





Abstract
Question addressed by the study Endogenous opioids (endorphins) have been reported to modulate exercise-induced breathlessness, but the relative contribution of peripheral opioid receptors has not been tested.
Materials, participants and methods This was a double-blind, randomised, three-arm, cross-over trial in outpatients with spirometry-verified moderate to severe chronic obstructive pulmonary disease. Participants undertook an incremental symptom-limited treadmill test followed by five endurance treadmill tests at 75% of their maximal work rate; two tests for familiarisation and three tests 30 min after intravenous injection of either methylnaltrexone 0.3 mg·kg−1 (blocking peripheral opioid receptors only) or naloxone 0.1 mg·kg−1 (blocking both central and peripheral opioid receptors) or normal saline, in randomised order. The primary end-point was the regression slope between breathlessness intensity (0–10 numerical rating scale) and oxygen consumption (V′O2) during the walk tests, comparing methylnaltrexone and placebo using a paired t-test.
Results 17 participants completed the trial: median (range) 66 (55–82) years; 15 males; mean±sd forced expiratory volume (FEV1) 53.8±17.6% predicted; FEV1/forced vital capacity ratio 0.55±15.9. There was no statistically or clinically significant difference in the primary end-point (regression slope of breathlessness intensity and V′O2) for methylnaltrexone (p=0.498) or naloxone (p=0.804), compared to placebo. Secondary outcomes were similar between the three treatment groups, including peak and mean breathlessness intensity and unpleasantness, exercise capacity, endurance time and leg fatigue.
Answer to the question Blocking peripheral opioid receptors (methylnaltrexone) or peripheral and central opioid receptors (naloxone) did not appear to modulate breathlessness intensity nor exercise capacity when compared with placebo (no blockade).
Abstract
A double-blind, placebo controlled, randomised, cross-over study using methylnaltrexone found no evidence for a contribution of peripheral opioid receptors to the modulation of breathlessness by endogenous endorphins. http://bit.ly/32DZv3I
Introduction
Chronic breathlessness [1] is a major cause of suffering and in people with chronic obstructive pulmonary disease (COPD) may lead to a vicious circle of reduced physical capacity and activity in order to avoid worsening breathlessness, deconditioning and further worsening respiratory distress [2, 3].
Opioids have been shown to decrease chronic breathlessness in COPD [4, 5]. Endogenous opioids (endorphins) increase in the blood during exertion and have been reported to modulate exercise-induced breathlessness both in healthy volunteers and in people with COPD [6–8]. In a double-blind, randomised, cross-over trial of 17 people with COPD by Mahler et al. [7], intravenous naloxone (blocking central and peripheral opioid receptors [9]) resulted in increased breathlessness during a treadmill walk test.
It is not known whether, and to what extent, endogenous opioids modulate breathlessness through central or peripheral opioid receptors. Central nervous system (CNS) sites that may modulate breathlessness through opioid-related pathways include the anterior cingulate cortex, amygdala, thalamus and even the brainstem [10]. Peripheral target receptors include on peripheral afferent nerves in the lungs, chest wall and other sites outside the CNS. No study has tested the effect of blocking only peripheral opioid receptors during exertion.
Methylnaltrexone is an opioid receptor antagonist that blocks only peripheral opioid receptors, as it does not cross the blood–brain barrier [9]. Methylnaltrexone is registered to treat opioid-induced constipation. Naloxone and methylnaltrexone offer the opportunity to for the first time test the contribution of peripheral opioid receptors (methylnaltrexone versus placebo) with central opioid receptors (naloxone versus methylnaltrexone) to exertional breathlessness in people with background chronic breathlessness [1]. This is important as clinical studies are being conducted into the use of nebulised morphine that specifically seeks to avoid systemic absorption (to reduce peripheral adverse effects including constipation) and provide a peripheral effect only.
The primary aim of this study was to isolate the role of peripheral opioid receptors in modulating exertional breathlessness in people with moderate or severe chronic obstructive pulmonary disease.
Methods
Study design and setting
This was a double-blind, triple-arm, cross-over, randomised controlled trial (RCT) of patients with COPD recruited from respiratory and palliative care outpatient clinics at the Repatriation General Hospital (Adelaide, South Australia). Each participant provided written informed consent. The study was approved by the appropriate human research ethics committee. The trial was prospectively registered (ACTRN12611001182987). This study is reported in compliance with the CONSORT (Consolidated Standards of Reporting Trials) guidelines for reporting RCTs [11].
Study population
Inclusion criteria (all required) were age ≥50 years; physician-diagnosed COPD with spirometry-verified forced expired volume in 1 s (FEV1)/forced vital capacity ratio <0.7 and a FEV1 of 30–80% predicted [12]; >10 pack-years of smoking; stable medications for breathlessness over the prior 1 week except routine “as-needed” medications; and the ability to use a treadmill.
Exclusion criteria were treatment with regular or as-needed opioids in the week before commencing the study and at any time during the study; adverse reaction to any of the study medications; cognitive impairment defined as a Mini Mental State score <24 [13]; calculated creatinine clearance ≤30 mL·min−1 [14]; body mass index (BMI) >35 kg·m−2; known or suspected bowel obstruction or gastrointestinal lesion; pulmonary rehabilitation ongoing or completed in the past 6 weeks; participants with a treadmill endurance time >25 min during the training phase (visits 2 or 3); and a history of myocardial infarction, unstable cardiovascular disease or other contraindication to exercise testing. A complete list of exclusion criteria is presented in supplementary appendix S1.
Intervention
The study comprised six treadmill tests for each participant. Before each test, participants self-administered four inhalations (i.e. total 400 μg) of albuterol/salbutamol using a metered-dose inhaler with a valved holding chamber. First, the maximal work rate was determined using a symptom-limited maximal incremental treadmill test. The subsequent five tests were endurance treadmill tests conducted at 75% of each participant's achieved maximal work rate using the modified Balke protocol [15, 16]. The exercise test consisted of a warm-up phase of ∼2 min, a symptom limited constant rate exercise phase at 75% of the participant's maximum work load, and a recovery phase of up to 15 min after exercise ceased. Two tests were performed for familiarisation and optimised reproducibility. Three intervention tests were then performed, each preceded by a double-blind i.v. injection of the agent to which they were randomised for that test 30 min before commencing on the treadmill. Interventions were naloxone 0.1 mg·kg−1 (10 mg maximum), methylnaltrexone 0.3 mg·kg−1 (30 mg maximum) and isotonic saline (placebo), with each injection diluted to 10 mL.
Each treadmill test was separated by ≥1 week (all conducted within an 8-week time frame for each participant) and the tests were conducted in the same half of the day (morning or afternoon) for each participant. Endurance treadmill exercise testing was chosen to replicate Mahler et al.'s model [7].
Assessments
Data on measured height, weight, functional status using the Australia-modified Karnofsky Performance Scale [17] and Charlson Comorbidity Index were obtained at baseline [18]. Spirometry was performed after bronchodilator administration at screening and before each intervention test using an EasyOne spirometer (Medical Technologies; Andover, MA, USA) and real-time exercise measures were performed initially on a CosMed Quark (CosMed, Rome, Italy) and later on an Oxycon mobile device (Jaeger, Carefusion, Höchberg, Germany). Predicted normal spirometry values were calculated using the NHANES III reference equations [19].
Outcomes
The primary outcome was breathlessness intensity measured at 1-min intervals on 0–100-mm visual analogue scale on an iPad (Apple, Cupertino, CA, USA) which converted responses to 0.5 cm numerical rating scale (NRS 0 “no breathlessness” and 10 “worst possible breathlessness”) [20–22]. Secondary outcomes included breathlessness unpleasantness recorded in a similar manner (0–10 NRS; 0 “not at all unpleasant” and 10 “the most unpleasant breathlessness I have ever felt”); peak breathlessness intensity and unpleasantness from study start to 15 min after completing the study; mean breathlessness intensity and unpleasantness during the exercise phase, and during the recovery phase, oxygen consumption (V′O2;; mL·min−1·kg−1); carbon dioxide production (V′CO2; mL·min−1·kg−1); minute ventilation (V′E; L·min−1); exercise endurance time; pulse oximetry; leg fatigue (0–10 NRS; 0 “none” and 100 “worst possible”); reason for stopping the exercise test (leg fatigue, breathlessness or both); time to return to baseline breathlessness intensity after exercise ceases; and participant-blinded report of the worst study treatment symptomatically at the end of the test.
Randomisation
Participants were randomised to the order in which the double-blind medication (methylnaltrexone; placebo; naloxone) was administered. Randomisation was generated from a random number generator. The schedule was provided to pharmacy in individual envelopes where medications were prepared by staff who had no other involvement in the clinical study. Consent and randomisation notification were carried out by trial nurses after referral from the medical team. All staff with direct participant contact were blinded to the order of allocation.
Statistical analyses
The outcome variables were tabulated for each treatment, and for pairwise treatment differences using descriptive statistics between baseline and peaks or the end of the test. Continuous variables were compared between groups using random effects cross-over models and paired t-tests.
The population included in the analysis was participants who provided informed consent, were randomised to a treatment sequence and who received at least one dose of study treatment. All analyses were performed according to the received treatment. No data were imputed.
The primary efficacy end-point was the difference between methylnaltrexone and placebo in the regression slope between the breathlessness intensity and oxygen consumption (V′O2) during the exercise phase of the treadmill test. A random effects model for cross-over designs was used to examine the overall treatment effect across the three treatment groups in outcome regression slopes, peak values and mean values during the exercise phase, and mean values during the recovery phase. Paired t-tests were used to examine differences between pairwise treatment groups, if the overall treatment effect was statistically significant.
Time to return to baseline breathlessness after exercise ceased was analysed using Kaplan–Meier time-to-event analysis. Patients were censored at the time of their last breathlessness measurement if they did not return to baseline breathlessness.
As there was only one primary end-point, adjustment for multiple comparisons was not performed and a two-tailed p-value <0.05 was considered statistically significant for the primary outcome. For the secondary pairwise comparisons (naloxone versus placebo and naloxone versus methylnaltrexone) and the pairwise comparisons of all end-points except the primary end-point, the overall Type I error rate was controlled at 5% using the closed global test procedure. First, the global test of association between treatment group and the end-point was assessed at the 5% significance level using the p-value from a random effects model for cross-over designs. Only if the global test of association was significant, the secondary pairwise treatment comparisons were tested at the 5% significance level using paired t-tests.
A sample size of 17 patients completing all tests was estimated to provide 80% power to detect a clinically significant difference in the primary outcome with α=0.05, based on the previous study by Mahler et al. [7].
Results
Out of a total 21 participants who entered the first exercise test between March 2012 and June, 2016, 17 participants were randomised and completed the protocol and all their available data were included in this analysis with three missing intervention walk tests (one on naloxone and two on placebo); median (range) age 66 (55–82) years; 15 were male; median (range) modified Medical Research Council (mMRC) 1 (0–3) [23]; median (range) BMI 24.1 (18.0–36.8) kg·m−2; and Charlson Comorbidity Index median (range) score 1 (1–3) (table 1). Respiratory function tests at baseline included FEV1 median (range) 1.87 (0.88–3.08) L, which equated to 57% pred (29–82% pred).
Characteristics before each randomised intervention treadmill test in 17 patients with moderate to severe chronic obstructive pulmonary disease
The exercise endurance time was similar for methylnaltrexone, naloxone and placebo (p=0.79; table 2). V′O2 and V′E were similar between the intervention groups throughout the duration of the walk tests (figure 1).
Parameters during the treadmill exercise tests

Values of a) oxygen consumption (V′O2) and b) minute ventilation (V′E) for methylnaltrexone, naloxone and placebo during endurance treadmill walk tests.
Primary end-point: breathlessness intensity
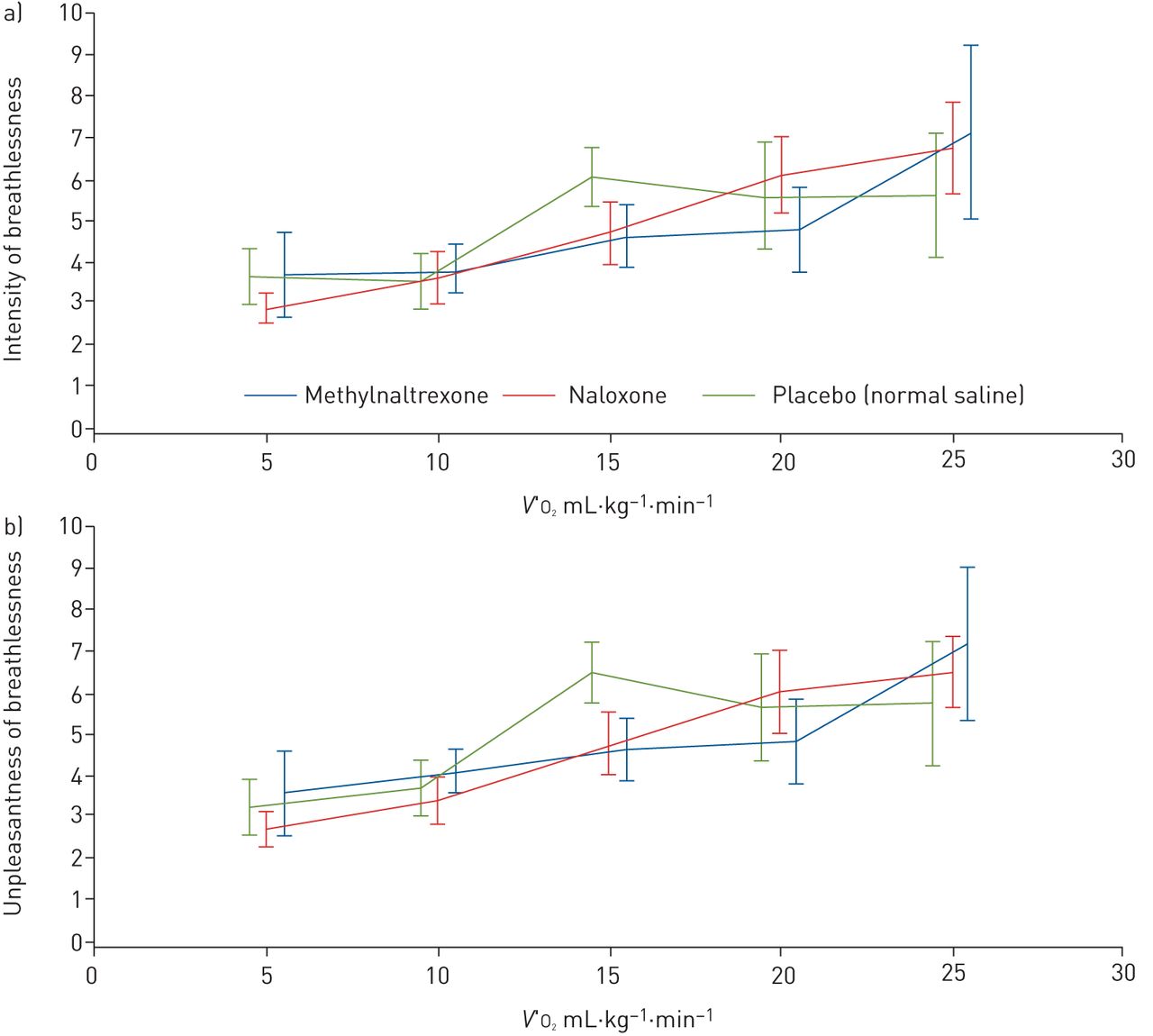
The slope of breathlessness intensity by oxygen consumption was similar between the three intervention groups (p=0.791; figure 2a). Breathlessness was similar throughout levels of standardised exercise (V′O2) between groups. For all intervention groups, participants exerted themselves up to similar maximal end-test breathlessness intensity (p=0.339) and unpleasantness (p=0.630; table 2). Individual differences in mean ratings of breathlessness intensity varied between participants, but with eight participants close to zero (figure 3).
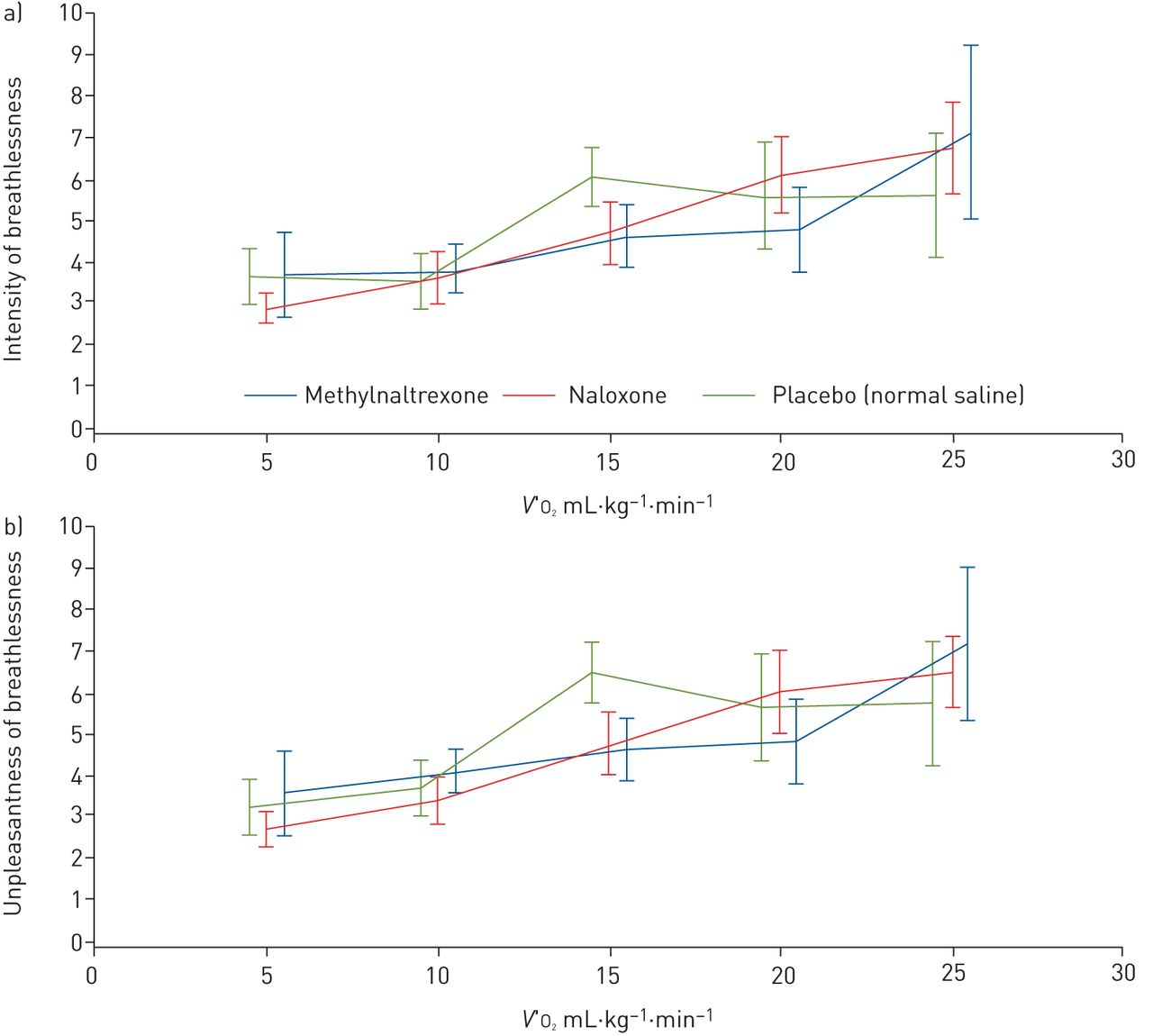
a) Intensity of breathlessness and b) unpleasantness of breathlessness by work rate (V′O2).

{kind=link}
{kind=link}
{kind=link}
Individual differences in mean breathlessness intensity between methylnaltrexone and placebo during endurance treadmill testing.
During recovery, there were no statistically significant differences between any of the interventions for breathlessness intensity (p=0.309) or breathlessness unpleasantness (p=0.375). For methylnaltrexone and placebo, the mean differences in breathlessness intensity and unpleasantness were small (mean difference intensity 0.57, 95% CI −1.03–2.16; p=0.58; mean difference unpleasantness 0.37, 95% CI −1.20–1.93; p=0.72). Median recovery time for breathlessness intensity was 0.8 (95% CI 0.3–0.9) min for normal saline, 0.9 (95% CI 0.5–1.2) min for methylnaltrexone and 1.2 (95% CI 0.5–4.2) min for naloxone. The probability of not recovering (breathlessness intensity) by 1 min was 37.5% and 35.3% for methylnaltrexone and placebo respectively, compared to 57.1% for naloxone.
Secondary outcomes
Secondary outcomes were similar between the intervention groups, including slopes of breathlessness unpleasantness (figure 2b), maximal exercise capacity (peak V′O2), minute ventilation, V′CO2, exercise endurance time and leg fatigue (table 2). At the end of the last intervention test, participants' blinded report of the intervention test with the worst breathlessness was similar between methylnaltrexone (n=3), naloxone (n=6) and placebo (n=6).
One participant had an episode of lightheadedness at the time of injection. This settled with being supine for a few minutes and the study proceeded without any problems.
Discussion
Using an i.v. bolus of methylnaltrexone to try and isolate the net effects of peripheral opioid receptors on the modulation of exercise-induced breathlessness in people with moderate to severe COPD and a background of chronic breathlessness, we found no difference from the uninhibited endogenous response (normal saline), suggesting that there is little peripheral modulation. Using a similar exercise protocol to Mahler et al. [7], we could not replicate previous findings that naloxone (blocked central and peripheral opioid receptors) worsened exertional breathlessness during treadmill walking in patients with COPD and chronic breathlessness. There was no evidence for effect of blocking either peripheral or central opioid receptors. Secondary outcomes were similar between the groups including peak exercise capacity, endurance, V′E, mean breathlessness intensity and unpleasantness and leg fatigue.
Importantly, the lack of effect of naloxone on exertional breathlessness seen in this study does not imply that exogenous opioids may be ineffective for alleviating chronic breathlessness. The lack of effect in the present study may relate to insufficient levels of endorphins provoked by the treadmill exercise.
One of these current findings concurs with a previous systematic review that found no evidence that exogenous opioids improve exercise tolerance [4], although one more recent study of morphine suggests a positive effect on the intensity of breathlessness and on the endurance time during a cycle test [24].
Limitations
It is unclear what the dosing of i.v. methylnaltrexone should be in these circumstances, nor the timing of its administration. These parameters were based on the best available evidence at the time of designing the study [9]. Subcutaneous methylnaltrexone bromide is a commercially available opioid antagonist and is used for the symptomatic treatment of opioid-induced constipation is administered at a dose of 0.15 mg–0.3 mg·kg−1, reflecting the doses used in this study [25]. Time to maximum concentration is 30 min (range 15–45 min), which was the time after the injection that the treadmill exercise commenced in this present study.
The study could not replicate the findings of Mahler et al. [7]; the lack of any signal from a contribution of peripheral opioid receptors should be treated with caution. The population in the study by Mahler et al. had more severe breathlessness and were able to tolerate the treadmill for a shorter period of time. This raises the possibility of a Type II error in the current study: it may be under-powered because people enrolled had greater exercise tolerance than the Mahler et al. article, on which the power calculation was based. Even in people with similar pathophysiology, the sensation of breathlessness may theoretically respond differently to endorphins. Even during exercise, the characteristics of breathlessness theoretically may also change in their response to opioids.
mMRC was patient-rated in the current study, rather than by a pulmonologist who knew the patients well, as in the study by Mahler et al. In recent work, it appears that patients will systematically underestimate their level on the mMRC breathlessness scale when compared to contemporaneous clinician rating [26].
Research implications
Developing robust and reproducible in vivo models that allow evaluation of interventions for exercise-induced acute breathlessness that is superimposed on chronic breathlessness is an urgent need given the suffering generated on a daily basis around the world. Given recent evidence of potential benefit from opioids in exercise induced acute-on-chronic breathlessness being differentially of benefit to people with COPD whose exercise capacity was limited because of breathlessness (rather than leg fatigue), this may help to define a target subpopulation in future work [21]. Both endurance and breathlessness were greater in this group in the morphine cross-over study conducted by Abdallah et al. [24], while in the current study, half the participants were limited in their exercise by leg fatigue, not breathlessness.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00153-2019.supplement
Acknowledgements
Our thanks go to all the people who participated in this difficult study. Their time and dedication are appreciated.
Footnotes
This article has supplementary material available from openres.ersjournals.com
This study is registered at www.anzctr.org.au with identifier number ACTRN12611001182987. Data are available on request from bona fide researchers.
Support statement: Funding was provided for the study by the National Health and Medical Research Council (Australia) grant 1065572. The funder had no control over study design, conduct, analysis, interpretation or dissemination of results. M. Ekström was supported by an unrestricted grant from the Swedish Heart-Lung Foundation and the Swedish Society for Medical Research. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: D.C. Currow is an unpaid member of an advisory board for Helsinn Pharmaceuticals, is a consultant to Specialised Therapeutics and Mayne Pharma, and received intellectual property payments from Mayne Pharma.
Conflict of interest: T. Hunt reports paid employment independent of this work for Boehringer Ingelheim and Janssen-Cilag Pty Ltd.
Conflict of interest: S. Louw reports statistical consulting fees from McCloud Consulting Group during the conduct of the study.
Conflict of interest: D. Eckert reports research grants from and advisory board membership for Apnimed (a pharmaceutical company established to develop drug therapy for sleep apnoea), a research grant from and consultancy (sleep apnoea area) for Bayer, and a Cooperative Research Centre (CRC)-P grant, a collaboration between the Australian Government, academia and industry (industry partner Oventus Medical), outside the submitted work.
Conflict of interest: P. Allcroft has nothing to disclose.
Conflict of interest: T.H.M. To has nothing to disclose.
Conflict of interest: A. Greene has nothing to disclose.
Conflict of interest: M. Krajnik reports that she is the head (unpaid) of a foundation supported financially in its educational activities by Angellini, Stada, Takeda and Molteni, outside the submitted work.
Conflict of interest: D. Mahler has nothing to disclose.
Conflict of interest: M. Ekström has nothing to disclose.
- Received August 15, 2019.
- Accepted October 17, 2019.
- Copyright ©ERS 2019
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










