: OMNIgene.SPUTUM procedure.
Unlike MGIT TTP, there was no difference in the viable bacterial load count (median (range) 6 (3–8) log10 eCFU·mL−1 and 6 (3–7) log10 eCFU·mL−1 for control and OM-S-treated sputa, respectively, in the same-day arm (p=0.3). In the 5-day arm, OM-S-treated sputa had 1 log lower bacterial load (5 (2–7) log10 eCFU·mL−1) compared to 6 (3–8) log10 eCFU·mL−1 for control samples (p<0.0001) (figure 3).

Differences in viable bacterial load count by molecular bacterial load assay for the two groups in each study arm. Bars represent median values. CRL: control; SD: same-day arm; 5D: 5-day arm; OM-S: OMNIgene.SPUTUM procedure.
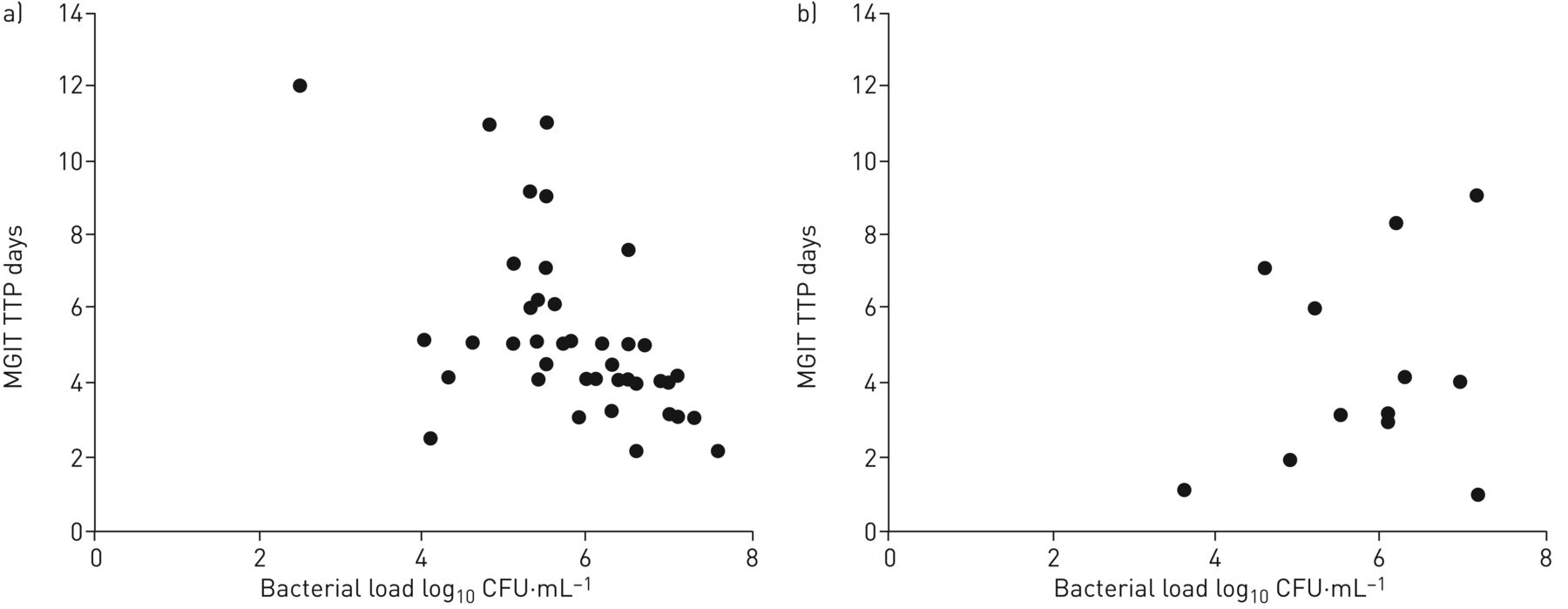
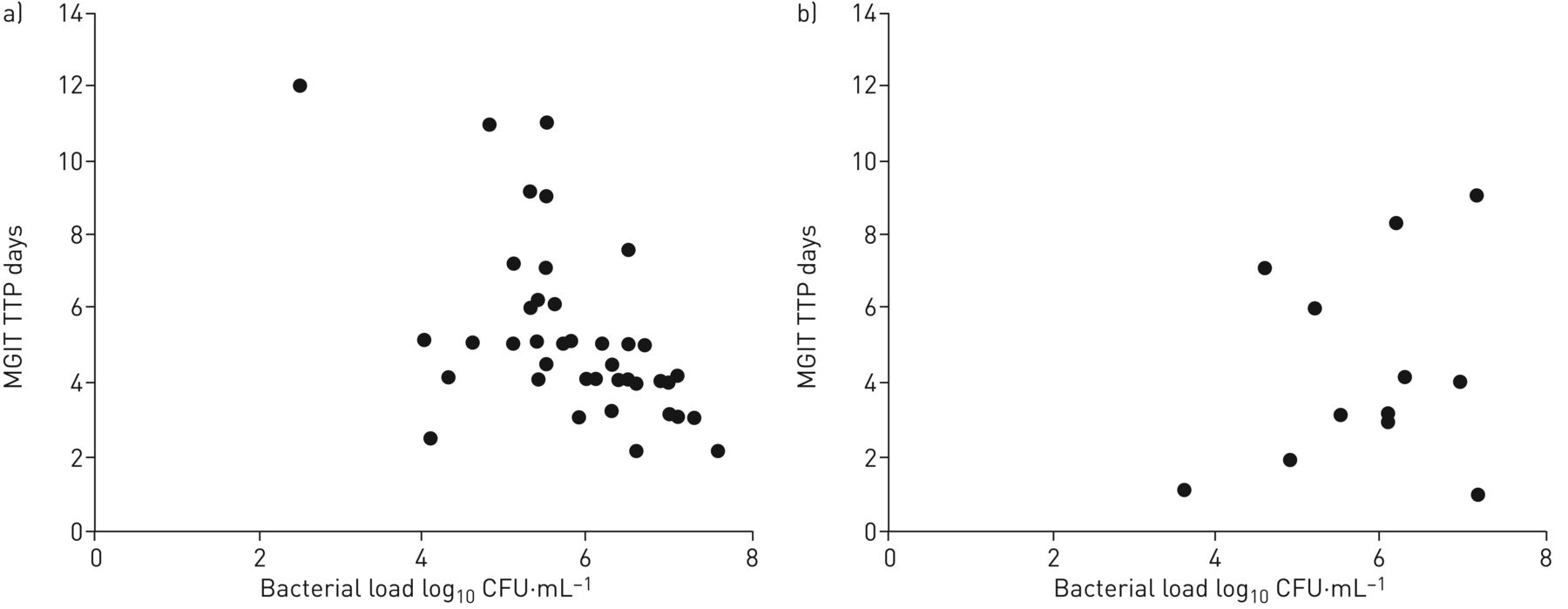
As measures of viability, MGIT TTP and molecular bacterial load are inversely correlated [9, 10]. Given the many MGIT negative results, we explored whether this was due to loss of viability by testing the correlation between SDP/OM-S MGIT TTP and bacterial load measured by MBLA among same-day samples. There was a strong correlation between SDP MGIT TTP and bacterial load (Spearman's r=−0.6, 95% CI −0.8–−0.4; p<0.0001). In contrast, there was no such correlation between MGIT TTP and bacterial load count in the OM-S-treated samples (r=−0.1, 95% CI −0.4–0.5; p=0.8) (figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The correlation between Mycobacterium growth indicator tube (MGIT) time to culture positivity (TTP) and bacterial load count by molecular bacterial load assay for a) standard decontamination procedure-treated samples and b) OMNIgene.SPUTUM-treated samples.
Operational usability
Addition of OM-S at the site of sputum collection took on average 2 min per sample. At the laboratory, sample processing took 20 min including centrifugation to remove the OM-S reagent and inoculation. This translates into 22 min sample processing time for OM-S. SDP took 45 min, including NALC/NaOH preparation, sputum decontamination, neutralisation and centrifugation to inoculation. OM-S-treated samples appeared milky, more fluid and easy to pipette. 500 mL OM-S reagent was used to process 176 samples. At a cost of USD 250 per 250-mL reagent (manufacturer's quoted price), it means each sample cost USD 2.84 compared to USD 0.10 per sample for SDP reagents. Both prices exclude labour and estate costs.
Discussion
The WHO End TB Strategy calls for detection and treatment of every case [17]. Tools that maintain sample quality will be critical in the realisation of this target by assuring the accuracy of tests. To this end we evaluated the novel medium OM-S for short-term and long-term decontamination and preservation of M. tuberculosis viability at ambient temperature. We have shown that OM-S is more effective at suppressing contaminants, supports higher M. tuberculosis recovery from solid LJ culture, and maintains substantial M. tuberculosis viability over a longer period at ambient temperature than the SDP. This makes it an optimal medium for sample transport in places where processing laboratories are far away from centres of sample collection and cold-chain transport is unrealistic. In addition, we have shown that OM-S-treated MGIT samples had longer TTP: 4 and 10 days longer in same-day and 5-day samples, respectively. The effective suppression of contaminants and the longer TTP concur with previous evaluation studies of OM-S [8, 15].
The long-term assessment mimics long-distance specimen referral system where samples are likely to take >24 h to reach the processing laboratory. We have shown that over a period of 5 days and temperature range 29–34°C, OM-S maintained a high level of M. tuberculosis viability with loss of only 1 log eCFU·mL−1. This contrasts with the reported 1 log viability loss caused by 15-min treatment of samples with NALC/NaOH [18]. The WHO recommends not more than 20 min NALC/NaOH sample treatment, suggesting that any longer exposure would adversely reduce viable bacilli in the sputum [6]. A recent study has further shown increased TB detection in OM-S-treated sputum by smear microscopy and Xpert MTB/RIF [7].
Importantly, we have shown that in addition to maintaining viability, OM-S is more effective at suppressing contaminants than SDP. The 27% contamination rate observed in the 5-day control sputum demonstrates the overgrowth of contaminating organisms that can occur at high temperature when referred specimens take long in the delivery processes. Our results show that NALC/NaOH is less effective against such high level of contamination. This perhaps explains the unacceptable (>7%) culture contamination reported in tropical settings [19]. Cold-chain transport has always been recommended as preventative measure of contaminant growth but it is expensive to maintain and often impractical if specimens take a week or longer on the way to the processing laboratory. OM-S obviates cold-chain transport by effectively suppressing growth of contaminants while maintaining viability.
Although OM-S was effective at supressing contaminants, it achieved low M. tuberculosis recovery, particularly in MGIT culture. The lower positivity corresponded with higher MGIT culture TTP, both in same-day and 5-day arms. In contrast OM-S treatment produced more positive LJ cultures than SDP with comparable TTP. In addition, the LJ colony densities and MBLA positivity were similar. The viable bacterial load count was similar between OM-S and control in the same-day arm and only 1 log less in the 5-day arm. Taken together, we hypothesise that low percentage positivity is not due to loss of viability, but due to inhibition by leftover reagent that diffused into the MGIT broth following inoculation. In the same vein, we believe that LJ agar absorbs and neutralises the leftover OM-S, leaving bacilli to grow free of the reagent. The absence of correlation between OM-S-treated sample TTP and bacterial load supports our hypothesis. Studies in our group and others have shown that MGIT TTP is inversely correlated with bacterial load [9, 10, 20]. Further studies are needed to optimise OM-S sample processing for MGIT culture to reduce inhibition and shorten TTP.
This 84% OM-S LJ culture positivity compared to 28% of the NALC/NaOH-decontaminated control sputa at 5 days further confirms maintenance of viability. However, we don't know whether effect on sputum M. tuberculosis viability would remain minimal under OM-S beyond 5 days, a question that calls for further investigations beyond 5 days. The caveat on LJ TTP is that it is not as accurate as the automated MGIT. LJ cultures were read on a weekly basis, thus increasing the possibility of colonies appearing before the reading time. So, the LJ culture TTP only gives a rough idea of the time when colonies were visible on the slant, and it could well be that both treatments had similar LJ culture TTP.
In resource-limited settings with processing laboratories far away from specimen collection centres, OM-S provides a practical solution for maintaining sample quality. Even when Mozambique achieves the required capacity of six culture laboratories, samples will need to be transported over a distance of >20 000 km2 and at high ambient temperatures [5]. The situation is not different in many other resource-limited high-burden TB countries [21, 22].
Overall, it takes less time to process sputum using OM-S. The ease of adding OM-S to the sputum means that technicians in microscopy laboratories can add the reagent and send the sample to a central culture laboratory. The USD 2.84 cost of OM-S per reagent demonstrates the potential affordability of OM-S in resource-limited settings. The simplicity of use and transportation at ambient temperature offsets labour time and cold transport costs. Although the NALC/NaOH solution reagents are cheaper, (USD 0.10 per 5 mL sputum), the technician's time cost of preparing solution every day and costs of retreating contaminated samples and the requirement of cold-chain transport offset the advantage of the low cost of reagents. With OM-S treatment, samples can be batched without worry of contamination and loss of viability, and thus increase the management efficiency of high sample volume TB laboratories.
Conclusion
OM-S has demonstrated high potency to suppress contaminants, and has achieved higher positive culture results and maintenance of viability, particularly in LJ cultures of sputa kept for long time at ambient temperatures. Due to low sensitivity and long time to results, the use of LJ cultures in most laboratories is declining, and so the higher positivity caused by OM-S treatment will revitalise the use of these cultures. Operationally, OM-S is more user-friendly, providing advantages such as effective liquefaction and shorter sample processing time. TB detection by culture and time taken to obtain a result is important clinically; thus, further studies to optimise sample processing to achieve higher MGIT culture positivity and shorter time to result are critical. Evaluation of the utility of OM-S on smear-negative sputa is crucial, especially for paucibacillary patients such as children and HIV-positive patients. In addition, the cost-effectiveness of using OM-S should be assessed in detail to provide compelling evidence to policy makers for its adoption in routine practice.
Acknowledgements
The study was made possible by funding from DNA Genotek Inc. Canada and staff: Alexandra Weirich, Pat Curry and Cassandra Kelly–Cirino who supported the study. We acknowledge the Mozambique NTRL technical staff Manuel Gimo, Sheridan Semá, João Manuel, Joaquim Dimande and Leonel Fernando, who were very instrumental in processing the samples. Special thanks to staff at sputum collection sites: Chamanculo and Boane Health Centres and APOPO for collecting samples, and to patients who donated the samples.
Footnotes
Conflict of interest: None declared.
Support statement: The study was funded by DNA Genotek Inc. Canada, the manufacturer of OMNIgene.SPUTUM (grant number SMD0 – Z0B014). The funder did not influence the analysis of data or the choice of where to publish the findings. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received June 20, 2017.
- Accepted December 19, 2017.
- Copyright ©ERS 2018
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










