





Abstract
Novel methodological approaches now demonstrate that the unique elastin degradation products desmosine and isodesmosine are detectable in plasma of cystic fibrosis patients and correlate to lung function, exacerbation frequency and disease progression http://bit.ly/2VwZOcx
To the Editor:
Monitoring the integrity of the lungs using biomarkers is a major goal as an indicator for patient prognosis, especially in diseases like cystic fibrosis (CF) where 85% of mortality is a result of lung disease [1]. Advances in the precision of current biomarkers and identification of new biomarkers are needed to accelerate CF drug development. The development of biomarkers to reflect disease progression or the effect of new therapy has the potential to improve patient care and new drug discovery. Systemic monitoring of biomarkers via body fluids such as blood sampling is ideal as a relatively noninvasive approach to monitor patient disease progression. Blood can easily be obtained from patients of all ages despite lung disease severity. An ideal biomarker for CF disease progression would allow diagnosis of patients following an exacerbation and monitor changes in response to treatment [2]. The airways of CF patients have a large population of neutrophils that are associated with the lung inflammation and tissue remodelling observed with the disease [3]. The abundance of neutrophils and their intracellular components, such as neutrophil elastase [4], alter the lung microenvironment for example the extracellular matrix proteins, which represent plausible targets for biomarkers. The unique elastin degradation products desmosine and isodesmosine (DI) are stable cross-linking amino-acids that are detectable in body fluids as indicators of lung damage [5], and are proposed as biomarkers for lung disease severity. Elastin degradation is reported to be increased in patients with CF [6], with elevated DI levels observed in the urine of CF patients. However, as DI is present at extremely low concentrations in body fluids, their precise and specific measurement has been a challenge and until recently were not envisioned as a viable biomarker. Using a quantitative ion mobility-mass spectrometry (MS) method to analyse free DI, DI concentrations are consistently detected and are enhanced in the urine of chronic obstructive pulmonary disease (COPD) patients relative to healthy controls [7]. The increased sensitivity in the method of analysis of DI increases specificity and sensitivity for DI measurements in body fluids, including plasma, sputum, bronchoalveolar lavage fluid and urine [8, 9]. The liquid chromatography–tandem mass spectrometry (LC–MS/MS) method can avoid homologous interference of both desmosine and isodesmosine. When detecting DI by ultraviolet or ELISA, DI levels detected in plasma are higher and have more signal-to-noise than the LC–MS/MS method. Here, we investigate plasma samples from CF patients for DI levels and determined whether DI levels in plasma correlates with pulmonary function and the frequency of annual exacerbations.
We used plasma samples collected from both male and female CF patients and healthy volunteers (n=12 per group, see figure 1a). 12 patients had CF confirmed by sweat testing or genotyping, and were compared with 12 non-CF control patients. Full informed consent was obtained before the procedure according to a protocol approved by Beaumont Hospital Ethics Committee. Genotyping demonstrated that the allelic frequency for the ∼F508 mutation was 100%; 3 (25%) out of 12 were homozygotes; and 25%, 16.66%, 8.33%, 8.33% and 8.33% were compound heterozygotes for ∼G551D, R560T-K, R117H, 621+1G->T and 3007G, respectively. At the time of evaluation, five of the subjects had an acute exacerbation of the lung disease. All healthy adults had no history of respiratory disease, and all had normal physical examinations. High-performance liquid chromatography (HPLC) and tandem MS was utilised as previously described [10]. Analyses of DI levels were performed in triplicate on 12 samples per group on subsequent days. DI levels were normalised to urea levels. The coefficient of variation of the method is 8%. The detection limit of DI is 0.05 ng·mL−1 for the electrospray ionisation mode. Plasma samples with a DI content <0.1 ng·mL−1 required concentration.

{kind=link}
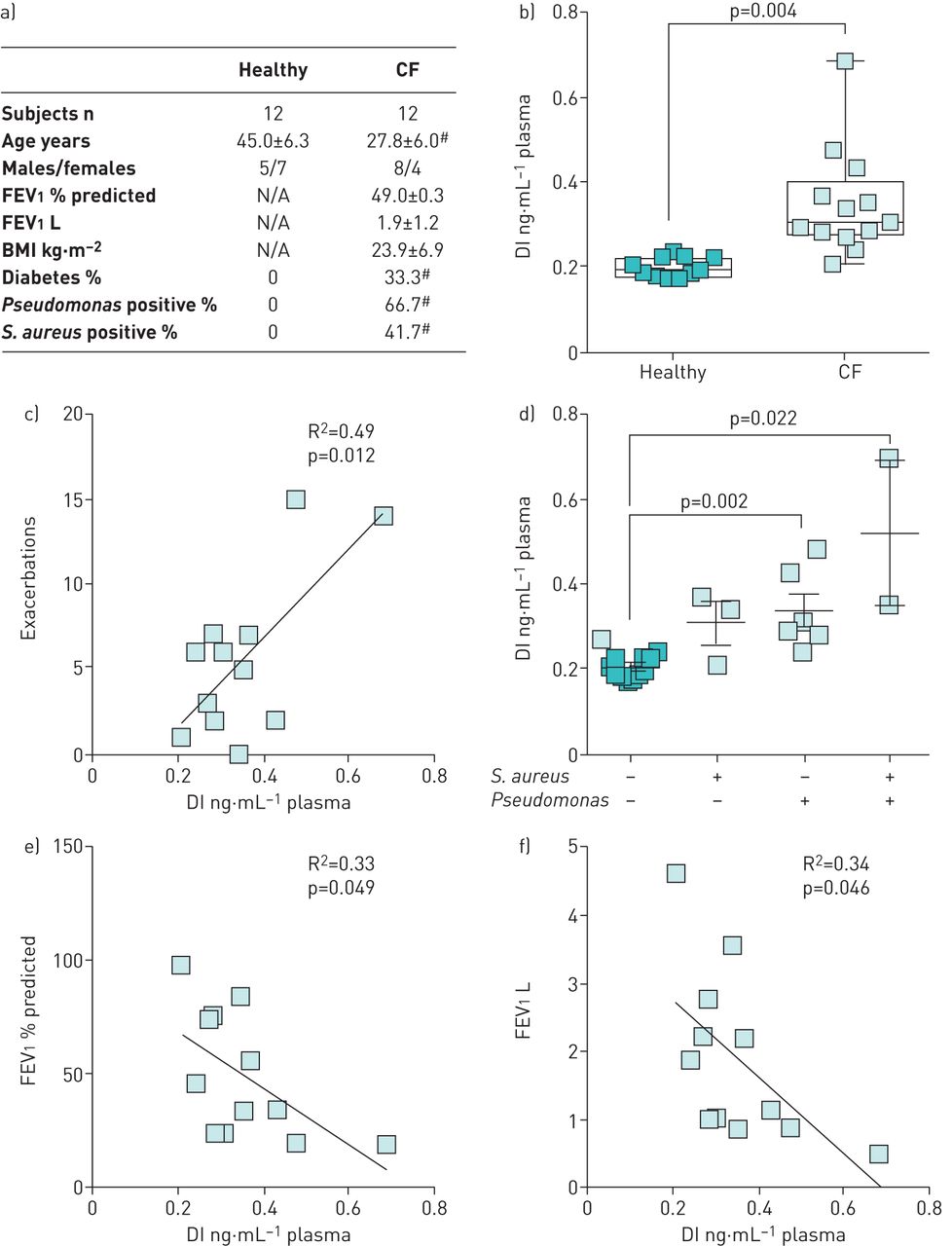
Cystic fibrosis (CF) patients have elevated plasma desmosine and isodesmosine (DI) levels compared with healthy subjects. a) Patient demographics. #: denotes a statistically significant difference between groups. b) DI levels were determined in plasma from 12 healthy and 12 CF patients. Box plots represent mean±sem, where each measurement was performed three times on each sample. Groups were compared by the D'Agostino and Pearson omnibus normality test and by Mann–Whitney tests. c) Plasma DI levels were correlated with the frequency of disease exacerbations in the past 12 months. d) DI levels were examined in plasma from patients colonised by Staphylococcus aureus (S. aureus), Pseudomonas or both. e) Forced expiratory volume in 1 s (FEV1) (% predicted) and f) FEV1 (L) levels were plotted against plasma DI levels in CF patients. The R2 and p-value is shown for each correlation, determined by linear regression analysis. All analysis was performed using GraphPad Prism Software (Version 5 for Mac OS X; GraphPad Software, La Jolla, CA, USA). BMI: body mass index.
Plasma DI levels from healthy individuals were significantly lower than in the plasma from CF patients, with a mean±sem of 0.20±0.02 ng·mL−1 (n=12) and 0.35±0.13 ng·mL−1 (n=12), respectively (figure 1b). The CF patients in this study suffered frequent exacerbations and the frequency of these exacerbations correlated with the plasma concentration of DI within in the CF group (figure 1c). Importantly, plasma from Pseudomonas positive patients had significantly higher levels of DI (figure 1d). This is important as isodesmosine is a chemoattractant for Pseudomonas aeruginosa [11] and could contribute to further infection. Pulmonary function tests revealed that plasma DI levels negatively correlate with forced expiratory volume in 1 s expressed in litres or % predicted (fig. 1e and f). These data demonstrate statistically significant increases in levels of DI in plasma in a small pilot study of CF patients and suggest that this improved methodology for testing DI levels in body fluids may be an effect means of monitoring disease progression in CF patients.
The need for biomarkers in CF cannot be understated, with ∼25% of exacerbations in CF patients resulting in permanent loss of lung function despite antibiotic therapy [12]. Using DI plasma measurements, a clear correlation is observed in exacerbation frequency and DI levels with only 12 samples. Our data suggests that DI plasma levels reflect severity of disease in CF patients and monitoring DI plasma levels could contribute to therapy selection and the subsequent improvement of patient care. The detection and measurement of DI as a means to study elastin degradation has been used for almost 30 years, but recent methodological advances by our group and others have aided in DI detection, as the concentrations present in body fluids are extremely low. In fact, others have described correlations between urine desmosine excretion and the severity of lung disease in the patients with CF, using the chest radiograph score and morphological evidence for proteolytically damaged elastin in the lungs [6]. Earlier methodological approaches were immunological and isotope dilution-based techniques. To improve the specificity and sensitivity of DI measurement, we developed an analytical method using HPLC followed by electrospray ionisation MS [8] and DI levels are then measured by molecular ion mass-to-charge ratio. Using this method, enhanced DI levels were identified in plasma and sputum from COPD patients [7]. The ratio of free to bound DI correlated with lung function, unlike total desmosine levels, which can be variable even in patients with similar levels of lung disease [13]. We also used tandem MS to detect the reaction ion M/Z-481 and M/Z-395, thereby allowing confirmation of molecular specificity and accuracy of measurement. We have validated the use of DI as a sensitive biomarker in α1-antitrypsin (AAT) deficiency with patients receiving intravenous augmentation therapy having less DI in their plasma [14]. This is important as this randomised, double-blind, placebo-controlled trial (RAPID trial) demonstrated a significant reduction in lung density decline in patients with AAT deficiency receiving α1-proteinase inhibitor versus placebo [15].
Our data links plasma DI levels to lung function and disease decline in CF. The quantification method of DI requires several levels of purification and complex detection methodology, which adds to the cost of screening. However, due to this stringent methodology, consistent data readings outweigh other limitations for the use of DI as a biomarker for CF patient samples. As yet, we have not correlated DI levels with lung function in healthy controls or specifically targeted critical thresholds for DI and loss of lung function. Future studies will need to address these limitations. There are several levels of evidence to suggest that using DI as a biomarker for CF is feasible, as elastin degradation is a recognised occurrence in the pathogenesis of CF [6] and current methodologies allow the accurate measurement of DI in all body fluids. Currently, there is little to no data correlating DI to current medications, apart from antibiotic treatment [16]. DI is a consistent correlating readout to lung function and therefore could be also used as a biomarker for CF and provide a means to test the beneficial effects of current and future medications.
Footnotes
Conflict of interest: S. Ma has no financial conflicts of interest to disclose.
Conflict of interest: P. Geraghty has no financial conflicts of interest to disclose.
Conflict of interest: A. Dabo has no financial conflicts of interest to disclose.
Conflict of interest: C. McCarthy has no financial conflicts of interest to disclose.
Conflict of interest: N.G. McElvaney has no financial conflicts of interest to disclose.
Conflict of interest: G.M. Turino has no financial conflicts of interest to disclose.
- Received December 19, 2018.
- Accepted April 29, 2019.
- Copyright ©ERS 2019
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References









