





Abstract
Electrical impedance tomography (EIT) is able to detect rapid lung volume changes during breathing. The aim of our observational study was to characterise the heterogeneity of regional ventilation distribution in lung-healthy adults by EIT and to detect the possible impact of tobacco consumption.
A total of 219 nonsmokers, asymptomatic ex-smokers and current smokers were examined during forced full expiration using EIT. Forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and FEV1/FVC were determined in 836 EIT image pixels for the analysis of spatial and temporal ventilation distribution. Coefficients of variation (CVs) of these pixel values were calculated. Histograms and medians of FEV1/FVCEIT and times required to exhale 50%, 75%, 90% of FVCEIT (t50, t75 and t90) were generated.
CV of FEV1/FVCEIT distinguished among all groups (mean±sd: nonsmokers 0.43±0.05, ex-smokers 0.52±0.09, smokers 0.62±0.16). Histograms of FEV1/FVCEIT differentiated between nonsmokers and the other groups (p<0.0001). Medians of t50, t75 and t90 showed the lowest values in nonsmokers. Median t90 separated all groups (median (interquartile range): nonsmokers 0.82 (0.67–1.15), ex-smokers 1.41 (1.03–2.21), smokers 1.91 (1.33–3.53)).
EIT detects regional ventilation heterogeneity during forced expiration in healthy nonsmokers and its increase in asymptomatic former and current smokers. Therefore, EIT-derived reference values should only be collected from nonsmoking lung-healthy adults.
Abstract
EIT assesses the spatial and temporal distribution of lung function in adults without pulmonary disease, and detects its increased heterogeneity in former and current smokers compared with nonsmokers. EIT reference values should originate from nonsmokers. http://bit.ly/2wsJQWD
Introduction
Pulmonary disorders are associated with heterogeneity of ventilation distribution [1–4]. Pulmonary function testing (PFT) and imaging are frequently used for the assessment of lung impairment, most commonly spirometry, chest radiography and computed tomography (CT). Spirometry determines the global lung function derived from measurements at the airway opening. It is not able to assess the regional lung function. Radiography serves as an initial imaging examination for the rough detection of lung changes. CT provides the anatomical information on the lung structure and is able to present structural changes like atelectasis or bronchiectasis; however, both imaging modalities are associated with radiation exposure.
Electrical impedance tomography (EIT) is a functional imaging modality capable of detecting rapid air content changes as required by PFT [5]. Its use is new in pneumology [6, 7]. EIT assesses the regional lung function and is able to identify ventilation heterogeneities directly in the examined region of the chest in spontaneously breathing subjects [8, 9]. Because of its noninvasiveness, radiation-free measuring principle and easy bedside use, EIT can be applied at any age [10–15]. In order to correctly interpret the impairment of regional lung function and its development over time in patients with lung diseases, reference values of regional lung function parameters derived from a lung-healthy population are needed. No systematic large EIT data exist on regional lung function in lung-healthy adults. Therefore, we examined a population of asymptomatic lung-healthy adults using EIT. In order to verify whether subtle functional changes in ventilation distribution are detectable, we included three groups of subjects in our study population: nonsmokers and asymptomatic former and current smokers.
The goal of the study was the characterisation of the ventilation distribution in a lung-healthy, asymptomatic population and the determination of tobacco's influence on a regional level using EIT. The obtained results are intended to serve as reference values for patients with lung diseases.
Material and methods
The observational monocentric study was approved by the institutional ethics committee and informed written consent was obtained from each studied subject. Between August 2013 and October 2013, PFT using EIT was carried out in 219 lung-healthy subjects during a standardised forced vital capacity (FVC) manoeuvre [16] during an average of 90 s. A total of 36 subjects were excluded from further data analysis due to their inability to adequately perform the manoeuvre. From the remaining 183 subjects, a further 5 were excluded because of inadequate electrode contact, necessary for proper EIT scanning. The remaining 178 lung-healthy asymptomatic subjects consisted of 64 nonsmokers, 68 past smokers and 46 current smokers (figure 1). The examined patients also served as a study population in a separate examination regarding the preoperative pulmonary risk assessment using the new spirometric reference values of the worldwide Global Lung Initiative [17]. Nonsmokers were defined as subjects who did not smoke more than 50 cigarettes in their whole life, past smokers as subjects that managed to quit smoking for more than 6 months before the study and current smokers as subjects who were smoking up to the inclusion in the study. All subjects had no history of chronic obstructive pulmonary disease or other pulmonary diseases or any pulmonary symptoms. They did not use any pulmonary effective drugs. Not included in the study were subjects younger than 18 years and subjects having a contraindication to an FVC manoeuvre, such as cerebral aneurysm.
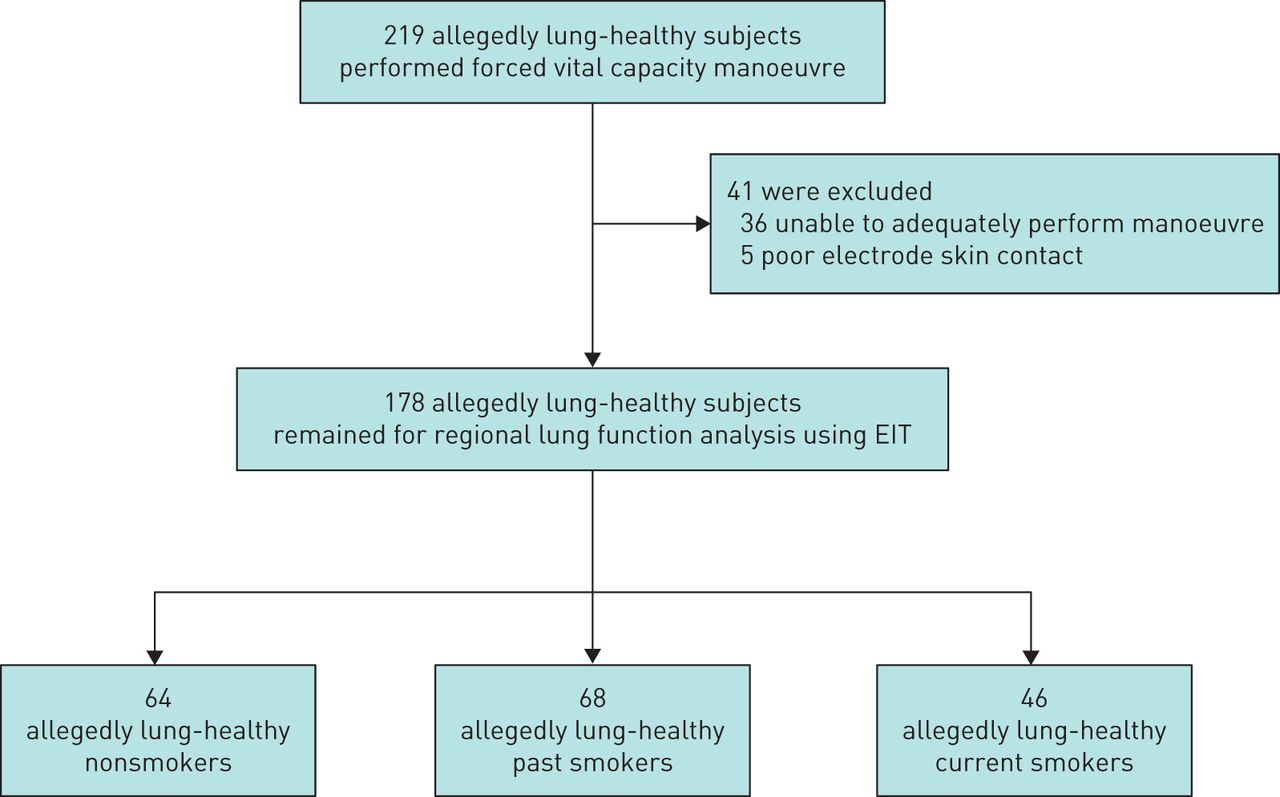
Enrolment and follow-up of the study participants. EIT: electrical impedance tomography.
A total of 16 electrodes (BlueSensor BR-50-K, Ambu, Ballerup, Denmark) were attached on the chest circumference at the 4–5th intercostal space for the EIT data collection and one reference electrode on the abdomen of each subject. All participants were studied in the sitting position using the Goe-MF II device (CareFusion, Höchberg, Germany) recording 33 images·s−1 during a conventional FVC manoeuvre consisting of full inspiration from residual volume to total lung capacity (TLC) with subsequent forced full expiration.
The EIT measuring principle is based on repetitive alternating current applications (5 mArms and 50 kHz) between 16 adjacent pairs of electrodes. During each current application over one adjacent electrode pair, 13 remaining passive adjacent electrode pairs measured the resulting voltages. A sequence of 2000 to 3300 raw EIT images (each consisting of 836 image pixels) was acquired in each study subject during the examination. The images were generated by the reconstruction algorithm GREIT [18]. They showed the differences between the instantaneous (Z) and reference pixel impedance (Zref) normalised by Zref ((Z-Zref)/Zref). Pixel Zref corresponded to the average pixel Z during the stable tidal breathing period at the beginning of the measurement before the forced manoeuvre. These values are given as “relative impedance change” (rel. ΔZ). The pixel EIT waveforms of rel. ΔZ in each of the image pixels were used for further analysis of regional lung volumes and expiratory times. For the detailed analysis of regional lung function, we identified the beginning and the end of the forced full expiration in every EIT waveform. Thereafter we calculated the following values in each EIT pixel: forced expiratory volume in 1 s (FEV1,EIT) as the difference between rel. ΔZ at TLC and after 1 s of forced expiration, FVC (FVCEIT) as the difference between rel. ΔZ at TLC and the end of forced expiration and the FEV1/FVCEIT ratio. In order to characterise the heterogeneity of ventilation distribution, we calculated the coefficient of variation (CV) from the 836 values of each EIT-derived lung function parameter. Furthermore, we generated histograms of the pixel values of FEV1/FVCEIT, presenting the spatial ventilation distribution in more detail. The temporal ventilation distribution was assessed by histograms of pixel expiratory times required to exhale 50% (t50), 75% (t75) and 90% (t90) of FVC.
Statistical analysis was carried out by GraphPad Prism version 5.01 (GraphPad Software, San Diego, CA, USA). The differences in all EIT-derived regional lung function parameters among the three studied groups were determined by one-way ANOVA with Bonferroni's multiple comparison post-test. A p-value <0.017 was considered significant.
Results
We analysed 64 nonsmokers, 68 past smokers and 46 currents smokers. The studied former smokers were older than current and nonsmokers and they showed lower smoking intensity (indicated by pack-years) than current smokers. The proportion of women compared with men was higher in nonsmokers than in the other two groups.
The physical characteristics of the study participants and the corresponding spirometric lung function values are given in table 1.
Study participants' characteristics.
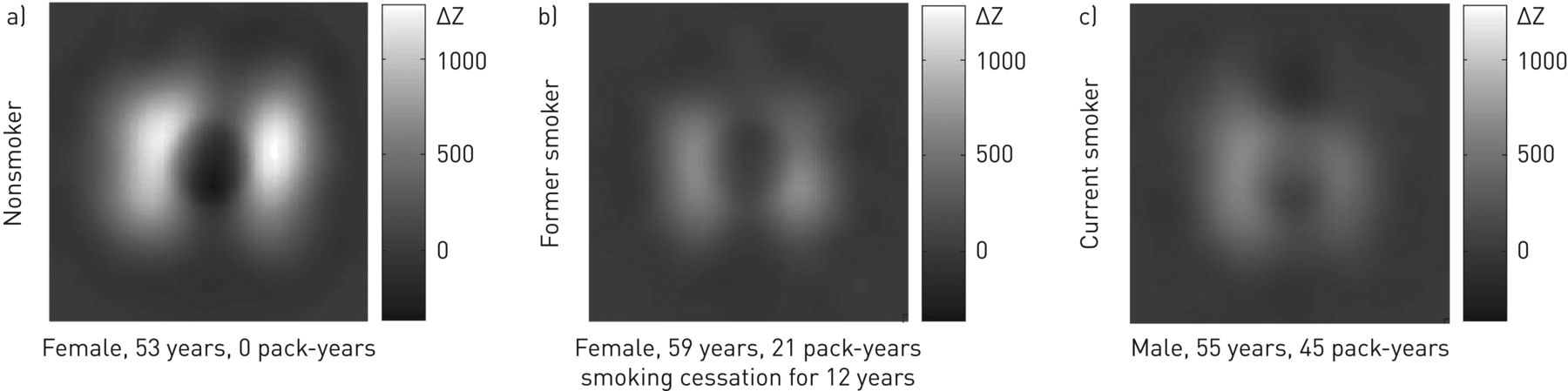
Subtle ventilation differences like reduced ventilation impedance signal variation or regional deficit in ventilation were already discernible in functional EIT images before the quantitative analysis of ventilation heterogeneity. Example images are given in figure 2 presenting functional EIT images obtained in three subjects during FVC: one nonsmoker, one former smoker and one current smoker.

Functional electrical impedance tomography images presenting the regional ventilation distribution during forced expiration corresponding to the forced vital capacity manoeuvre determined in the chest cross section of three lung-healthy asymptomatic adults: a) nonsmoker, b) former smoker and c) current smoker. ΔZ: relative impedance change.
The CV value of regional FEV1/FVCEIT was the highest in smokers followed by former smokers and nonsmokers. It distinguished among the three groups (p<0.0001) and indicated the most homogenous ventilation distribution in nonsmokers and the highest degree of ventilation heterogeneity in allegedly lung-healthy smokers. The CV of FEV1,EIT and FVCEIT did not show any significant differences among the three groups (figure 3).

Coefficients of variation (CVs) of electrical impedance tomography (EIT)-derived regional pulmonary function measures of a) forced expiratory volume in 1 s (FEV1), b) forced vital capacity (FVC) and c) FEV1/FVC determined in lung-healthy asymptomatic nonsmokers, and former and current smokers. The box and whiskers plots display the minimum, 25% percentile, median, 75% percentile and maximum values. The p-value in the right upper corner of each diagram shows the result of statistical testing using a one-way ANOVA. Significant differences among the individual groups assessed by the Bonferroni's multiple comparison test are indicated by asterisks. rel. ΔZ: relative impedance change. ***: p<0.0001.
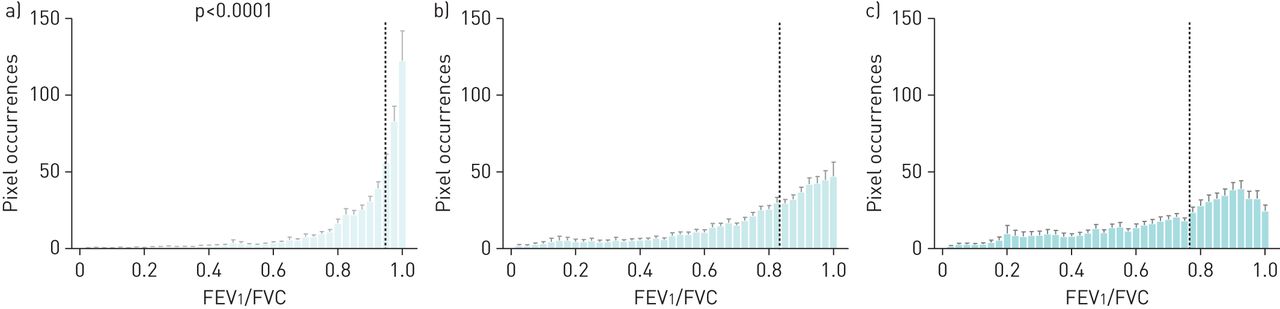
The frequency distributions of all pixel values of FEV1/FVCEIT presented as histograms highlighted the spatial ventilation heterogeneity (figure 4). In lung-healthy nonsmokers the values were higher with a rather narrow peak at higher values (figure 4a), whereas the former and current smokers showed flat distributions (figure 4b and c); in smokers the values were shifted towards left to lower values (figure 4c). Median of FEV1/FVCEIT distinguished between the lung-healthy nonsmokers (median: 0.97) and the other two groups (median past smokers: 0.87; median smokers: 0.84) (p <0.0001).

Frequency distributions of pixel values of the forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) ratio determined by electrical impedance tomography in studied lung-healthy asymptomatic a) nonsmokers, and b) former and c) current smokers. The histograms show mean+sem. The vertical dotted lines correspond to the mean of the median values of the respective histograms. The p-value shows the result of statistical testing using one-way ANOVA. Significant differences among the studied groups assessed by the Bonferroni's multiple comparison test are indicated by asterisks. ***: p<0.0001.
The temporal heterogeneity of ventilation distribution was shown by the frequency distributions of pixel t50, t75 and t90 presented as histograms (figure 5). Already in t50, there were significant differences between the median value of nonsmokers and the values of past and currents smokers (p=0.0003). The histograms of nonsmokers were characterised by the highest peak and a narrow base when compared with the other two study groups (figure 5a, d and g). The median of t75 also discriminated between nonsmokers and the subjects affected by smoking (p <0.0001). Past and current smokers showed a pixel shift towards higher values (to the right) with a more heterogeneous pixel values distribution pattern than the lung-healthy nonsmokers (figure 5b, e and h). The best discrimination among the groups offered the regional t90 values (figure 5c, f and i). The median values of t90 were the longest in smokers and the shortest in nonsmokers and this effect was highly significant (p <0.0001). The distribution of the pixel values of t90 reached the highest degree of ventilation heterogeneity when compared with t50 and t75.
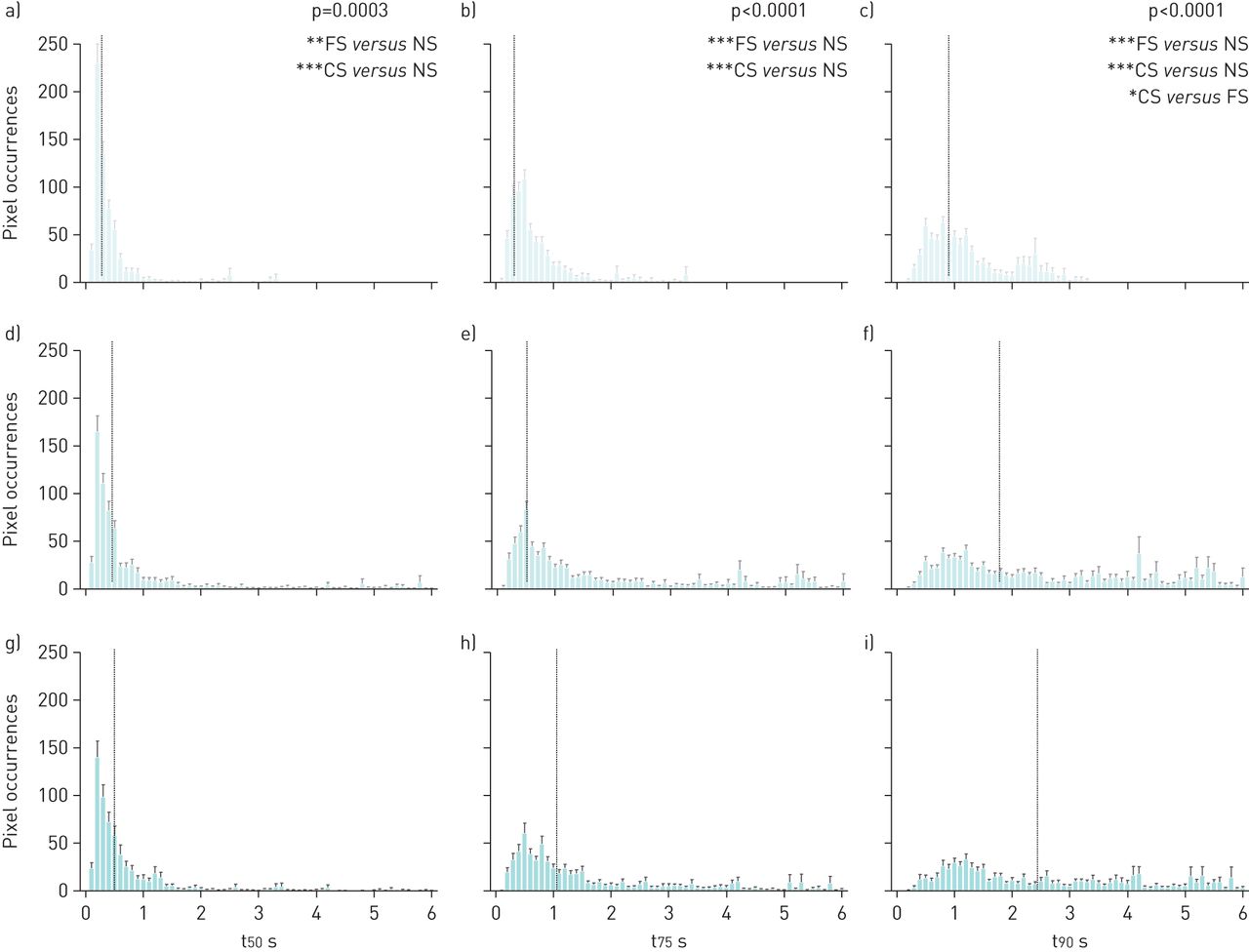
Frequency distributions of a, d and g) pixel times required to exhale 50% (t50) of regional forced vital capacities, b, e and h) pixel times required to exhale 75% (t75) of regional forced vital capacities and c, f and i) pixel times required to exhale 90% (t90) of regional forced vital capacities determined by electrical impedance tomography in lung-healthy asymptomatic a–c) nonsmokers (NS), d–f) former smokers (FS) and g–i) current smokers (CS). The histograms show mean values+sem. The vertical grey dotted lines correspond to the mean of the median values of the respective histograms. The p-values of t50, t75 and t90 median in the corresponding columns show the results of statistical testing using one-way ANOVA. Significant differences among the groups assessed by the Bonferronís multiple comparison test are indicated by asterisks. *: p<0.05; **: p<0.001; ***: p<0.0001.
The CV values of regional t50, t75 und t90 were able to equally differentiate between the heterogeneities of ventilation distribution in nonsmokers and both past and current smokers (p<0.0001). We did not find any differences between past and current smokers when the CV of regional expiration times was considered (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Coefficients of variation (CVs) of electrical impedance tomography (EIT)-derived regional a) pixel times required to exhale 50% (t50) of regional forced vital capacities, b) pixel times required to exhale 75% (t75) of regional forced vital capacities and c) pixel times required to exhale 90% (t90) of regional forced vital capacities determined in lung-healthy asymptomatic nonsmokers, former and current smokers. The box and whiskers plots display the minimum, 25% percentile, median, 75% percentile and maximum values. The p-value in the right upper corner of each diagram shows the result of statistical testing using a one-way ANOVA. Significant differences among the individual groups assessed by the Bonferroni's multiple comparison test are indicated by asterisks. rel. ΔZ: relative impedance change. ***: p<0.0001.
The corresponding values of the above-mentioned regional parameters of ventilation heterogeneity derived by EIT are given in table 2.
Values of electrical impedance tomography (EIT) variables in the three study groups.
Discussion
The results of our study showed that EIT-derived regional lung function parameters were able to assess the spatial and temporal ventilation distribution in lung-healthy subjects during a forced expiration manoeuvre. EIT was also able to detect the differences in ventilation heterogeneities on a regional level among lung-healthy nonsmokers and asymptomatic allegedly lung-healthy past and current smokers depending on tobacco consumption.
The CV of EIT-derived regional FEV1/FVCEIT exhibited the highest degree of ventilation heterogeneity in asymptomatic allegedly lung-healthy current smokers. The higher the CV in the examined chest section, the more heterogeneous was the ventilation distribution. The CV of FEV1/FVCEIT is a rather rough regional parameter of ventilation heterogeneity that was sensitive enough to detect the current and the past smoking effects in our study. The advantage of the CV of different regional lung function parameters (like FEV1,EIT, FVCEIT and FEV1/FVCEIT) is a single value that focuses on the overall degree of spatial ventilation distribution in the whole studied chest section [6]. This might be beneficial in the routine care for the first assessment of possible regional lung function impairment. The CV of t50, t75 and t90 only managed to distinguish the nonsmokers from the other two groups. The ventilation distribution was more homogeneous in nonsmokers than in both past and current smokers. The particular feature of EIT is its ability to assess the regional temporal differences in the regional forced expiration times. The frequency distributions of pixel values of t50, t75, and t90 revealed the ventilation distribution in a more detailed way than the CV of regional lung function parameters FEV1,EIT, FVCEIT and FEV1/FVCEIT. The histograms of regional forced expiration times with their characteristic silhouettes could serve as reference histogram shapes for further studies characterising the regional temporal ventilation distribution in subjects suffering from lung diseases like chronic obstructive pulmonary disease (COPD), asthma or pulmonary fibrosis. The medians of the frequency distributions of t90 distinguished among nonsmokers, allegedly lung-healthy past smokers and current smokers. The detected smoking influence in past and current smokers resulted in an approximately twice prolonged exhalation of the same volume as in nonsmokers, the medians of respective groups differed significantly, and the frequency distribution shifted to the right towards higher values.
The time-dependent functional information from PFT can be visualised by means of the regional lung function parameters t50, t75 and t90. This allows not only the detection of differences in ventilation distribution among several study groups, as shown in our current study, but also timely changes in ventilation distribution between two measuring times in one individual such as before and after exercise challenge or before and after administration of bronchodilators as already shown in small studies [10–12]. In one of the first studies on PFT and EIT we detected differences in spatial and temporal ventilation distribution between lung-healthy subjects and patients with COPD [6]. The present study did not include patients with COPD; however, it still confirmed that EIT is sensitive enough to detect the even smaller regional differences in regional ventilation distribution in nonsmokers compared with asymptomatic past and current smokers. These study groups are not as clinically (concerning the pulmonary conditions) different from each other as the lung-healthy subjects and patients with COPD in the former study.
EIT is a functional imaging modality; it does not aim to provide anatomical information [5]. This is highlighted in figure 2 where the reduction in relative impedance change and the ventilation defects are only slightly visible. The spatial resolution of EIT is low when compared with other imaging modalities like magnetic resonance imaging (MRI) or CT. Sheikh et al. showed ventilation defects in never-smokers with normal spirometry results using hyperpolarised 3He MRI [19]. Hamedani et al. used 3He MRI to prove that cigarette smoke induced pulmonary alterations that were not detectable by nonimaging clinical tests such as spirometry, plethysmography and the 6 min walk test (6MWT). They examined nonsmokers, asymptomatic smokers and patients with COPD and found no differences between nonsmokers and asymptomatic smokers when spirometry, plethysmography or 6MWT were applied [20]. Pike et al. were able to show very mild emphysema in ex-smokers without airway limitation by 3He MRI [21]. New developments in CT allow differentiating among specific COPD phenotypes [22]. The anatomical information, such as dimensions of airways delivered by CT, correlates with the severity of airway obstruction [23]. In comparison with MRI and CT, EIT can be used at the bedside or in the PFT lab with lower costs regarding staff, equipment and examination time. Despite smaller scan rates than conventional PFT dominated by spirometry and plethysmography, EIT delivered data at a scan rate of 33 images per second in the present study, in up to 836 regional values of a certain regional lung function parameter, such as FEV1,EIT in the examined thorax cross section. Conventional PFT provides only one value, such as global FEV1 measured at the airway opening [10, 24].
As expected, in this study the proportion of women in the nonsmokers group was higher than in past and current smokers. Aside from the age of the past smokers and smoking history the study groups did not differ from each other. In the previous EIT study examining the ventilation heterogeneities in young and elderly nonsmokers, there were no differences found when CV was used [6]. We suspect that the age in the studied age range between 47 and 55 years had less influence on the regional lung function than the smoking history.
The nonsmokers group had a 20% higher proportion of women than men compared with the other study groups. We did not find any significant differences in the determined parameters of ventilation heterogeneity between men and women in the three study groups. That is why we assume that the higher number of women than men was not the cause of more homogenous ventilation distribution in the nonsmoking study participants. However, studies on much higher number of subjects are needed to prove conclusively that sex does not affect the heterogeneity of ventilation distribution. In addition, other parameters may be needed to separately assess any possible effect of sex.
In order to adequately interpret changes in regional ventilation distribution in patients with pulmonary diseases, we need data from lung-healthy subjects and knowledge about its meaning. The basic research on heterogeneity of ventilation distribution during spontaneous breathing by EIT is new in the field of pneumology and must be systematically examined, as stated in the recent consensus statement on chest EIT [5]. The current study presents the first steps in this direction. The need for reference values in PFT has increased in recent years, as initially shown by Quanjer et al. for spirometry [25]. For years, reference values were used with a fixed FEV1/FVC ratio <0.7 for the detection of airway obstruction [26]. In 2012 the Global Lung Initiative introduced new spirometric reference values collected on 98 000 healthy nonsmokers [25] that allowed more correct and personalised diagnostics of pulmonary function.
The present study was carried out in spontaneously breathing lung-healthy subjects, but the long-term goal is to establish EIT as a diagnostic and monitoring method in patients with chronic lung diseases. EIT has the potential for this use not only in the clinical hospital and outpatient settings but also in the preclinical home environment. Wearable EIT systems are being developed that might facilitate this application of EIT in the future [27]. Even with the currently available technology, the EIT examinations are not time-consuming. The attachment of electrodes is the most extensive work, whereby it takes less than 5 min for experienced personnel and this time can further be reduced if electrode belts are used. The duration of EIT data acquisition is based on the needs defined by the medical question. If EIT data are recorded only during the FVC manoeuvre then the EIT measurement takes just as long as when conventional spirometry is used, usually about 90 s. During continuous patient examinations data collection over hours is possible.
Our study generated reference values of several regional EIT lung function parameters. The examinations were performed in parallel with conventional PFT (such as the FVC manoeuvre). This approach was chosen as it may facilitate the attempted establishment of EIT in the field of pneumology because the same well-known lung function parameters are determined by EIT as by spirometry, only on a regional level. However, additional new measures could be calculated (t50, t75 and t90) from EIT recordings in our study capable of characterising the heterogeneity of regional lung function. We suppose that further lung function measurements specifically designed for EIT use will be developed in the future. They should be easily carried out by patients and independent of their cooperation.
The number of our study participants is limited when compared with the mentioned large studies on conventional PFT. However, this study is the largest one ever carried out in adults for the determination of regional lung function by EIT worldwide to the best of our knowledge. The majority of the existing EIT studies on ventilation distribution focus on mechanically ventilated intensive care patients [14, 28–30]. We believe that EIT chest examinations may be beneficial in spontaneously breathing patients with pulmonary diseases like COPD, [6, 31] asthma [12, 13, 32] or cystic fibrosis [11, 33, 34] as well and that this new functional method has a potential in pneumology.
The EIT impedance changes correlate strictly with spirometric data during the forced expiration manoeuvre [35]. Therefore, EIT can be used as a diagnostic tool providing the information about the regional pulmonary function in addition to the global one determined by conventional PFT. The new gained knowledge about the regional lung function might enable comprehensive individualised medicine.
Our study has some limitations that we wish to address. EIT measurements were carried out with the electrodes placed on the chest circumference in one plane. When EIT electrodes are located between the 4th and the 6th intercostal space, the apical lung regions and the areas close to diaphragm are not accessible to EIT examination. The optimal solution would be the simultaneous examination in multiple levels. To date, there are no devices available that would make this possible. Efforts exist to develop such technology [36] but the corresponding data acquisition and simultaneous processing at multiple levels are currently still difficult and not yet established.
We used single electrodes instead of EIT belts for data collection in our study. At first sight this might seem disadvantageous but, according to our experience, the EIT belts sometimes lose skin contact during the FVC manoeuvre due to the very quick decrease in the thoracic cross section. For each EIT measurement, the skin electrode contact and electrode location for current injection and detection of voltage changes should ideally not change with time. That is why we decided to use the single electrodes instead of EIT belts, although the belts are more frequently used in adults, especially in mechanically ventilated lying patients.
Another limitation of this study is the lower proportion of smokers than past smokers and nonsmokers. Most smokers develop pulmonary complaints over time and they become symptomatic. We selected current smokers that were still asymptomatic and that did not yet receive the diagnosis of COPD. The recruitment at this stage is difficult because asymptomatic smokers have no reason to undergo medical consultation and treatment.
Our results support the hypothesis that only EIT-derived regional lung function parameters originating from lung-healthy nonsmokers should serve as reference values for regional ventilation distribution for patients with lung diseases. Smoking impacts the ventilation distribution patterns during forced expiration manoeuvre rendering them not compatible with values of homogeneous ventilation distribution observed in nonsmokers.
Conclusions
The results of our study highlight the potential of EIT as an additional tool in PFT for detecting regional ventilation distribution and its heterogeneity. In this study, we established the first EIT-derived regional lung function values for lung-healthy adults. Furthermore, we showed the impact of tobacco consumption on regional lung function. The regional EIT parameters might enable the discrimination between lung-healthy subjects and patients affected by lung diseases. The regional lung function results determined in patients should only be compared with results originating from nonsmoking lung-healthy reference population when EIT is used.
Footnotes
Conflict of interest: B. Vogt reports grants from the European Commission outside the submitted work.
Conflict of interest: K. Deuß has nothing to disclose.
Conflict of interest: V. Hennig has nothing to disclose.
Conflict of interest: Z. Zhao reports a consulting fee from Dräger Medical AG outside the submitted work.
Conflict of interest: I. Lautenschläger has nothing to disclose.
Conflict of interest: N. Weiler has nothing to disclose.
Conflict of interest: I. Frerichs report grants from the European Commission, and a speaking fee and reimbursement for travel costs from Dräger, outside the submitted work.
- Received December 10, 2018.
- Accepted May 1, 2019.
- Copyright ©ERS 2019
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










