





Abstract
Introduction The study aim was to examine the association of snoring and nocturnal gastro-oesophageal reflux (nGOR) with respiratory symptoms and lung function, and if snoring and/or nGOR associated with a steeper decline in lung function.
Methods Data from the third visit of the European Community Respiratory Health Survey (ECRHS) was used for cross-sectional analysis. Pre- and post-bronchodilator spirometry was performed, and information on sleep, nGOR and respiratory symptoms was collected (n=5715). Habitual snoring and nGOR were assessed by questionnaire reports. Pre-bronchodilator spirometry from ECRHS I, II and III (20 years follow-up) were used to analyse lung function changes by multivariate regression analysis.
Results Snoring and nGOR were independently associated with a higher prevalence of wheeze, chest tightness, breathlessness, cough and phlegm. The prevalence of any respiratory symptom was 79% in subjects with both snoring and nGOR versus 56% in those with neither (p<0.001). Subjects with both snoring and nGOR had more frequent exacerbations (adjusted prevalence 32% versus 19% among “no snoring, no nGOR”, p=0.003). Snoring but not nGOR was associated with a steeper decline in forced expiratory volume in 1 s over 10 years after adjusting for confounding factors (change in % predicted −5.53, versus −4.58 among “no snoring”, p=0.04) and forced vital capacity (change in % predicted −1.94, versus −0.99 among “no snoring”, p=0.03).
Conclusions Adults reporting both habitual snoring and nGOR had more respiratory symptoms and more frequent exacerbations of these symptoms. Habitual snoring was associated with a steeper decline in lung function over time.
Abstract
Middle-aged adults with habitual snoring have a steeper decline in lung function over 10 years compared to controls. Habitual snorers with nocturnal gastro-oesophageal reflux have a higher prevalence of nocturnal respiratory symptoms than controls. http://ow.ly/YsiK30odcMY
Introduction
Sleep disordered breathing and nocturnal gastro-oesophageal reflux (nGOR) are common and comorbid conditions [1, 2], and both have inter-relationships with respiratory symptoms. Snoring is associated with respiratory symptoms such as wheezing and chronic bronchitis [3]. Individuals with both sleep disordered breathing and asthma have poorer sleep quality and a lower nocturnal oxygen saturation [4]. Even though sleep disordered breathing induces airway inflammation and airway remodelling [5, 6], it is not known if it causes changes in spirometry over time.
Respiratory symptoms are also commonly associated with nGOR and having persistent nGOR induces various respiratory symptoms. We have previously even found nGOR to associate with rhinosinusitis [7]. However, nGOR by itself is only weakly associated with changes in lung function [8–10].
As nGOR and sleep disordered breathing often co-exist and are linked by an increased prevalence in obese individuals [11, 12], it is of interest to study their combined effect on the respiratory tract. There is a stronger association between nGOR and snoring than between nGOR and the apnoea–hypopnoea index [9]. As snoring is even more prevalent in the general population, this makes snoring (a symptom of upper airway resistance) even more interesting in this context. Recent data from a small, cross-sectional study found the combination of snoring and nGOR to associate synergistically with exacerbations of respiratory symptoms, with increased microaspirations of gastric contents being one plausible explanation [8]. Otherwise, data on the respiratory effects of snoring and nGOR in combination are lacking.
The aim of the study was to examine the association of snoring and nGOR with respiratory symptoms and lung function, and to determine whether participants with snoring or nGOR had a steeper decline in lung function over a previous 20-year period.
Methods
Design and study cohort
This study is a part of the Ageing Lungs in European Cohorts (ALEC) consortium (www.alecstudy.org), which is a large research collaboration that aims to improve knowledge on risk factors of lung diseases and lung function decline. For the current study, data were used from the European Community Respiratory Health Survey (ECRHS) I, II and III, a prospective, international, population-based cohort study with three separate waves of visits over 20 years [10, 13]. First, >18 000 young adults (20–44 years old, ECRHS I) were recruited in 1991–1993. Thereafter, two examinations have taken place (at 27–57 years (ECRHS II, 1999–2003) and at 39–67 years (ECRHS III, 2010–2014)). Data for this study were available for 5715 participants from 22 European centres and one centre in Melbourne, Australia. Spirometry at ECRHS III was available from 5156 subjects.
The majority of participants in the ECRHS I were randomly selected from the general population, with an additional subgroup selected based on a positive screening questionnaire on respiratory symptoms [14]. In the current study, 759 (13%) participants came from the symptomatic sample.
Spirometry was performed on all three occasions, with reversibility testing with an inhaled β-adrenergic bronchodilator only performed in ECRHS III. Data on nGOR and snoring were only available from ECRHS III (figure 1). Therefore, analysis of lung function decline was stratified by symptoms reported at the end of follow-up.
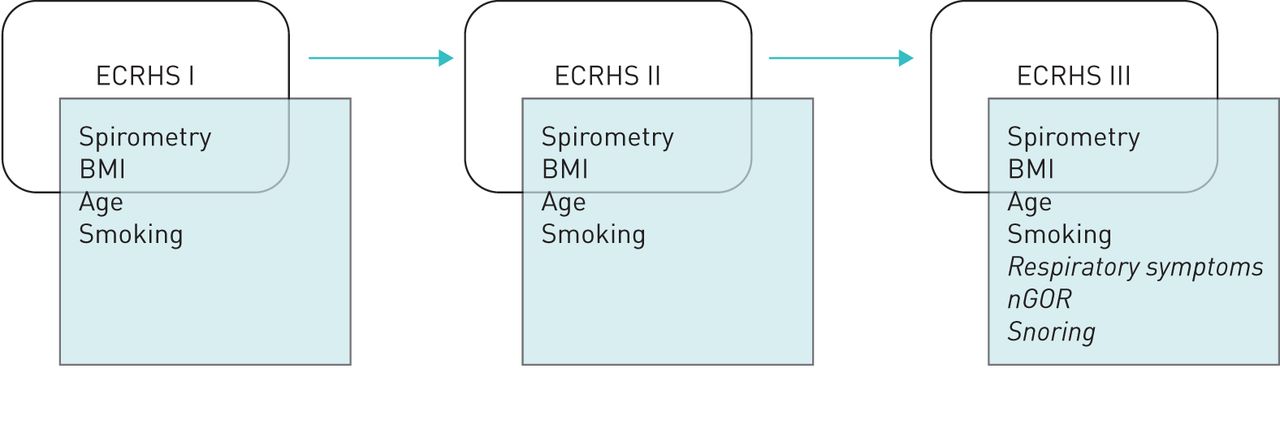
Time variant data used from the European Community Respiratory Health Survey (ECRHS) I, II and III. BMI: body mass index; nGOR: nocturnal gastro-oesophageal reflux.
Data from ECRHS III were used for a cross-sectional analysis on the association between snoring, nGOR and respiratory symptoms. Spirometry results, body mass index (BMI), age and smoking history were acquired from ECRHS I, II and III for a longitudinal analysis of lung function decline in relation to snoring or nGOR.
Nocturnal gastro-oesophageal reflux
In ECRHS III, the participants were asked how often during the last 3 months they had experienced heartburn or belching after going to bed. Participants answered on a five-step Likert scale: “Never or almost never”, “Less than once a week”, “Once or twice a week”, “Three to five nights a week” and “Almost every night” [15]. nGOR was defined as reporting heartburn or belching after going to bed once a week or more [10, 16].
Snoring
Snoring was analysed using questions from the Sleep Apnea scale of Sleep Disorders Questionnaire, only posed in ECRHS III [17]. Snoring was first assessed by the question “Have you ever been told that you snore when you sleep?” The 78% of participants who answered “yes” to that question were further assessed by the following question: “Have you been told that you snore loudly or that your snoring disturbs other people in the last 12 months?” Participants answered on a five step Likert scale: “Never”, “Seldom”, “Sometimes”, “Frequently” and “Every night”. Habitual snoring was defined as reporting to snore loudly or disturbingly frequently or every night [18].
Respiratory symptoms
The questionnaire included questions on respiratory symptoms during the previous 12 months. Symptoms included wheezing, nocturnal chest tightness, breathlessness at rest or after effort, nocturnal breathlessness, nocturnal cough, morning cough and morning phlegm. Exacerbations were defined by a positive answer to the question “In the last 12 months, have you had any episodes/times when your symptoms (cough, phlegm, shortness of breath) were a lot worse than usual?” They also reported the frequency of such exacerbations and “frequent exacerbations” was defined as two or more exacerbations in the previous 12 months. Participants also reported whether they had doctor-diagnosed asthma.
Spirometry
Lung function in ECRHS III was measured with the spirometer EasyOne (ndd Medical Technologies Inc., Andover, MA, USA) but in ECRHS I and II with the Biomedin Spirometer (Biomedin srl, Padua, Italy). A few centres differed in equipment but without notable heterogeneity in results [19]. Forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) were recorded. All subjects performed at least five forced expiratory manoeuvres and maximal values with ≥200 mL reproducibility were used for analysis. Predicted values were calculated using data from the Global Lung Function Initiative (GLI) [20].
In ECRHS III, spirometry was performed before and after bronchodilation with 200 µg salbutamol. Reversibility in FEV1 was calculated as the difference between pre- and post-bronchodilator FEV1 divided by pre-bronchodilator FEV1.
In ECRHS I and II, spirometry data were recorded similarly; however, no bronchodilation was performed. Predicted values were calculated using data from the GLI.
Change in lung function from ECRHS I to III was calculated both as change in % of predicted values between the surveys and in millilitres per year, using the actual time between the two spirometries for calculation.
Statistics
The statistical program STATA (Stata Inc., College Station, TX, USA) version 14.2 was used for statistical analysis. One-way ANOVA, Chi-squared, Wilcoxon rank-sum, multiple linear and logistic regressions were used as appropriate in cross-sectional analysis. Negative binomial regression was used for adjusted analysis of exacerbation frequency. On adjusted cross-sectional analyses of lung function, we adjusted for age, sex, centre, BMI and pack-years. On adjusted analyses of respiratory symptoms, we used the same factors for adjustment (age, sex, centre, BMI and pack-years) and added current smoking status. Lung function changes over time were first analysed by descriptive statistics without adjustments. Lung function changes over time were then analysed by multiple linear regression models, adjusting for the baseline value of the respective lung function parameter, with standard errors clustered by centre [21]. When analysing FEV1 and FVC, we also adjusted for follow-up time, baseline BMI, change in BMI, pack-years at baseline, change in pack-years, sex and age. When analysing FEV1 and FVC as % predicted, we did not adjust for sex and age at baseline, as the predicted values were already adjusted for these variables. To validate the results of the multiple linear regression model, we also performed a multilevel mixed linear regression, with centre and subject identifier (ID) as random effect variables (centre hierarchical to subject ID) but otherwise identical adjustments as above.
Results
The study comprised 5715 participants (2713 men and 3002 women); mean age was 54±7 years. Of these, 927 (16%) participants reported habitual snoring, 398 (7%) reported nGOR, and 94 (1.6%) had both snoring and nGOR (figure 2). Participants with nGOR had a higher prevalence of habitual snoring than those without nGOR (24% versus 16%, p<0.001).

Habitual snoring and nocturnal gastro-oesophageal reflux (nGOR) in the study population.
Participants reporting either habitual snoring or nGOR were slightly older and had a higher BMI than participants without habitual snoring or nGOR. Habitual snorers were more often ever-smokers and male compared to those without habitual snoring and nGOR (table 1).
Characteristics of participants in the European Community Respiratory Health Survey III stratified by snoring and nocturnal gastro-oesophageal (nGOR)
Cross-sectional symptom analysis
Overall, respiratory symptoms were more common among participants with habitual snoring and nGOR compared to those without these symptoms. Having both habitual snoring and nGOR had an additive effect on respiratory symptoms (table 2).
Unadjusted analysis of respiratory symptoms by nocturnal gastro-oesophageal reflux (nGOR) and snoring status
The association between habitual snoring (in the absence of nGOR) and respiratory symptoms remained significant after adjustment for BMI, smoking and study centre, and this was also true for the association between nGOR (in the absence of snoring) and respiratory symptoms (table 3).
Adjusted odds of respiratory symptoms and difference in lung function measures by snoring and nocturnal gastro-oesophageal reflux (nGOR)
Exacerbations: cross-sectional
Among participants reporting respiratory symptoms, the prevalence of frequent exacerbations was significantly higher among participants with the combination of both habitual snoring and nGOR compared to those without either of these symptoms (30% versus 19%, p=0.02) (figure 3). In addition, after adjusting for potential confounding factors, those with both habitual snoring and nGOR were significantly more likely to have frequent exacerbations compared to those without (adjusted prevalence 32% versus 19%, p=0.003). This association was only seen in males (adjusted prevalence in males 37% versus 17%, p<0.001; adjusted prevalence in females 25% versus 21%, p=0.66). For the whole group, the number of exacerbations reported by participants was significantly higher for those with habitual snoring and nGOR combined compared to those without habitual snoring and nGOR (incidence rate ratio 1.56, 95% CI 1.06–2.30; p=0.006) even after adjusting for confounding factors (predicted number of events 6.4 (95% CI 3.2–9.6) versus 3.6 (95% CI 3.2–4.0), p=0.02).

Exacerbations of respiratory symptoms. Only calculated for participants reporting any respiratory symptoms. nGOR: nocturnal gastro-oesophageal reflux.
Lung function: cross-sectional and changes over time
In unadjusted cross-sectional analyses, subjects that were habitual snorers had lower lung function levels than subjects without habitual snoring (table 4). Subjects with nGOR had a significantly lower pre-bronchodilator FEV1 than participants without nGOR. However, most of the associations of lung function with snoring and nGOR became statistically nonsignificant after adjustment. The only exception being a significantly higher reversibility of FEV1 after bronchodilator among habitual snorers (table 3). Adding asthma diagnosis to the regression model did not affect the increased reversibility among habitual snorers, neither when added as an independent factor nor with an interaction to snoring or nGOR (coefficient for snoring 0.40 (p=0.04) and 0.42 (p=0.01), respectively).
Unadjusted analysis of lung function by nocturnal gastro-oesophageal reflux (nGOR) and snoring status
Complete spirometry data from at least two time-points were available for 4592 subjects. Complete spirometry data from ECRHS II and III were available for 3798 subjects.
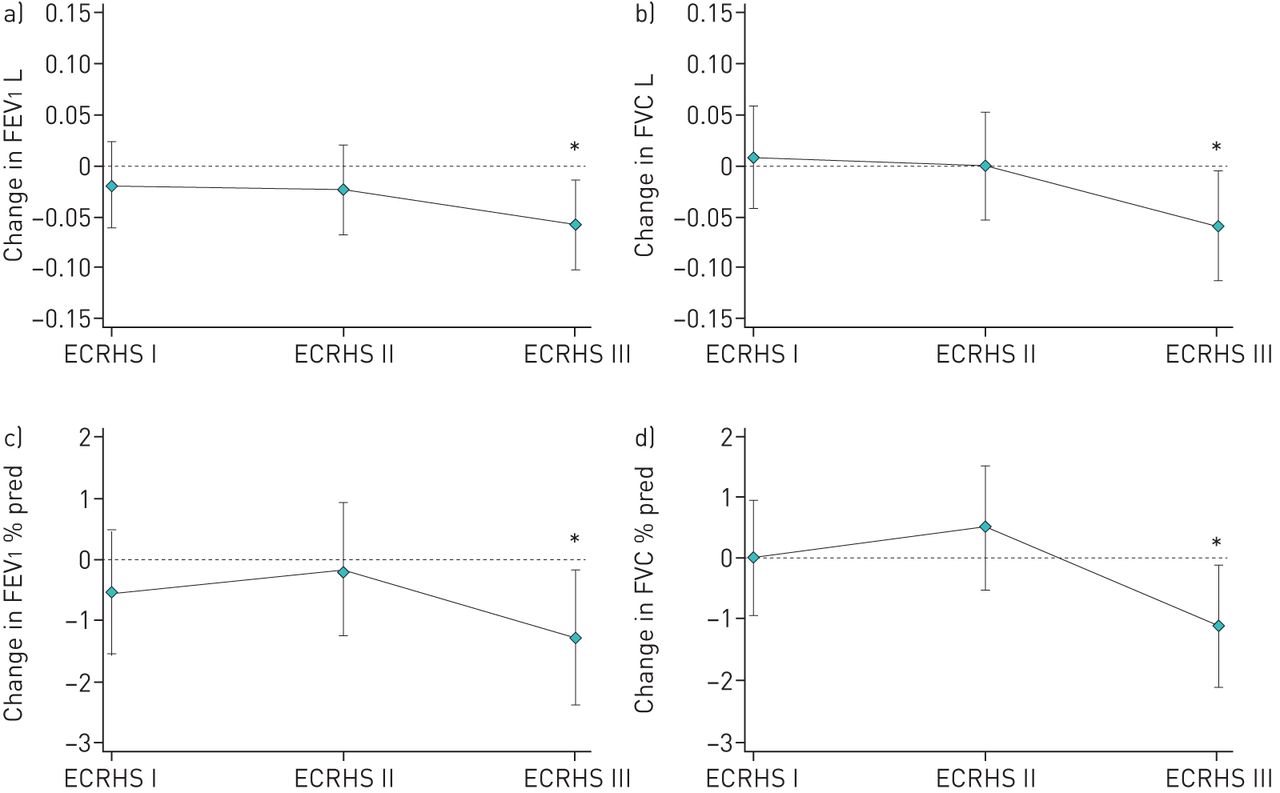
FEV1 levels decreased on average 35.4 mL·year−1 between ECRHS I and ECRHS III for the whole group, regardless of snoring and nGOR status (n=4592). Correspondingly, the FVC decreased on average 27.2 mL·year−1. When stratified by habitual snoring, the group reporting this symptom in ECRHS III was associated with a greater decline in FEV1 and FVC between ECRHS II and ECRHS III, even after adjusting for confounding factors such as BMI and smoking (n=3798) (tables 5 and 6 and figure 4). In these multiple linear regression models, the average effect of snoring can be compared to the average effect of 10 pack-years between ECRHS II and III. The first model finds FEV1 to decline, on average, by 0.9% due to snoring and 2.1% due to a smoking history of 10 pack-years. The second model finds FVC to decline on average 1.0% from snoring and 1.4% from 10 pack-years.
Mean change in lung function over the previous 20 years by snoring and nocturnal gastro-oesophageal reflux (nGOR) at follow-up
Adjusted mean change in lung function over the previous 20 years by snoring or nocturnal gastro-oesophageal reflux (nGOR) at follow-up

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The marginal effect of habitual snoring on forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC), in terms of a and b) absolute values in litres, and c and d) % of predicted, after adjusting for confounding factors such as body mass index, pack-years, centre and follow-up time. For FEV1 and FVC reported as litres, additional adjustments were made for age and sex. Graphs created from a mixed regression model; see the Methods section for details. Error bars represent 95% confidence intervals. *: p<0.05 compared to European Community Respiratory Health Survey (ECRHS) I.
A sensitivity analysis, adding doctor-diagnosed asthma to the same regression models, did not affect the results. Habitual snoring associated with a significant decline in FEV1 and FVC in percent predicted between ECRHS II and III (p=0.047 and p=0.037, respectively).
A multivariable association between nGOR and lung function decline was not seen nor did nGOR have an additive effect on the association between snoring and lung function decline.
Discussion
Using data from a large, multicentre, population-based cohort, we report a clear association between respiratory symptoms, snoring and nGOR. We found subjects with both nGOR and habitual snoring had the highest frequency of respiratory symptoms. Exacerbations of respiratory symptoms were also more frequent among participants with both nGOR and habitual snoring. We additionally found that habitual snorers had a larger retrospectively measured decline in pre-bronchodilator lung function over the preceding decade.
Respiratory symptoms
Participants with nGOR and habitual snoring had a higher prevalence of a range of respiratory symptoms, such as wheezing, breathlessness, cough and phlegm, compared to participants without nGOR and snoring. After adjustment for confounding factors, the largest difference between the controls and those with both nGOR and snoring was for the sleep-related symptoms: nocturnal chest tightness, waking up from attacks of breathlessness, coughing up phlegm in the morning and waking up from coughing. This predominance of nocturnal symptoms was noteworthy. As daytime symptoms and wheezing had, in total, a relatively similar frequency distribution, it is likely that the nocturnal symptoms do represent a specific phenotypic entity among snorers with nGOR. In addition, previous studies on patients with obstructive sleep apnoea and asthma have found asthma-related quality of life to increase and nocturnal symptoms to diminish after treatment with positive airway pressure [22, 23]. Further studies are needed to better characterise how sleep disordered breathing affects the airways, ideally including more specific markers of sleep disordered breathing and respiratory inflammatory biomarkers.
Exacerbations
Our previous study on nGOR and snoring in a smaller population, where snoring was objectively measured and nGOR assessed by a validated questionnaire, found the combination of nGOR and snoring to be associated with frequent exacerbations [8]. In the current multicentre population study, which defined snoring using questionnaire data, we confirmed this finding: having two or more exacerbations in a year was more than twice as common for participants with both nGOR and snoring when compared to those with neither. Obstructive sleep apnoea is an independent risk factor for exacerbations among asthma patients [24], and in a previous study we found pepsin in exhaled breath condensate to be increased among subjects with nGOR, as well as snoring and exacerbations of respiratory symptoms [8]. These findings support that nGOR and snoring combined may increase the risk of episodes of worsened respiratory symptoms, possibly through microaspirations of gastric contents. Our study adds that this effect seems to be important at the general-population level. Together, this implies that patients suffering from respiratory symptoms with episodic worsening should be evaluated for potential nGOR and sleep disordered breathing, and treated accordingly.
Lung function
In the current study, habitual snoring, but not nGOR, was associated with a significant decline in lung function in the preceding decade. This effect was mainly seen between ECRHS II and III, without a significant difference between ECRHS I and II. This is not surprising, as sleep disordered breathing usually increases with increasing age. This means the adverse effects of snoring should presumably be greatest under the last years of the study [25, 26]. Previous studies have found increased airway inflammation and effects on airway remodelling among subjects with obstructive sleep apnoea, and treatment with positive airway pressure may diminish the airway inflammation. This makes it plausible that sleep disordered breathing may affect the lung function [6, 27]. Our study adds that even habitual snoring in the general population may have detrimental effects on lung function over time. The significant decrease in FEV1 and FVC may be clinically meaningful and warrants further assessment.
Strengths and weaknesses
This study's main strengths lie in the well characterised and large general population cohort, with a long follow-up time. In addition, spirometry performed in the same formal manner over 20 years with at least five forced expiratory manoeuvres give further strength to the data. However, the study also has some weaknesses. First, the definition of nGOR is only based on a single question, albeit with answers on a five-point scale. However, reporting nGOR symptoms once a week or more is generally considered sufficient for subject identification [28, 29]. Regarding the analysis of changes in lung function over time, we were limited by only having data on nGOR and snoring status in ECRHS III, making the temporal relationship the opposite of the study hypothesis. However, as snoring and nGOR are conditions that often develop over a long time, it could be argued that a significant proportion may have been symptomatic over a long time. Indeed, we found that the lung function decline was greater in the second half of the study period, when snoring and nGOR were likely more pronounced. The spirometry in ECRHS I and II were only performed pre-bronchodilator, so reversibility could not be assessed over time.
Conclusion
Middle-aged adults reporting both nGOR and habitual snoring had more respiratory symptoms, and especially nocturnal respiratory symptoms, than controls. They also had more exacerbations of respiratory symptoms. Those who were habitual snorers shared greater lung function decline over the previous 10 years.
Footnotes
Conflict of interest: Ö.I. Emilsson has nothing to disclose.
Conflict of interest: S.A. Hägg has nothing to disclose.
Conflict of interest: E. Lindberg has nothing to disclose.
Conflict of interest: K.A. Franklin has nothing to disclose.
Conflict of interest: K. Toren has nothing to disclose.
Conflict of interest: B. Benediktsdottir has nothing to disclose.
Conflict of interest: T. Aspelund has nothing to disclose.
Conflict of interest: F. Gómez Real has nothing to disclose.
Conflict of interest: B. Leynaert has nothing to disclose.
Conflict of interest: P. Demoly has nothing to disclose.
Conflict of interest: T. Sigsgaard has nothing to disclose.
Conflict of interest: J. Perret has nothing to disclose.
Conflict of interest: A. Malinovschi has nothing to disclose.
Conflict of interest: D. Jarvis reports grants from the European Union and the Medical Research Council during the conduct of the study.
Conflict of interest: J. Garcia-Aymerich reports payment to her institution for consulting and lectures from AstraZeneca, and lecture fees from Esteve and Chiesi, outside the submitted work.
Conflict of interest: T. Gislason has nothing to disclose.
Conflict of interest: C. Janson has nothing to disclose.
Support statement: The ALEC Study is funded by the European Union's Horizon 2020 Research and Innovation programme under grant agreement number 633212. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received January 10, 2019.
- Accepted March 11, 2019.
- Copyright ©ERS 2019
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References









