





Abstract
Upper airway obstruction with decreased central drive (ODCD) is one of the causes of ineffective noninvasive ventilation (NIV) in amyotrophic lateral sclerosis (ALS). The aim of this study is to determine the mechanism responsible for ODCD in ALS patients using NIV.
This is a prospective study that included ALS patients with home NIV. Severity of bulbar dysfunction was assessed with the Norris scale bulbar subscore; data on upper or lower bulbar motor neuron predominant dysfunction on physical examination were collected. Polysomnography was performed on every patient while using NIV and the ODCD index (ODCDI: number of ODCD events/total sleep time) was calculated. To determine the possible central origin of ODCD, controller gain was measured by inducing a hypocapnic hyperventilation apnoea. Sonography of the upper airway during NIV was performed to determine the location of the ODCD.
30 patients were enrolled; three (10%) had ODCDI >5 h−1. The vast majority of ODCD events were produced during non-rapid eye movement sleep stages and were a consequence of an adduction of the vocal folds. Patients with ODCDI >5 h−1 had upper motor neuron predominant dysfunction at the bulbar level, and had greater controller gain (1.97±0.33 versus 0.91±0.36 L·min−1·mmHg−1; p<0.001) and lower carbon dioxide (CO2) reserve (4.00±0.00 versus 10.37±5.13 mmHg; p=0.043). ODCDI was correlated with the severity of bulbar dysfunction (r= −0.37; p=0.044), controller gain (r=0.59; p=0.001) and CO2 reserve (r= −0.35; p=0.037).
ODCD events in ALS patients using NIV have a central origin, and are associated with instability in the control of breathing and an upper motor neuron predominant dysfunction at the bulbar level.
Abstract
Upper airway obstructions in ALS patients using NIV have a central origin, and are associated with instability in the control of breathing and an upper motor neuron predominant dysfunction at the bulbar level http://bit.ly/2WEMt28
Introduction
Amyotrophic lateral sclerosis (ALS) is a neurodegenerative disease of unknown origin that involves loss of corticospinal tract, bulbar and spinal motor neurons [1]. Respiratory problems related to respiratory muscle weakness are the main causes of morbidity and mortality in ALS patients [2]. The use of noninvasive respiratory muscle aids, such as noninvasive ventilation (NIV) and assisted cough techniques, has been shown to prolong survival, relieve symptoms, avoid hospitalisations and improve quality of life in ALS [3, 4].
NIV effectiveness in correcting nocturnal desaturations is a prognostic factor in those ALS patients using NIV [5]. The severity of bulbar dysfunction is linked to the effectiveness of NIV in ALS, both when patients are in a medically stable condition and when suffering acute chest episodes [6, 7]. Moreover, the effectiveness of mechanically assisted coughing is linked to the behaviour of the upper airway [8]. It has been found that, during NIV, upper airway obstruction with decreased central drive (ODCD) events, which presented in 45% of patients after correction of leaks, are one of the causes of ineffective NIV [9]. These obstructive events are associated with a poor prognosis and lower survival; when ODCD events are corrected, survival improves [9]. The importance of these ODCD events during NIV in ALS is crucial because even those patients who present such episodes without nocturnal desaturations and who are theoretically adequately ventilated have poor survival, in the same way as those patients who are thought to be inadequately ventilated [9]. Unfortunately, no effective treatment has been identified for those ODCD events that cannot be reverted with changes to ventilator parameters.
In order to improve the management of respiratory problems in ALS patients and given that 10% of ALS patients using NIV suffer ODCD events despite the adjustment of ventilator settings [9], with a negative impact on survival, the aim of this study is to determine the mechanism responsible for ODCD events in ALS patients using NIV.
Materials and methods
This is a prospective study that included, after informed consent, patients diagnosed with probable or definitive ALS, diagnosed according to the revised El Escorial criteria [10], managed at the Respiratory Care Unit of the Hospital Clínico Universitario (Valencia, Spain) for whom NIV was indicated according to the American College of Chest Physicians criteria [11]. All the patients were in a medically stable condition. Exclusion criteria were refusal to participate, bronchial pathology or associated illness with a poor prognosis, use of NIV for >18 consecutive h·day−1 and refusal of NIV. The study protocol was approved by the hospital's ethics committee.
Demographic, clinical and respiratory function assessment data were collected. Clinical assessment included the use of the Revised Amyotrophic Lateral Sclerosis Functional Rating Scale [12] and the Norris scale bulbar subscore [13]. Data concerning age, sex, body mass index, upper or lower bulbar motor neuron predominant dysfunction on physical examination, ALS onset and time from ALS onset to NIV were also collected.
Respiratory function was assessed by means of spirometry (MS 2000; C. Schatzman, Madrid, Spain), performed in accordance with the European Respiratory Society guidelines and using suggested reference values [14], recording forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1) and FEV1/FVC. Maximum inspiratory pressure (PImax) and maximum expiratory pressure (PEmax) were measured at the mouth (Electrometer 78.905A; Hewlett-Packard, Andover, MA, USA) while the cheek was held. PImax was performed close to residual volume and PEmax was performed close to total lung capacity, with the pressures sustained for 1 s being measured [15]. Three measurements with <5% variability were recorded and the highest value was used for the data analysis. Sniff nasal inspiratory pressure (SNIP) was measured in an occluded nostril during a maximal sniff through the contralateral nostril (Micro RPM; MicroMedical, Rochester, UK). SNIP was measured during 10 maximal sniffs performed at functional residual capacity and the highest recorded pressure was used [16]. Maximum insufflation capacity (MIC), peak cough flow (PCF), manually assisted PCF (PCFMIC) and mechanically assisted PCF (PCFMI-E) were measured as described in previous studies [17].
Study protocol
The study protocol was performed over 2 nights at the Respiratory Care Unit during a hospital admission.
Polysomnography
During the first night, polysomnography (Alice 5; Philips Respironics, Murrysville, PA, USA) was performed according to the American Academy of Sleep Medicine recommendations on every patient while using NIV [18]. NIV parameters were set similar to those set for home NIV for each patient. Data for the following parameters were collected: total sleep time (TST), sleep efficiency index (total sleep time/total recording time), sleep latency, rapid eye movement (REM) latency, total time in each sleep stage, percentage of time with arterial oxygen saturation measured by pulse oximetry (SpO2) <90% (TST90), mean SpO2, minimum SpO2, mean heart rate, arterial blood gases upon waking, number of ODCD events, number of ODCD events during each sleep stage, ODCD index (ODCDI: number of ODCD events/TST), number of total respiratory events (air leaks and obstructive events with or without decreased central drive), number of patient–ventilator asynchronies (ineffective trigger, auto-trigger, double-trigger, flow mismatch, delayed cycling and prolonged cycling) and patient–ventilator asynchrony index (number of patient–ventilator asynchronies/TST).
ODCD events were defined as periods of ≥10 s with an increase in PImax, a distortion in the airflow waveform in volume ventilator mode or a decrease in airflow without a change in pressure in pressure ventilator mode and a reduction or disappearance of the thoracoabdominal belt signal [19]. These episodes can be enclosed with desaturations and/or arousals. A value of 5 h−1 for ODCDI was taken as significant for our analysis [9].
Ventilation was considered effective when TST90 while using NIV was <5%, arterial carbon dioxide tension (PaCO2) <45 mmHg, air leaks >24 L·m−1 occurred <20% of the recorded time, presence of respiratory events and asynchronies occurred <20% of the recorded time, and hypoventilation-related symptoms were relieved [20].
Sonographic images of the upper airway during NIV (Logiq F6; GE Healthcare, Hatfield, UK) were obtained using a high-frequency linear transducer (7.5 MHz) that was oriented transversally across the anterior surface of the neck at the level of the thyroid cartilage [21].
Control of breathing assessment
The stability/instability of the respiratory control breathing system was assessed on the basis of the concept of “loop gain”, i.e. the ratio of the response of a system to the disturbance that this response produces; changes in ventilation produce changes in arterial blood gases that trigger corrective actions from the controller, in order to restore the ventilatory drive to the baseline level [22]. Loop gain has three components: controller gain from the central respiratory controller, plant gain deriving from the efficiency in CO2 excretion, and mixing gain from the delay imposed by haemoglobin binding, circulation and diffusion [22]. During a second night, loop gain was measured by inducing a hypocapnic hyperventilation apnoea with pressure support ventilation (Trilogy 100; Philips Respironics) through an oronasal mask during regular sleep hours, according to the method described by Zhou et al. [23].
A gas analyser to measure end-tidal CO2 tension (PETCO2) (EMMA Capnograph; Masimo, Irvine, CA, USA) was placed in the circuit between the mask and the ventilator. Polysomnography recordings were taken. The ventilator was set at an expiratory positive airway pressure (EPAP) of 2 cmH2O; during periods of hyperventilation the ventilator was set on spontaneous timed mode, with timing matched to each patient's eupneic rate. Hyperventilation was achieved by increasing the inspiratory positive airway pressure (IPAP) of the ventilator. For each successive trial, the IPAP was increased by 1 cmH2O increments from the initial level of 2 cmH2O. Mechanical ventilation was continued for 3 min and was terminated during expiration by decreasing the support to the baseline EPAP. A mechanical ventilation trial of each IPAP was repeated twice, with trials separated by a minimum of 3 min. All trials were performed during stable non-REM (NREM) sleep (stage N2 or N3).
For each trial, three periods were established: 1) the control period, which was represented by the mean average of five spontaneous breaths immediately preceding the onset of mechanical ventilation; 2) the hyperventilation period during performance of mechanical ventilation; and 3) the recovery period immediately after removing mechanical ventilation. Hypocapnic central apnoeas were recorded during the recovery period. Central apnoea was defined as a period of no airflow for at least 5 s.
Minute ventilation (V′E) and PETCO2 were recorded during the control period and the last five mechanical breaths of the hyperventilation period, before the ventilator was turned back to the baseline EPAP. During the recovery period central apnoea was considered when V′E=0 L·min−1. In those trials in which the apnoea occurred during the recovery period, the apnoeic threshold was defined as the PETCO2 measured during the hyperventilation period. The CO2 reserve (CO2R) was defined as the change in PETCO2 between eupneic PETCO2 measured during the control period and the apnoeic threshold. Controller gain was defined as the ratio of the change in V′E between control and apnoea to the corresponding CO2R. Plant gain was calculated using a hyperbolic first-order function, plotting PETCO2 during control periods against V′E during the last five mechanical ventilation breaths; the slope of the curve at the PETCO2 operating point (mean PETCO2 during control periods) was calculated. Plant gain was defined as the inverse of the slope at the operating point [23].
Statistical analysis
Binary and categorical variables were summarised using frequency counts and percentages. Continuous variables were expressed as means with standard deviations. Data comparisons were performed using the t-test and the Mann–Whitney test for normally and nonnormally distributed data, respectively. Dichotomous variables were compared with the Chi-squared test. Pearson correlation coefficients were used to assess the association between the different parameters in normally distributed data and the Spearman correlation test in nonnormally distributed data. Statistical significance was taken as p<0.05.
Results
30 consecutive ALS patients using NIV at home were included in the study. All of them were using NIV at home in volume-assisted/control mode. All the enrolled patients presented some degree of bulbar dysfunction: 19 (63.3%) with lower motor neuron predominant dysfunction at the bulbar level and 11 (36.7%) with upper motor neuron dysfunction. Data on demographics, respiratory function and functional assessment of the patients included in the study are shown in table 1. 29 patients (96.7%) were using mechanically assisted coughing at home and nine patients (30%) had a gastrostomy for enteral nutrition.
Demographic and pulmonary function in the total population and the groups with obstruction with decreased central drive index (ODCDI) <5 and >5 h−1
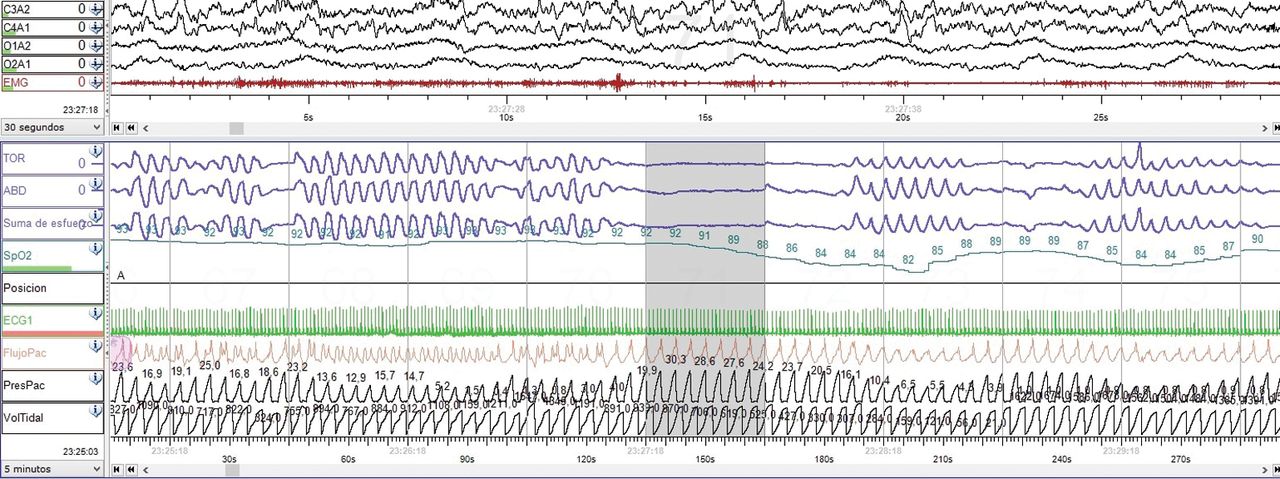
Table 2 displays the results of the polysomnography recordings. Three patients (10%) presented with ODCDI >5 h−1 (figure 1). Statistical differences were found between those with ODCDI <5 h−1 and those with ODCDI >5 h−1 in terms of percentage REM sleep stage, oxygen desaturation index and arterial carbon dioxide tension (PaCO2) (tables 1 and 2). The vast majority of ODCD events were produced in NREM sleep stages (N1 24.87%, N2 56.91%, N3 10.7%, REM 7.4%). No differences were found in tidal volume programmed on the device between those patients with ODCDI <5 h−1 and those with ODCDI >5 h−1 (827.40±185.67 versus 625.00±106.06 mL; p=0.144) and time spent daily with NIV at home (9.18±3.05 versus 8.00±0.00 h; p=0.513).
Polysomnography while using noninvasive ventilation and gas exchange parameters in the groups with obstruction with decreased central drive index (ODCDI) <5 and >5 h−1

Polysomnography recording of an obstructive event in the upper airway with decreased central drive in a patient with amyotrophic lateral sclerosis using noninvasive ventilation in volume-preset mode.
The patient–ventilator asynchrony index for the whole population was 0.98±1.40 h−1, with ineffective triggering the most frequently detected problem.
Central control of breathing
Those patients with ODCDI >5 h−1 had higher controller gain values (1.97±0.33 versus 0.91±0.36 L·min−1·mmHg−1; p<0.001) and lower CO2R (4.00±0.00 versus 10.37±5.13 mmHg; p=0.043) (figure 2). No differences were found between those with ODCDI >5 h−1 and those with ODCDI <5 h−1 in terms of apnoeic threshold (40.66±8.68 versus 38.22±6.24 mmHg; p=0.538) and plant gain (1.80±0.70 versus 2.02±1.4 mmHg·L−1·min−1; p=0.256).

{kind=link}
{kind=link}
Relationship between minute ventilation (V′E) and end-tidal carbon dioxide tension (PETCO2) representing controller gain (CG) in two amyotrophic lateral sclerosis patients, one with obstruction with decreased central drive index (ODCDI) <5 h−1 and another with ODCDI >5 h−1.
In those patients with ODCDI >5 h−1, no statistically significant differences were found between V′E during NIV (10.00±1.69 L·min−1), V′E during spontaneous quiet breathing (7.90±1.36 L·min−1; p=0.258) and V′E needed to produce the hypocapnic apnoea during a hyperventilation period (13.56±8.17 L·min−1; p=0.489). Regarding those patients with ODCDI <5 h−1, V′E during NIV (12.54±3.09 L·min−1) was higher than V′E during quiet spontaneous breathing (8.32±2.32 L·min−1; p<0.001) and lower than V′E used to cause a hypocapnic apnoea (18.00±5.09 L·min−1; p<0.001).
Bulbar dysfunction
Although no differences were found in the severity of bulbar dysfunction (table 1), 100% of the patients with ODCDI >5 h−1 had upper motor neuron predominant dysfunction at the bulbar level; however, only 29.62% of the patients with ODCDI <5 h−1 had bulbar upper motor neuron impairment (p=0.41).
Sonograms taken during NIV showed that those ODCD episodes were caused by glottic closure events in all patients (see videos in the supplementary material).
Relationship of obstructive events
ODCDI was significantly associated with the severity of bulbar dysfunction, CO2R and controller gain (table 3).
Associations with the obstruction with decreased central drive index
Ineffective NIV was present in all patients with ODCDI >5 h−1 (100%) and only in 25.92% of those patients with ODCDI <5 h−1 (p=0.01). The cause of ineffective ventilation in all patients with ODCDI <5 h−1 was the presence of air leaks.
Discussion
The findings of this study show that ALS patients who present ODCD events while using NIV have more instability in control of breathing and have upper motor neuron predominant dysfunction at the bulbar level; moreover, these obstructive events are associated with ineffective NIV.
The presence of ODCD events in ALS patients using NIV has a negative impact on survival [5, 9], and in our patients ODCD events and air leaks are the main causes of ineffective NIV. Several mechanisms have been proposed as the causes of these ODCD events [9]: central neural dysregulation with instability in control of breathing, severity of bulbar dysfunction with upper airway collapse due to hypotonia in lower motor neuron predominant dysfunction at the bulbar level or hyperreflexia in upper motor neuron predominant dysfunction, central apnoeas due to hyperventilation with reduction in PaCO2 induced by NIV and inhibition of the ventilatory drive triggered by thoracic afferents stimulated by NIV.
Respiratory problems in ALS patients are derived from respiratory muscle weakness due to motor neuron degeneration. However, based on the results of recent studies, some authors suggest the involvement of voluntary and involuntary components of central control of breathing in ALS [24, 25]. Nocturnal desaturations have been reported in both NREM and REM sleep stages in ALS patients with preserved respiratory function and intact electrodiagnostic tests [26, 27]. Some studies have found that phrenic conduction and diaphragmatic response persists in response to cervical magnetic stimulation, contrasting with a slowdown of the response or its disappearance with transcranial magnetic stimulation [28, 29]. In this respect, Onders et al. [30] found that, in some ALS patients with minimal or absent electromyographic spontaneous activity of the diaphragm, direct stimulation produces a brisk contraction, suggesting the preservation of the corticorespiratory pathways and the probable degeneration of the central respiratory centres. The proposed areas involved include the medullary dorsal and ventral respiratory pre-motor neurons and the interneurons of the pre-Bötzinger complex [24, 25].
The results of the present study show more instability in control of breathing, reflected in a longer controller gain and a lower CO2R, in those ALS patients with ODCDI >5 h−1 during NIV. As the loop gain is higher in such patients, the tendency for ventilatory instability in response to a disturbance is also greater. A large controller gain promotes instability because it leads to a greater ventilatory overshoot in response to CO2 accumulation and a greater ventilatory undershoot in response to decreased CO2 [31]. A central apnoea during NIV results from this instability, as occurs with other pathologies [32]. Plant gain, which reflects the response of CO2 to changes in V′E, depends on lung volumes [33]; thus, we found no difference in this respect between the two groups of patients, i.e. those with ODCDI <5 and >5 h−1, who both have low lung volumes as a consequence of their neuromuscular disease. Such central apnoeas deriving from the instability in control of breathing are mainly produced during NREM sleep stages, as can be seen in our results, because, in these sleep stages, control of breathing is critically dependent upon chemical and mechanical reflex feedback. During these central apnoeas caused by a decrease in central drive, an upper airway obstruction is produced; it has been described as an increase in the activity of the thyroarytenoid muscle leading to glottic closure and a collapse of the oropharynx during expiration [34, 35]. These features are consistent with the sonographic images obtained for our patients with ODCDI >5 h−1.
Regarding bulbar dysfunction, all of our patients had a certain degree of bulbar impairment and so no differences were found in the severity between the two groups; however, those patients with ODCDI >5 h−1 had upper motor neuron predominant dysfunction at the bulbar level. This suggests two underlying problems: degeneration of the corticobulbar pathways and hyperreflexia at the bulbar level, leading to a more forceful response of the upper airway to the central apnoea induced by the instability in the control of breathing, and then a glottic closure due to the mechanical stimulus of the upper airway. Furthermore, our findings in the three patients with ODCDI >5 h−1 (no differences in V′E during spontaneous breathing, V′E during NIV and V′E during hyperventilation to induce an apnoea) allow us to rule out, as causes of ODCD events, hyperventilation induced by NIV and inhibition of the ventilatory drive triggered by NIV-induced thoracic afferents stimulation, although it would have been more suitable to measure CO2 during all of the night using NIV.
We have found that ODCD events while using NIV in ALS are more frequent during NREM sleep stages; however, Georges et al. [9] recently found ODCD events to be more frequent during REM sleep in 20 patients in whom polysomnography was performed. Moreover, Georges et al. [9] were able to resolve ODCD events in some patients by increasing EPAP up to 10 cmH2O, but they did not report whether their patients had upper or lower motor neuron predominant dysfunction at the bulbar level or whether obstructive events were resolved during NREM or REM sleep, and they used pressure-cycled ventilator mode rather than volume-cycled mode as with our patients. Following the procedure described by Georges et al. [9], we increased EPAP up to 10 cmH2O during NIV in our patients with ODCDI >5 h−1, but no ODCD events were resolved by doing so. Another cause of obstructive events during NIV described in the literature is the use of oronasal masks, which may be resolved by transferring to nasal NIV, although patient numbers in the published studies are low with regard to ALS [36–38]. In an attempt to achieve effective NIV, we trialled the use of a nasal mask in our patients with ODCDI >5 h−1. However, in two of our patients NIV was ineffective due to excessive air leaks through the mouth and in the other patient the obstructive events were not resolved.
This study has some limitations. The number of subjects enrolled in the study is low and the number of patients in which ODCD events were detected is also low. This fact may have reduced the statistical power; thus, the results must be taken with caution and more studies are needed to confirm our findings. Sleep state instability may influence the apnoeic threshold and the hypocapnic ventilatory response, and here we have only considered stable N2 and N3 sleep states. Controller gain is influenced by those factors that determine the ventilatory response to changes in blood gases; one of these factors is respiratory muscle strength [31], which is reduced in ALS patients needing NIV. However, no differences were found between the two ODCDI groups in those functional respiratory parameters that, directly or indirectly, evaluate respiratory muscle strength. We have not assessed the performance of the oropharynx during NIV with fibreoptics, as other studies have done: insertion of a tube into the upper airway during NIV can produce disturbances in airflow from the ventilator, which could trigger upper airway reflexes in those patients with upper motor neuron impairment.
In conclusion, ODCD events in ALS patients using NIV have a central origin, and are associated with instability in the control of breathing and with upper motor neuron predominant dysfunction at the bulbar level. Moreover, these events are a cause of NIV ineffectiveness.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00099-2019.supp
Video 1 00099-2019.video1
Video 2 00099-2019.video2
Footnotes
This article has supplementary material available from openres.ersjournals.com
Author contributions: E. Servera and J. Sancho conceived and designed the study, acquired the data, analysed and interpreted the data, drafted the article, and gave final approval of the submitted version. E. Burés, S. Ferrer, A. Ferrando and P. Bañuls acquired the data, drafted the article and gave final approval of the submitted version. J. Sancho is responsible for the overall content of the manuscript as guarantor
Conflict of interest: J. Sancho has nothing to disclose.
Conflict of interest: E. Burés reports grants from Institute Health Research INCLIVA outside the submitted work.
Conflict of interest: S. Ferrer has nothing to disclose.
Conflict of interest: A. Ferrando has nothing to disclose.
Conflict of interest: P. Bañuls has nothing to disclose.
Conflict of interest: E. Servera has nothing to disclose.
- Received April 18, 2019.
- Accepted May 30, 2019.
- Copyright ©ERS 2019
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










