





Abstract
Pleural transudative effusion arises from imbalances between the hydrostatic and/or oncotic pressures. Temperature drop following talc poudrage through a spray may accentuate the pressure changes induced by superior vena cava syndrome. http://ow.ly/EpZm30nwVZj
To the Editor:
Pathophysiology, diagnosis and treatment of pleural transudates has widely been described in the literature [1–3]. Except for left heart failure, which requires diuretics, thoracoscopic talc pleurodesis appears to be a safe and effective therapeutic option [4–6]. We report the case of a woman who presented with a sudden pleural fluid formation from her parietal pleura during a talc pleurodesis for a recurrent transudative pleural effusion. We discuss the pathophysiology of this phenomenon.
A 71-year-old woman presented with left pleural effusion. She had a history of Hodgkin lymphoma treated in 1987 with chemotherapy (ABVD regimen: adriamycin, bleomycin, vinblastine and dacarbazine) and extended-field radiation therapy (mantle: 40 Gy; para-aortic and splenic: 30 Gy) leading to a restrictive ventilatory defect (total lung capacity 58.8% of predicted). In 2010, she presented with multifactorial polycythaemia that was managed through phlebotomy. Due to poor peripheral vein conditions, a port catheter was placed to optimise treatment. In 2011, she developed a bilateral pleural effusion with left predominance. Clinical examination revealed erythema, laterocervical oedema and collateral venous circulation of the chest. Vascular imaging revealed a complete superior vena cava (SVC) thrombosis extended to the left subclavicular vein leading to the ablation of the port catheter and to an anticoagulation therapy (tinzaparin followed by acenocoumarol). Despite this management, a moderate left pleural effusion persisted, and a new vascular imaging revealed a 4-cm-long remaining thrombosis of the SVC (below the junction of the arch of the azygos vein), and a congenital anastomosis between a left intercostal vein and the left upper pulmonary vein. In June 2016, bilateral pleural effusion occurred due to congestive heart failure following a myocardial infarction. The evolution was initially good under diuretic therapy (furosemide 40 mg·day−1), with a complete regression of the right-sided pleural effusion but only a partial regression of the left-sided one, which progressively increased during follow-up. In this patient treated with diuretics, thoracentesis revealed a protein pleural fluid concentration of 37 g·L−1 while the pleural/serum ratios for proteins and lactate dehydrogenase were 0.51 and 0.5, respectively. The serum/effusion gradient was 12.9 g·L−1 for albumin and 35 g·L−1 for protein. Altogether, these results were consistent with a true transudate. Considering the symptomatic recurrence of this left-sided effusion, a thoracoscopic talc pleurodesis was decided. During talc poudrage (6 g Steritalc spray; Novatech, La Ciotat, France), immediate emergence of droplets was observed exclusively from the parietal pleura (figure 1). Follow-up of the patient revealed no recurrence of pleural effusion.
{kind=link}
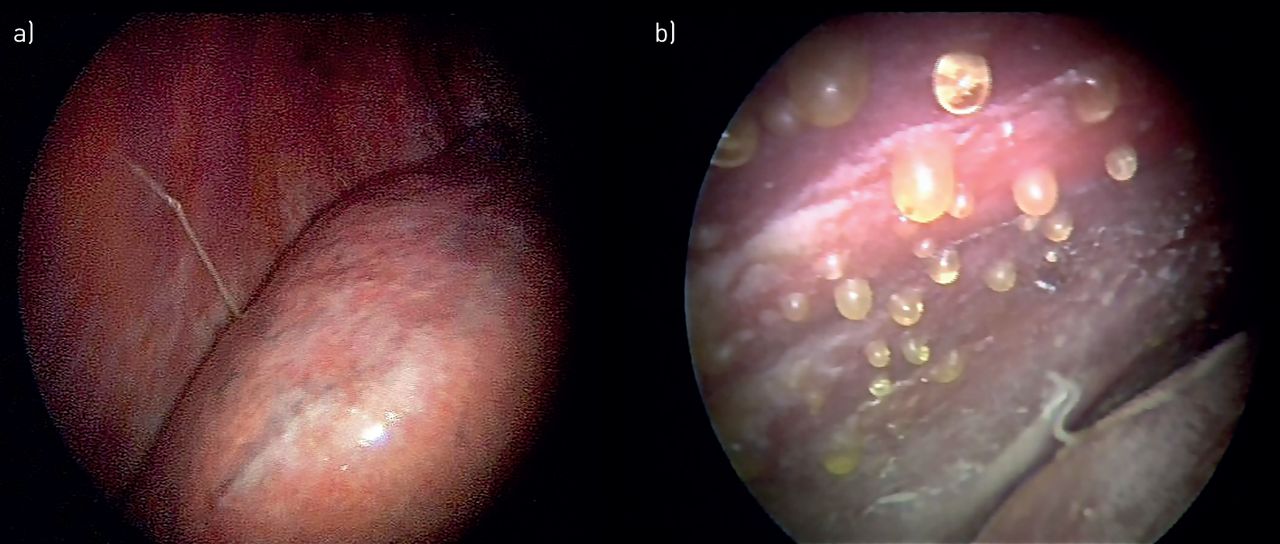
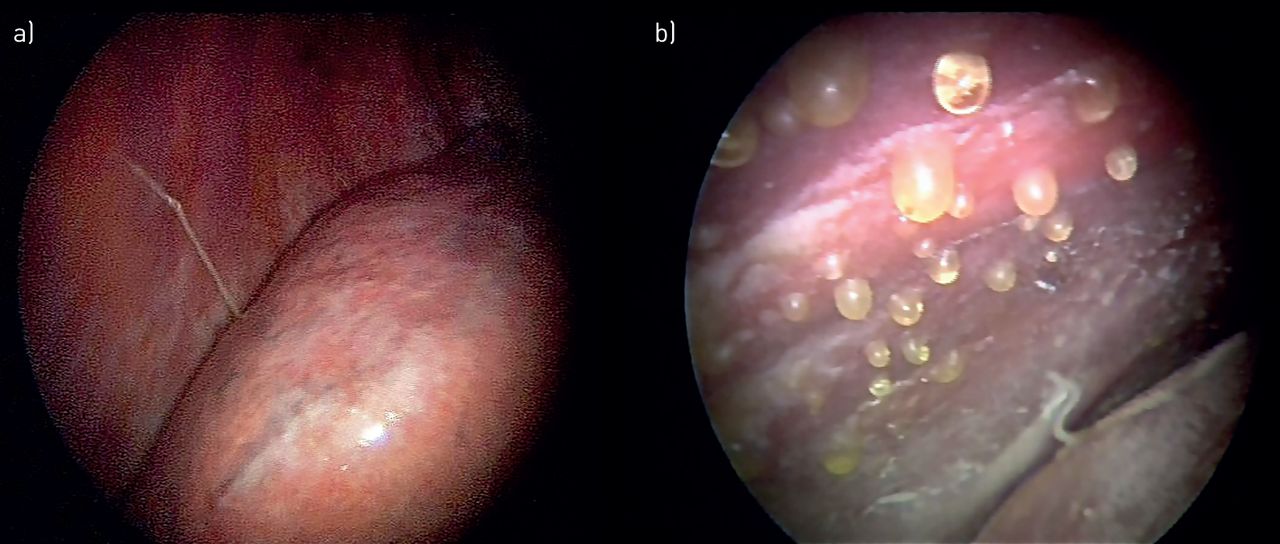
a) Thoracoscopic view of the left pleural cavity before talc pleurodesis. b) Same view following talc poudrage with Steritalc spray (Novatech, La Ciotat, France): an immediate sweating of pleural fluid droplets from the parietal pleura can be observed.
According to Starling's equation, pleural fluid formation is regulated by the balance of hydrostatic and osmotic pressures. The role of parietal pleura is thought to be more important than the visceral pleural for fluid production according to the different anatomies of the two pleural membranes [7–9]. Indeed, the parietal pleura receive their blood supply from systemic capillaries (mainly through intercostal arteries) with a high-pressure regimen and its venous drainage relies primarily on intercostal veins, which drain into the azygos vein (for the right-sided pleura) and into the hemiazygos veins (left-sided pleura). Conversely, blood supply to the visceral pleura originates from both bronchial and pulmonary artery (low-pressure regimen), and its venous drainage is provided by pulmonary veins flowing into the left atrium. Considering these differences, the driving pressure determining the movements of liquid from pleura into the pleural space has been estimated to 14 cmH2O for the parietal pleura versus 9 cmH2O for the visceral pleura [7]. Another argument for a predominant fluid formation from the parietal pleura is that the parietal pleural microvessels are closer to the pleural space (10–12 µm) than are those of the visceral pleura (20–50 µm) [7, 8]. Finally, pleural liquid absorption is mainly provided by interstitial lymphatics through the stomata of the parietal pleura [7–9]. Excessive accumulation of pleural fluid develops when the rate of fluid formation exceeds its drainage capacity. Transudates arise from imbalances between the hydrostatic and/or oncotic pressures, which result in increased fluid production.
In the case of our patient, due to the occlusion of the SVC below the junction of the arch of the azygos vein, shunt through the azygos system occurred and blood flowed counter-current to join the right heart through inferior vena cava [10]. Moreover, thrombosis of the left supraclavicular vein might have contributed to impairing the lymphatic drainage of the left hemithorax, which relies on the thoracic duct, leading to the left-sided predominance of the pleural effusion. The combined effect of all these conditions resulted in an increased hydrostatic pressure in intercostal veins, sufficient to reveal a congenital anastomosis between a left intercostal vein and the left upper pulmonary vein (right–left shunt).
The sudden emergence of droplets from the parietal pleura during talc poudrage (nebulisation by aerosol) can be explained by pressure modifications induced by cold. Indeed, during the poudrage, the expansion of the compressed propellant gas is accompanied by an immediate decrease in temperature (−80°C), resulting in a sudden cooling of the pleural cavity. This is significant and might cause frostbite (noted in the product manual) or bradycardia during the poudrage of the mediastinal pleura [11]. Markewich et al. [11] assessed the cooling properties of a talc spray (Sclerosol; Brian Corporation, Woburn, MA, USA) in a plastic model of the chest: two temperature probes placed in the model revealed an immediate decrease in temperature after onset of talc spray that each reached 0°C within 7 s. In a study of bronchial cryotherapy, Maiwand and Homasson [12] reported a vasoconstrictive effect induced by cold as well as an increased capillary permeability. This vasoconstrictive effect was predominantly on venules. Therefore, we can suggest that the sudden cooling of the pleural cavity in our patient has induced a venous pleural vasoconstriction leading to an increase in the hydrostatic pressure, which can explain the immediate emergence of droplets of pleural fluid that we observed on the parietal pleura after talc poudrage. The visceral pleura was not affected by this phenomenon and this can be explained by the different driving pressure regimens; a more profound position of the vessels in visceral pleura compared to parietal pleura and a less important cooling of the visceral pleura, because the talc spray was mainly directed onto the parietal pleura.
In conclusion, in our patient presenting with left transudative effusion, the thoracoscopic talc poudrage through a spray has revealed, by accentuating them, the pressure changes induced by superior vena cava syndrome.
Footnotes
Conflict of interest: D. Basille has nothing to disclose.
Conflict of interest: K. Chevalier has nothing to disclose.
Conflict of interest: C. Andrejak has nothing to disclose.
Conflict of interest: V. Jounieaux has nothing to disclose.
- Received December 19, 2018.
- Accepted December 21, 2018.
- Copyright ©ERS 2019
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










