





Abstract
We tested the hypothesis that dynamic hyperinflation develops in severe asthmatic subjects during exercise. Changes in inspiratory capacity (IC) were measured during the 6-min walk test (6MWT) in severe asthmatic subjects compared with chronic obstructive pulmonary disease (COPD) subjects with a similar degree of bronchial obstruction. We assessed whether changes in IC were associated with changes in dyspnoea perception.
27 severe asthmatic subjects (10 males and 17 females) and 43 COPD subjects (35 males and eight females) were recruited. The two groups performed similarly in the 6MWT (p=0.90). At the end of the test, the Borg score increased significantly in both groups (mean difference: for asthmatic subjects 1.7±1.6; p<0.0001; for COPD subjects 3.1±1.9; p<0.0001). IC measured at the beginning of 6MWT was not different between groups (2.25±0.47 L in asthmatic subjects versus 2.38±0.60 L in COPD subjects; p=0.32) and decreased in both groups (mean difference: for asthmatic subjects 0.160 L; p=0.02; for COPD subjects 0.164 L; p<0.0001). However, changes in IC were significantly associated with changes in the Borg score in the COPD group (r2=0.17; p=0.006), but not in the asthma group (r2=0.06; p=0.20).
In severe asthmatic subjects, IC significantly drops during the 6MWT to the same extent as COPD subjects with a similar degree of lung impairment, indicating the development of dynamic hyperinflation. Contrary to COPD, in asthmatic subjects the occurrence of dynamic hyperinflation was not associated with changes in dyspnoea perception.
Abstract
Severe asthma is characterised by occurrence of dynamic hyperinflation during exercise; inspiratory capacity drops in severe asthmatic subjects during the 6MWT to the same extent as in COPD subjects with similar lung impairment http://ow.ly/InfQ30jjivW
Introduction
Asthma is a common disease worldwide, impacting on daily activities and quality of life, especially in its most severe forms [1, 2]. Indeed, dyspnoea on exertion is the most cited and troublesome symptom described by uncontrolled asthmatic patients, mainly for inspiratory effort and not rarely for the occurrence of dynamic hyperinflation [3, 4]. Dynamic hyperinflation is considered the underlying mechanism of exertional dyspnoea in subjects with chronic obstructive pulmonary disease (COPD) and the main cause of disability in these patients. O'Donnell [5] demonstrated that the occurrence of dynamic hyperinflation during exercise in COPD strongly correlates with dyspnoea perception. Although dynamic hyperinflation is recognised as a key determinant of exercise limitation in COPD, little is known about this in other respiratory chronic conditions, such as bronchial asthma [6]. In COPD, the end-expiratory lung volume increases because of airflow limitation, usually due to the increase of ventilation during exercise, and it is expressed as a decrease in inspiratory capacity (IC). Therefore, changes in IC can be regarded as a useful marker of dynamic hyperinflation under experimental conditions that resemble those of daily life. It is plausible to speculate that, in asthma, the state of chronic airway inflammation could lead to oedema and airway smooth muscle contraction that, in turn, are responsible for the small airway collapse and airflow limitation leading to dynamic hyperinflation. Moreover, dynamic hyperinflation can also exert pro-inflammatory effects, mainly through a cellular stretch that acts as a potent inflammatory stimulus [7]. In a study conducted on 22 mild to moderate asthmatic subjects, Laveneziana et al. [8] recorded the occurrence of dynamic hyperinflation during a short cardiopulmonary exercise test in a subgroup of subjects. Satake et al. [9] found that IC decreased after the 6-min walk test (6MWT) in 23 stable COPD subjects and negatively correlated with dyspnoea.
We speculate that the most severe forms of asthma may be characterised by the occurrence of dynamic hyperinflation during exercise. To this aim, we assessed changes in IC during the 6MWT in severe asthmatic subjects and established whether these changes are associated with dyspnoea. COPD subjects, matched for degree of bronchial obstruction, served as a control group.
Methods
This was a case–control study carried out at the Respiratory Units of the University of Palermo (Palermo, Italy) and the San Paolo Hospital, University of Milan (Milan, Italy). Local ethics committees approved the study and written consent was obtained from each participant.
Study population
We enrolled two groups of subjects: 1) consecutive outpatients suffering from severe asthma, according to the European Respiratory Society (ERS) statement [1], and 2) consecutive patients with COPD diagnosis according to American Thoracic Society (ATS)/ERS guidelines [10] (i.e. post-bronchodilator forced expiratory volume in 1 s (FEV1)/forced vital capacity below the lower limit of normal) attending scheduled follow-up consultation with FEV1 >50% of predicted, matched for the same degree of bronchial obstruction. Exclusion criteria were: relevant contraindications to clinical exercise testing, exacerbations within the last 4 weeks, comorbidities that could affect exercise capacity, treatment with β-blockers and inability to perform the study protocol.
Study design
All subjects underwent careful medical history evaluation and symptoms assessment. Asthma control was established by the Asthma Control Test (ACT), which was self-administered. The ACT is a validated five-item instrument, each item rated on a five-point scale, providing a total score that allows discrimination between “well-controlled” (total score 25), “partially controlled” (total score 20– <25) and “not controlled” (total score <20). The questions address symptoms occurring within the 4 weeks preceding the evaluation. The frequency of exacerbations in the previous year was also recorded.
Dyspnoea was measured using the Italian version of the modified Medical Research Council dyspnoea scale. Then, patients performed forced and slow vital capacity manoeuvres in accordance with ATS/ERS guidelines [11, 12]. The 6MWT was performed along a flat, straight, 30-m walking course supervised by a well-trained researcher according to ATS guidelines [13], using a portable spirometer (Spiropalm; COSMED, Rome, Italy) with integrated pulse oximeter and ventilation measurement, which allows the measurement of IC at the beginning (at resting conditions) and immediately after the end of the test [14]. Exercise breathlessness was graded using the Borg scale [15]. Dynamic hyperinflation was defined as a decrease of >150 mL in IC at the end of exercise compared with resting levels [16].
Statistical analysis
The results are expressed as mean and standard deviation, unless otherwise stated. This was a pilot study. In view of the lack of previous experiences, no formal sample size calculation was made. Before data analysis, Lilliefors corrected Kolmogorov–Smirnov test was performed to examine the distribution of the residuals of the parametric tests. Quantitative variables were analysed using the t-test or Mann–Whitney test as appropriate. All tests were two-sided and p-values <0.05 were considered statistically significant. Statistical tests were performed using SPSS version 21.0 (IBM, Armonk, NY, USA).
Results
27 patients with severe asthma (10 males and 17 females) and 43 individuals affected by COPD (35 males and eight females) were recruited while in stable condition. All study subjects were under optimal inhaled treatment according to the stage of the disease, which was not stopped on the day of the study. All asthmatic subjects were under high-dose inhaled corticosteroids plus long-acting β2-adrenergics. COPD subjects were taking long-acting β2-adrenergics and/or long-acting muscarinic antagonists, together with inhaled corticosteroids according to the severity of their disease. None of the study subjects was under systemic corticosteroid treatment or biological drugs at the time of enrolment. No significant comorbid conditions potentially affecting the outcomes of the study (i.e. cognitive impairment, nonrespiratory mobility difficulties, heart failure) were documented. Asthmatic subjects were significantly younger than COPD subjects (57±11 versus 66±10 years, respectively; p=0.002). Body mass index did not differ between the two groups (28.6±5.0 versus 27.2±4.1 kg·m−2, respectively; p=0.19). Among asthmatic subjects, 18 subjects had never smoked, two were current smokers and seven were ex-smokers; conversely, among COPD subjects, only one had never smoked, 23 were current smokers and 19 were ex-smokers. Lung function characteristics are depicted in table 1. By design, the degree of airway obstruction was similar between groups. For asthmatic subjects, the mean ACT score was 16±3 and the rate of exacerbations in the previous year was 1.2±0.6. In COPD subjects, the rate of exacerbations was 2.2±0.8.
Baseline lung functional characteristics of the study subjects
The two groups did not differ in terms of metres walked in the 6MWT (asthmatic subjects versus COPD subjects: 392±71 versus 389±97 m; p=0.90). Heart rate at the beginning of the test was 84±14 beats·min−1 in the asthmatic subjects and 66±43 beats·min−1 in the COPD subjects (p=0.03). In both groups, the heart rate reached a peak value during the test that was significantly higher than baseline (mean difference: for asthmatic subjects 25±18 beats·min−1; p<0.0001; for COPD subjects 22±19 beats·min−1; p<0.0001). Minute ventilation at the beginning of the 6MWT was 13.5±7.3 L·min−1 in asthmatic subjects and 4.3±6.7 L·min−1 in COPD subjects, and reached a significantly higher peak value in both groups (mean difference: for asthmatic subjects 18 L·min−1; p<0.0001; for COPD subjects 23 L·min−1; p<0.0001). Percutaneous oxygen saturation at the beginning of the test was 95±2% in asthmatic subjects and 96±3% in COPD subjects (p=0.26), and remained unchanged at the end of the test in the asthmatic subjects (mean difference 0.26%; p=0.56), whereas it dropped significantly in the COPD subjects (mean difference 2.0%; p<0.0001). The Borg score was significantly different between the two groups prior to the procedure (asthmatic subjects versus COPD subjects: 1.1±1.3 versus 0.3±0.8; p=0.002). At the end of the test, the Borg score increased significantly in both groups (mean difference: for asthmatic subjects 1.7±1.6; p<0.0001; for COPD subjects 3.1±1.9; p<0.0001).
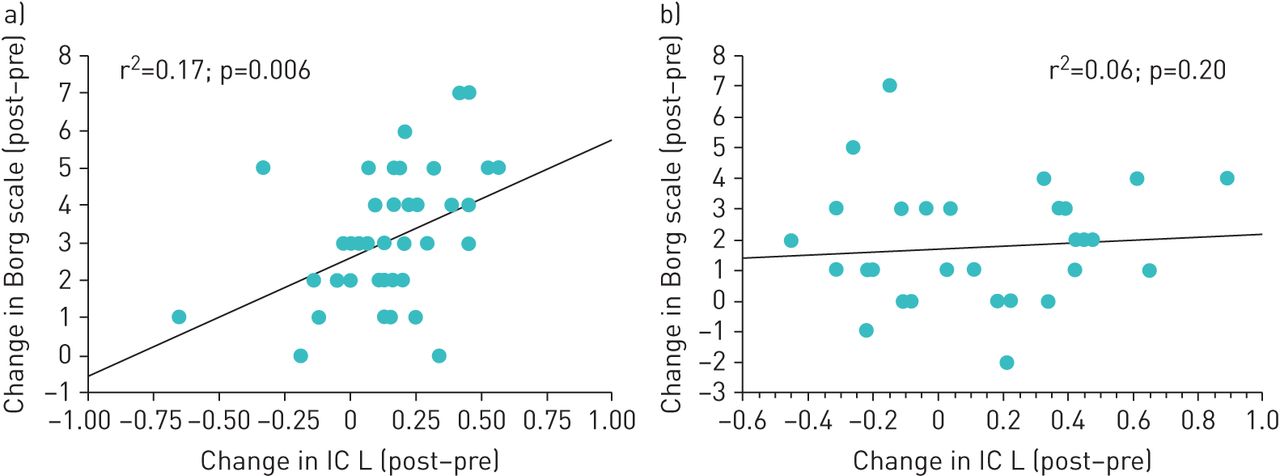
The IC measured at the beginning of the 6MWT was not different between groups (2.25±0.47 L in asthmatic subjects versus 2.38±0.60 L in COPD subjects; p=0.32). During the test, IC significantly decreased in both groups by the same extent (mean difference: for asthmatic subjects 0.160 L; p=0.02; for COPD subjects 0.164 L; p<0.0001) (figure 1). Interestingly, changes in IC were significantly associated with changes in the Borg score in the COPD group (r2=0.17; p=0.006), but not in the asthmatic group (r2=0.06; p=0.20) (figure 2a and b). The changes in IC during the 6MWT were not predicted by the degree of airway obstruction (FEV1 % pred) in either group (p>0.05).

Changes in inspiratory capacity (IC) during the 6-min walk test. COPD: chronic obstructive pulmonary disease. p<0.0001 for both groups.

{kind=link}
{kind=link}
Association between changes in inspiratory capacity (IC) during the 6-min walk test and changes in the Borg scale: a) chronic obstructive pulmonary disease group and b) asthmatic group.
Discussion
The current study was designed to test the hypothesis that the most severe forms of asthma are characterised by the occurrence of dynamic hyperinflation during exercise. By using a portable system, we found that during the 6MWT IC significantly decreased in severe asthmatic subjects and this reduction did not differ from that observed in COPD subjects with a similar magnitude of airway obstruction. The lack of association between changes in IC and in dyspnoea perception in severe asthmatic subjects as opposed to COPD subjects suggests that in the former exertional dyspnoea has multiple determinants.
Tidal expiratory flow limitation (EFL) is a pathophysiological feature of COPD, and arises because of the dual effects of permanent parenchymal destruction and airway obstruction [17]. In COPD patients, the increased compliance of the lung leads to a resetting of the respiratory system's relaxation volume to a higher level than in age-matched healthy individuals and this phenomenon is termed static lung hyperinflation. The EFL occurs in a significant proportion of patients with COPD during resting breathing and in almost all COPD patients during exercise [18], resulting in dynamic hyperinflation that is reflected in decreased IC and associated with impaired exercise performance [18–20]. O'Donnell et al. [16] examined dynamic hyperinflation during exercise in COPD and healthy age-matched controls, and concluded that inability to expand tidal volume in response to increasing metabolic demand contributed importantly to exercise intolerance in COPD. Marin et al. [21] tested the hypothesis that dyspnoea during the 6MWT could be associated with the development of dynamic hyperinflation. As most clinicians evaluate their patients with questions that relate breathlessness to activities of daily living such as walking, the 6MWT has become a popular, reliable and safe alternative to the more formal cardiopulmonary exercise test [22], and correlates with treadmill exercise [23]. Marin et al. [21] measured IC at rest and after a 6MWT in 72 males with COPD, showing that simple walking results in dynamic hyperinflation that can be easily determined using IC and that the increased perception of dyspnoea during walking correlates with the degree of dynamic hyperinflation. These findings were confirmed in a recent study by Satake et al. [9] performed in 23 subjects with stable COPD and replicated in our COPD group. Interestingly, Ofir et al. [24] showed that dynamic hyperinflation also develops during exercise tests in symptomatic patients with mild COPD and relatively preserved lung function, together with dyspnoea increase and exercise curtailment.
The current finding of the occurrence of dynamic hyperinflation during exercise in severe asthmatic subjects is novel and could contribute to explain exertional dyspnoea in this population. A clear relationship between activity limitation and quality of life has been demonstrated in asthmatic subjects. Uncontrolled asthma is associated with a two-fold risk of limitation of physical activity with a negative impact on work and regular activities [3, 4]. Several mechanisms are responsible for activity limitation in asthma, such as peripheral and respiratory muscle impairments and the negative impact of systemic corticosteroids [6]. Respiratory function, exercise capacity (6MWT distance, incremental cycloergometry and inspiratory threshold loading) and dyspnoea were assessed in seven patients with a history of near-fatal asthma and eight non-near-fatal asthma patients [25]. Although exercise tolerance was similarly reduced in both the near-fatal asthma and non-near-fatal asthma groups, dyspnoea at peak cycle exercise was significantly lower in the former who mainly stopped because of leg discomfort. A similar trend was observed in the 6MWT and inspiratory threshold loading test. However, few data are available with regard to EFL and dynamic hyperinflation during exercise. In their study, Barreiro et al. [25] found that patients with a history of near-fatal asthma had a significant decrease in IC during cardiopulmonary exercise testing (CPET). Dynamic hyperinflation is known to induce an intrinsic positive end-expiratory alveolar pressure, acting as a threshold inspiratory load and causing the tidal volume to set in a stiffer portion of the volume–pressure curve, thus increasing the elastic load, and leading to increased mechanical impedance of the respiratory system on inspiratory muscles that are functionally weaker, mainly because of an unfavourable position on their length–tension curve [26, 27]. It has been demonstrated that stable asthmatic patients seldom exhibit EFL during resting breathing [28, 29], unless under severe and prolonged bronchoconstriction [30]. Laveneziana et al. [8] assessed IC and the perception of dyspnoea in 22 stable asthmatic patients during short CPET and methacholine inhalation. Airway obstruction and hyperinflation were the best predictors of dyspnoea during methacholine challenge, whereas work rate, minute ventilation and tidal volume were the best predictors of dyspnoea in subjects undergoing CPET.
Our findings show that the Borg score at rest was significantly higher in COPD subjects than in asthmatic subjects, although matched for airway obstruction, as already found in previous studies [31–33]. In addition, similar to previous studies [31–33], changes in the Borg score during exercise were relatively low in the asthmatic populations. It was hypothesised that this may be related to the fact that the highest score on the Borg scale is anchored to the most severe breathlessness that patients had ever experienced [33]. Thus, since, unlike other patients, most asthmatic subjects experience severe breathlessness only during acute episodes of bronchoconstriction, they may perceive a relatively low sensation of dyspnoea during exercise. Interestingly, our investigation failed to find a significant relationship between changes in IC and in Borg scores, as opposed to COPD. This challenges our hypothesis of dynamic hyperinflation being the most relevant determinant of exertional dyspnoea in asthmatic subjects and suggests that other mechanisms, such as a mismatch between central drive and respiratory movements or different qualitative sensations of dyspnoea, could be implicated to explain the occurrence of dyspnoea during exercise.
The mechanisms leading to airflow limitation and dynamic hyperinflation in asthma may differ from the well-known pathogenetic factors that are implicated in COPD. Agusti et al. [7] speculated about the potential relationships between dynamic hyperinflation and airway inflammation. Inflammation contributes to the pathogenesis of dynamic hyperinflation through the oedema and increased airway resistance, increased mucus production and alveolar destruction. It is plausible to speculate that inflammation at the level of peripheral airways in asthma is responsible for the occurrence of EFL and dynamic hyperinflation. In this respect, a body of evidence has accumulated to confirm that small airways are the major site of inflammation in severe asthmatic subjects [34, 35], and features of air trapping and lung hyperinflation characterise the most severe forms of asthma [36–39]. The observation of loss of alveolar attachments in fatal asthma [40], as well as loss of elastic recoil and reduced diffusing capacity in severe asthmatic subjects [41], could imply the involvement of the parenchymal component of the lung, which deserves to be investigated in specifically designed studies. Of note, dynamic hyperinflation could contribute to inflammation, thus perpetuating the functional abnormalities; dynamic hyperinflation has been shown to promote pro-inflammatory effects through several mechanisms: cellular stretching, tissue damage and danger signals, and hyperventilation and hypoxia.
The study has some limitations. First, as the study was not designed to explore the mechanisms of dyspnoea on exertion in asthmatic subjects, the explanations provided are only speculative and not persuasive. Second, it is possible that some patients in both groups were not stressed enough during the walking test to induce severe dyspnoea (<2-unit increase in Borg ratings during the 6MWT), thus potentially limiting the results. If any, however, we would expect dynamic hyperinflation to occur earlier and to correlate with changes in dyspnoea with more intensive exercise. Third, little is known on the individual level about daily activities and conditioning, which could have potentially affected the differences between groups. Finally, enrolled asthmatic patients were significantly younger than those with COPD, with fewer comorbidities. This aspect could theoretically affect the occurrence of dynamic hyperinflation, which has been demonstrated in other conditions such as chronic heart failure. However, patients with comorbidities that could affect exercise capacity had been excluded, thus reasonably ruling out this bias.
In conclusion, the current study showed that severe asthmatic subjects develop dynamic hyperinflation during exercise to the same magnitude as COPD subjects. This phenomenon could add some insight into the mechanism of daily exercise limitations in this population. Further studies are needed to explore the determinants of exertional dyspnoea in severe asthmatic subjects.
Footnotes
Author contributions: A. Benfante participated in the design of the study, recruited the patients, performed the study tests, collected and analysed the data, and contributed to the writing of the manuscript. F. Di Marco participated in the design of the study, analysed the data, and participated in the interpretation of the results and the writing of the manuscript. S. Terraneo recruited the patients, performed the study tests, and collected and analysed the data. S. Centanni contributed to the interpretation of the results and to the writing of the manuscript. N. Scichilone conceived and designed the study, recruited the patients, participated in the analysis of the data, and wrote the first version of the manuscript. He is the guarantor of the paper.
Conflict of interest: None declared.
Support statement: The University of Palermo and University of Milan supported the study. The investigation had no external funding from other agencies. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received November 9, 2017.
- Accepted March 28, 2018.
- Copyright ©ERS 2018
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










