





Figures
- FIGURE 1
Cohort identification and exclusion. A flow diagram describing the methodology of the study, from patient identification and selection to the development and validation of the echocardiography (echo) score in the derivation (n=210) and validation (n=61) cohorts; the latter derived from the same population over the same time period, but with some missing brain natriuretic peptide (BNP) and pulmonary function testing (PFT) data from the time of right heart catheterisation (RHC). CT: computed tomography; PH: pulmonary hypertension; ILD: interstitial lung disease; HRCT: high-resolution CT.
- FIGURE 2
Severe pulmonary hypertension (PH) in interstitial lung disease (ILD) stepwise composite echocardiographic score. If an overall score of ≥7 is achieved, then the score is positive for the prediction of severe PH with a mean pulmonary arterial pressure (PAP) ≥35 mmHg. Where the right ventricular systolic pressure (RVSP) is >64 mmHg, the score is positive and no further analysis is necessary. Where RVSP is not available or intermediate then each step is continued until either a score of ≥7 is achieved, or if the final score is <7, in which case the score is negative and severe PH is unlikely. NA: not available; RV: right ventricle; LV: left ventricle.
- FIGURE 3
Line plots demonstrating the effect of increasing unavailability of tricuspid regurgitation on the echocardiographic score area under the curve (AUC) for severe pulmonary hypertension (PH) analysis and its effect on sensitivity. Given the frequent “real-life” difficulty assessing tricuspid regurgitant velocity (TRV) at echocardiography in interstitial lung disease (ILD) patients, models were created to demonstrate the effect of increasing unavailability of TRV on a) the AUC of the echocardiographic score and b) the sensitivity of the score in predicting severe PH. We simulated an increasing level of unavailable TRV by randomly blinding available TRV values, with 100 iterations (by bootstrapping), and calculated the AUC and sensitivity following each iteration. We tested levels of TRV unavailability ranging between 8% (observed in the original cohort) and 60% (by 1% increments). The line plots show that AUC for the echo score is preserved across a wide spectrum of TRV unavailability (a). In addition, there was a minor reduction in the sensitivity of the score, despite a dramatic reduction in TRV availability from 93% to 40%, as opposed to TRV alone (using a cut-off of 4 m·s−1, missing values considered ≤4 m·s−1) with a sensitivity that is halved.



{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Threshold values of individual variables within the composite echocardiographic score, and the final score based upon area under the curve (AUC) analysis
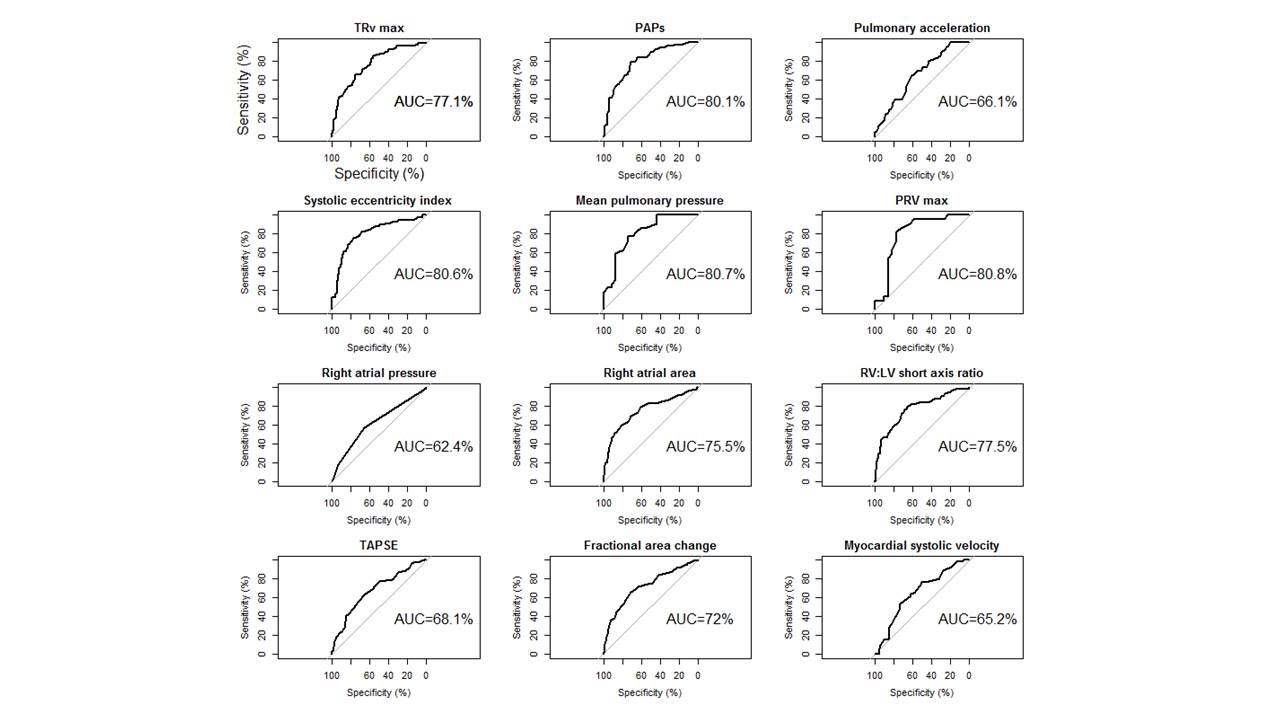
Score Permutations Score Minimum Maximum RV systolic pressure mmHg >64 4 8 5 7 >35 1 5 5 1 ≤35 or NA 0 0 1 0 Right atrial area cm2 >25 3 7 5 6 >20 1 2 4 1 ≤20 or NA 0 0 1 0 Early diastolic pulmonary regurgitation velocity mmHg >36 4 8 5 4 ≥20 1 3 3 3 <20 or NA 0 0 1 0 RV fractional area change % <35 1 5 5 4 ≥35 0 0 1 0 RV/LV short axis dimension >1 1 6 6 3 ≤1 or NA 0 0 0 0 Systolic eccentricity index ≥1.1 1 4 4 1 <1.1 or NA 0 0 1 0 Total permutations n 900 000 Maximum score 25 Each component of the composite score was selected as that having the highest AUC to predict pulmonary hypertension using receiver operating curve analysis (figure 1 and online supplementary material) and consensus. For example, for right ventricular systolic pressure (RVSP), a minimum score of 4 and a maximum of 8 was set; this was done for each threshold and variable, thereby creating a stepwise score. Different combinations of score components (n=900 000) were then tested, and the model with the best AUC chosen, which is displayed as the best score. The order of analysis using the echo composite score is shown in the third column. For example, if a score of 7 was achieved at the first step (if RVSP >64 mmHg), then the echo score became positive to predict severe PH, and no further analysis was needed. If the RVSP was <64 mmHg, the second factor, right atrial area, was considered, and so on. RV: right ventricular; NA: not available; LV: left ventricular.
- TABLE 2
Baseline right heart catheter and noninvasive variables
Total derivation cohort mPAP <25 mmHg mPAP 25–34 mmHg mPAP ≥35 mmHg p-value Subjects 210 46 79 85 Age years 61±11 63±11 64±11 58±12 0.004 Male % 55 52 54 56 0.9 ILD diagnosis CTD 59 (28) 15 (25) 21 (36) 23 (39) 0.7 Sarcoidosis 43 (20) 4 (9) 14 (33) 25 (58) 0.01 IPF 62 (29) 18 (29) 28 (45) 16 (26) 0.02 CHP 16 (8) 6 (38) 2 (12) 8 (50) 0.1 NSIP 16 (8) 2 (12) 8 (50) 6 (38) 0.5 Other ILD 14 (7) 1 (7) 6 (43) 7 (50) 0.4 Right heart catheter mPAP mmHg 33±11 20±4 29±3 43±7 <0.001 PVR Wood units 6.0±3.6 2.6±1.5 4.6±1.8 8.8±3.8 <0.001 Cardiac output L·min−1·m−2 4.3±1.3 4.8±1.3 4.1±1.3 4.1±1.2 0.02 PCWP mmHg 10±5 8±5 10±5 11±5 0.008 BNP ng·L−1 102 (44–266) 48 (30–72) 90 (42–141) 241 (105–436) <0.001 Pulmonary function tests FEV1 L 1.6±0.6 1.6±0.6 1.5±0.5 1.6±0.6 0.9 FEV1 % pred 58±18 62±21 57±17 57±17 0.2 FVC L 2.0±0.8 2.0±0.8 1.9±0.7 2.2±0.9 0.2 FVC % pred 60±20 61±22 59 ±18 62±22 0.7 TLCO % pred 25±10 28±10 25±9 24 ±10 0.04 KCO % pred 52±17 59±18 54±16 48±16 <0.001 PaO2 kPa 7.9±1.9 8.9±1.9 8.1±1.9 7.1±1.7 <0.001 CT scan ILD extent <20%/>20% 14/86 15/85 19/81 9/91 0.2 Data are presented as n, mean±sd, n (%) or median (interquartile range), unless otherwise stated. mPAP: mean pulmonary pressure at right heart catheterisation; ILD: interstitial lung disease; CTD: connective tissue disease; IPF idiopathic pulmonary fibrosis; CHP: chronic hypersensitivity pneumonitis; NSIP: nonspecific interstitial pneumonia; PVR: pulmonary vascular resistance; PCWP: pulmonary capillary wedge pressure; BNP: brain natriuretic peptide; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; TLCO: transfer factor of the lung for carbon monoxide; KCO: transfer coefficient of the lung for carbon monoxide; PaO2 : arterial oxygen tension (by capillary blood gas analysis); CT: computed tomography.
- TABLE 3
Echocardiographic variables grouped according to severity of pulmonary hypertension at right heart catheterisation (RHC)
Availability % Derivation cohort, total mPAP <25 mmHg mPAP 25–34 mmHg mPAP ≥35 mmHg p-value Subjects 228 46 79 85 TRVmax m·s−1 92 3.7±0.6 3.3±0.5 3.6±0.5 4.0±0.6 <0.001 RVSP mmHg 92 66±19 53±13 61±18 76±17 <0.001 Pulmonary acceleration time ms 93 77±18 82±17 80±19 70±14 <0.001 Systolic eccentricity index 82 1.4±0.4 1.1±0.2 1.2±0.3 1.6±0.5 <0.001 Early PRVmax m·s−1 20 2.5±0.5 2.0±0.3 2.3±0.5 2.7±0.4 0.001 RAP mmHg 99.5 5 (5–10) 5 (5–10) 5 (5–10) 10 (5–10) 0.008 Fractional area change % 93 37±8 41±8 39±7 34±8 <0.001 Right atrial area cm2 93 20±8 15±4 18±6 24±8 <0.001 TAPSE cm 92 1.8±0.5 1.9±0.4 1.9±0.5 1.7±0.4 <0.001 RV:LV short axis dimension ratio (systolic) 81 0.9 (0.7–1.4) 0.7 (0.6–0.9) 1.0 (0.6–1.1) 1.3 (0.9–2.0) <0.001 Data are presented as n, mean±sd or median (interquartile range), unless otherwise stated. mPAP: mean pulmonary pressure at RHC; TRVmax: maximum tricuspid regurgitation velocity; RVSP: right ventricular systolic pressure; PRVmax: maximum diastolic pulmonary regurgitation velocity; RAP: right atrial pressure; TAPSE: tricuspid annular plane systolic excursion; RV: right ventricular; LV: left ventricular.
- TABLE 4
Comparison of the derivation and validation cohorts
Derivation cohort Validation cohort p-value Subjects 210 61 Age years 61±11 61±13 0.9 Male % 55 39 0.03 ILD diagnosis CTD 59 (28) 33 (54) <0.001 Sarcoidosis 43 (20) 6 (10) 0.06 IPF 62 (29) 5 (8) 0.007 CHP 16 (8) 6 (10) 0.5 NSIP 16 (8) 6 (10) 0.5 Other ILD 14 (7) 5 (8) 0.7 RHC mPAP mmHg 33±11 33±12 0.8 PVR Wood units 6.0±3.6 6.9±5.6 0.3 Cardiac output L·min-1 4.3±1.3 4.1±1.4 0.6 PCWP mmHg 10±5 10±5 0.9 BNP ng·L−1 102 (44–266) 103 (42–306) 0.7 Pulmonary function tests FEV1 L 1.6±0.6 1.6±0.8 0.5 FEV1 % pred 58±18 62±21 0.3 FVC L 2.0±0.8 2.0±0.9 0.7 FVC % pred 60±20 65±22 0.2 TLCO % pred 25±10 27±10 0.2 KCO % pred 52±17 54±17 0.7 PaO2 kPa 7.9±1.9 8.5±2.1 0.1 CT scan ILD extent# 20%/>20% 14/86 19/81 0.5 Data are presented as n, mean±sd or median (interquartile range), unless otherwise stated. ILD: interstital lung disease; CTD: connective tissue disease; IPF idiopathic pulmonary fibrosis; CHP: chronic hypersensitivity pneumonitis; NSIP: nonspecific interstitial pneumonia; RHC: right heart catheterisation; mPAP: mean pulmonary pressure; PVR: pulmonary vascular resistance; PCWP: pulmonary capillary wedge pressure; BNP: brain natriuretic peptide; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; TLCO: transfer factor of the lung for carbon monoxide; KCO: transfer coefficient of the lung for carbon monoxide; PaO2: arterial oxygen tension (by capillary blood gas analysis); CT: computed tomography. #: formal scoring of severity on CT (see methods section).
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00124-2017_supp
Figure S1 00124-2017_figureS1
Figure S2 00124-2017_figureS2
{kind=link}
{kind=link}










