





Figures
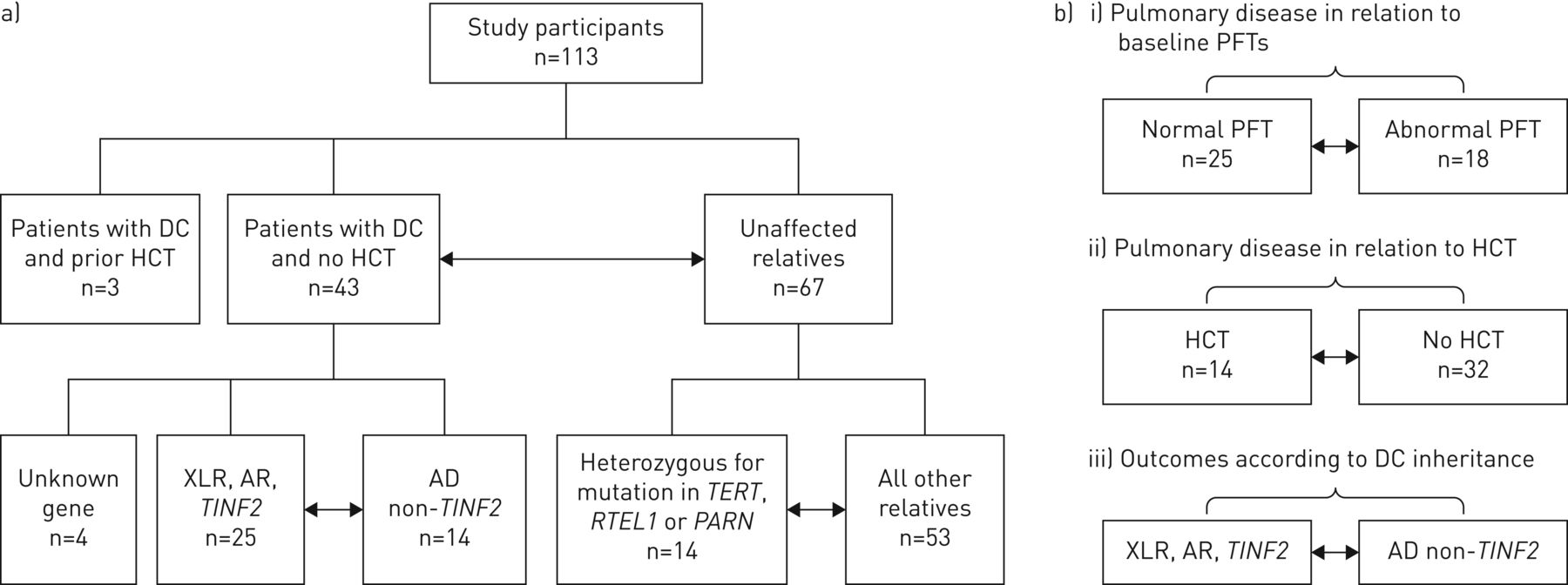
- FIGURE 1
Study schema indicating the comparison groups. a) Analyses of pulmonary function tests (PFTs) and groups. b) Analyses of patient outcomes in relation to PFT. DC: dyskeratosis congenita; HCT: haematopoietic cell transplantation; XLR: X-linked recessive; AR: autosomal recessive; AD: autosomal dominant.
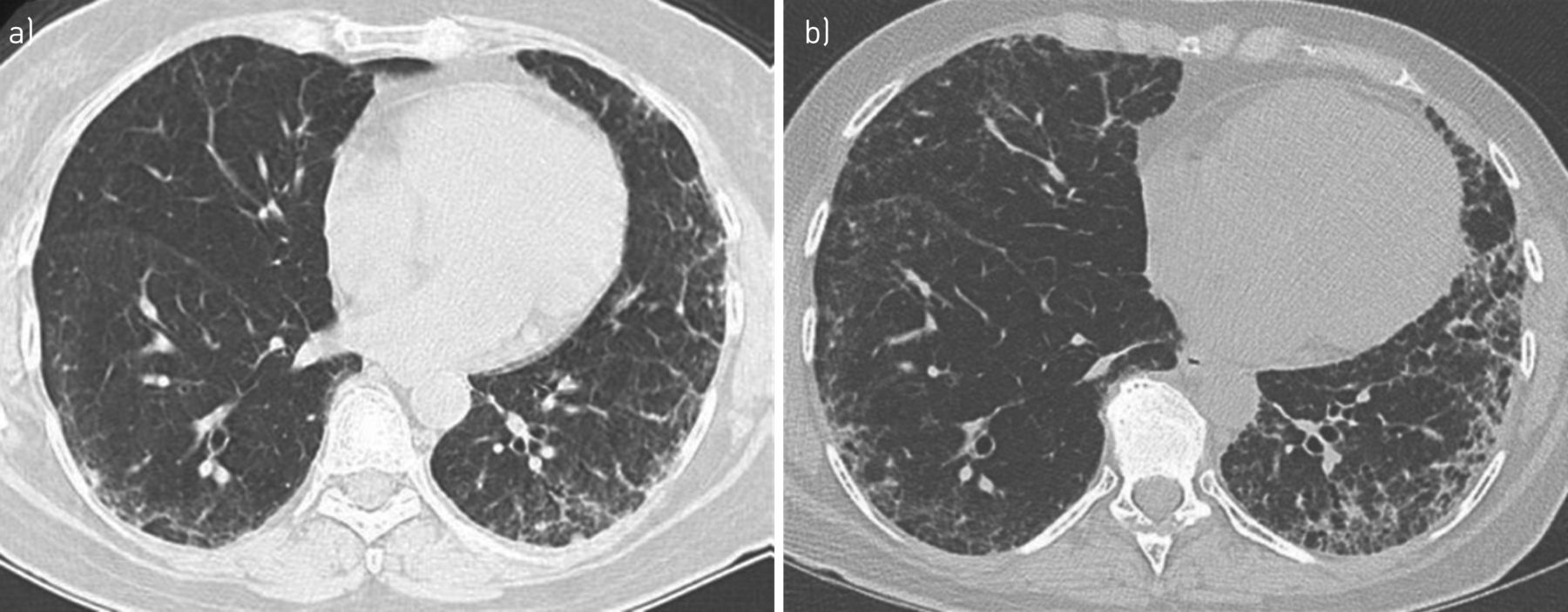
- FIGURE 2
High-resolution computed tomography (CT) scan of the lungs (patient NCI-6-1). a) Peripheral interstitial and ground-glass opacities with early honeycombing in bases bilaterally consistent with usual interstitial pneumonia pattern of pulmonary fibrosis in a 54-year-old female with heterozygous TERC mutation and symptoms of dyspnoea on exertion, impaired flows and diffusion with diffusing capacity of the lung for carbon monoxide (DLCO) 57% of predicted. b) The patient's symptoms had progressed 3 years later with dry cough, progressive dyspnoea, basal crackles and desaturation to 85% on 6-minute walk test; restrictive ventilatory defect and DLCO at 50%. The CT scan shows an increase in peripheral subpleural fibrosis. The advanced fibrosis in the left lung is also slightly worsened.
- FIGURE 3
Cumulative incidence of pulmonary disease in patients with normal versus abnormal baseline pulmonary function tests (PFTs). The graph starts at the age at PFT and ends at the diagnosis of pulmonary disease, death or last follow-up. The three patients with incident pulmonary disease at the time of baseline PFT were excluded from the graph. The blue line indicates patients with abnormal baseline PFTs (n=15; five patients developed pulmonary disease 2–7 years after the PFTs). The yellow dashed line depicts patients with normal baseline PFT (n=25; two patients were diagnosed with symptomatic pulmonary disease at 2 and 10 years after the baseline PFTs). The cumulative incidence of pulmonary disease by age 20 years was 55% (95% CI 28–100%) in patients with abnormal baseline PFT versus 17% (95% CI 3–100%) in those with normal PFTs (overall p=0.02).
- FIGURE 4
Competing risk of adverse events including pulmonary disease, haematopoietic cell transplantation (HCT), and death. a) autosomal recessive/X-linked recessive and TINF2 dyskeratosis congenita (DC). The first event was HCT for severe bone marrow failure in 12 patients (grey line) with a cumulative incidence of 50% (95% CI 33–77%) by age 30 years; two patients died at age 19 and 37 years from other causes (yellow line) and one developed pulmonary fibrosis plus pulmonary arteriovenous malformations at age 20 years (blue line). b) autosomal dominant non-TINF2 DC. In all, one patient received HCT, whereas four patients developed pulmonary fibrosis with a cumulative incidence of 70% (95% CI 39–100%) by age 60 years among non-HCT patients.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Characteristics of study participants
Patients with DC Unaffected relatives Patients versus relatives p-value All XLR, AR, TINF2# AD non-TINF2# p-value All Carriers of RTEL1, TERT or PARN All others Participants 43 25 14 67 14 53 Age at diagnosis years 13 (1–65) 11 (1–43) 32 (12–65) <0.0001 Age at study years 21 (6–69) 18 (6–42) 35 (12–69) 0.002 46 (10–60) 46 (10–60) 36 (7–64) 0.0001 Male/female 31/12 21/4 7/7 0.03 25/42 6/8 19/34 0.001 Smoker 7 (15%) 3 4 0.2 10 (15%) 3 (21%) 7 (13%) 0.8 Ethnicity Caucasian 40 24 12 63 14 49 0.7 African 2 1 1 0 0 0 Hispanic 0 0 0 1 0 1 Asian 1 0 1 3 0 3 Microcephaly 11 11 0 0.003 0 0 0 HH/RS 8 8 0 0.03 0 0 0 DC triad features¶ 0–1 20 8 11 0.008 63 14 53 ≥2 23 17 3 0 0 0 Bone marrow failure+ None 12 7 5 0.2 0 0 0 Moderate 13 4 5 Severe 18 14 4 Telomere length Z-score −3.9 −4.5 (−1.3– −6.7) −3.1 (−1.1– −5.5) 0.0007 −0.9 (−1.8– −4.2) −1.9 (−0.3– −1.9) −0.7 (−0.7– −4.2) <10-9 DC gene (inheritance) DKC1 (XLR) 7 7 0 7 0 7 RTEL1 (AR or AD) 7 6 1 8 8 0 PARN (AR) 3 3 0 5 5 0 WRAP53 (AR) 0 0 0 3 0 3 ACD (AR) 0 0 0 2 0 2 TERT (AR or AD) 6 1 5 1 1 0 TINF2 (AD) 8 8 0 0 0 0 TERC (AD) 8 0 8 0 0 0 Unknown 4 0 0 15 0 15 Negative 0 26 0 26 Data are presented as median (range) unless otherwise stated. DC: dyskeratosis congenita; XLR: X-linked recessive; AR: autosomal recessive; AD: autosomal dominant; HH: Hoyeraal–Hreidarsson syndrome; RS: Revesz syndrome. #: the number of patients with XLR/AR/TINF2 and AD non-TINF2 do not add up to the total of 43 because the causative gene was not identified in four patients; ¶: oral leukoplakia, dysplastic nails and abnormal skin pigmentation; +: “moderate” was defined as single or multilineage cytopenia not on treatment, and “severe” was cytopenia needing treatment. Significant p-values (<0.05) are in bold.
- TABLE 2
Pulmonary function tests (PFTs) in study participants
PFT abnormalities Patients with DC Unaffected relatives Patients versus relatives All XLR, AR, TINF2 AD non-TINF2 p-value All RTEL1, TERT, PARN All others p-value OR (95% CI) p-value Number with spirometry# 43 25 14 67 14 53 Spirometry abnormal 12 8 4 1.0 11 1 10 0.4 1.97 (0.77–4.9) 0.159 Obstructive 2 1 1 1.0 7 1 6 1.0 0.4 (0.08–2) 0.47 Restrictive 10 7 3 0.7 4 0 4 0.6 4.7 (1.3–16.3) 0.016 Mixed 0 0 0 0 0 0 Number with DLCO data 42 24 14 1.0 66 14 52 Mild DLCO change 23 12 8 0.7 33 5 28 0.4 1.2 (0.5–2.6) 0.695 Moderate DLCO abnormality 11 8 3 1.0 5 2 3 0.3 5.4 (1.7–16.7) 0.003 Severe DLCO abnormality 2 1 1 0 0 0 Abnormal spirometry and/or moderate/severe DLCO reduction 18 12 6 1.0 12 2 10 1.0 3.3 (1.3–7.8) 0.008 DC: dyskeratosis congenita; XLR: X-linked recessive; AR: autosomal recessive; AD: autosomal dominant; DLCO: diffusing capacity of the lung for carbon monoxide. #: the number of patients with XLR/AR/TINF2 and AD non-TINF2 do not add up to the total of 43 because the causative gene was not identified in four patients. Significant odds ratios and p-values are in bold.
- TABLE 3
Factors associated with pulmonary function test abnormalities
Factors evaluated OR (95% CI) p-value DC inheritance: AD non-TINF2 versus AR/XLR/TINF2 0.04 (<0.001–1.57) 0.08 DC triad features: 2 or 3 versus 0–1 0.90 (0.12–6.55) 0.92 Smoker versus nonsmoker 70.85 (1.84– >999.999) 0.02 Sex: male versus female 0.25 (0.02–2.70) 0.25 Age in years at PFT 1.11 (0.99–1.24) 0.07 Lymphocyte telomere Z-score 0.63 (0.20–1.94) 0.42 BMF: severe versus none or moderate 17.36 (1.82–165.30) 0.01 The multivariable regression model used includes dyskeratosis congenita (DC) inheritance (autosomal recessive (AR)/X-linked recessive (XLR)/TINF2 versus autosomal dominant (AD) non-TINF2), DC triad (0–1 versus 2–3), smoking, sex, age at pulmonary function testing (PFT) (integer), lymphocyte telomere Z-score, and bone marrow failure (BMF) (severe versus none/moderate). Overall, 38 patients were included in the multivariable regression model; five patients were excluded (four with unknown gene status and one without telomere length Z-score data). Significant p-values are in bold.
- TABLE 4
Features of patients with dyskeratosis congenita and pulmonary disease
NCI UPN Gene Age at diagnosis years Age at PFT years DLCO Spirometry Age at HCT years HCT regimen Age at PD years Pulmonary symptoms HRCT scan lungs AVM Outcome 160-1 TINF2 3.6 6.6 65% Restrictive 9.5 Cy/Flu/TBI 12 Dyspnoea, ↓SO2 Bibasilar fibrosis progressed over 2 years with features of UIP No Died from pulmonary fibrosis, age 14 years 216-1 AR-RTEL1 6 8.9 51% Obstructive 9.1 Cy/Flu/Bu 14 Dyspnoea, ↓SO2, worse with exercise Interstitial changes with ground-glass opacities mainly in apices c/w NSIP; 2 AVMs Yes, large Pulmonary AVM coiled at age 17 years; alive age 18 years 145-1 TINF2 3 9.5 62% Normal 10.9 Cy/Flu/Bu 15 Dyspnoea, ↓SO2 Normal Yes, liver Died from HPS, age 16 years 87-1 DKC1 3 10.6 49% Restrictive 16.2 Cy/Flu/TBI 17 Cough, air hunger Patchy ground-glass opacities with honeycombing c/w UIP No Died from pulmonary fibrosis, age 18 years 297-2 AR-RTEL1 14 18.3 61% Restrictive 19.3 Flu/C/TBI 22 Dyspnoea, ↓SO2 Numerous small micronodular opacities c/w hypersensitive pneumonitis; linear opacities c/w mild interstitial fibrosis Yes, portal Alive with pulmonary symptoms, age 23 years 204-1# TINF2 3 12.7 <40% Restrictive 4.2 Cy/ATG 11 Cough, air hunger Multifocal areas of reticular and ground-glass opacities with honeycombing c/w UIP No Lung transplant age 13 years; died from oral cancer, age 19 years 231-1# UK 3 9.8 53% Restrictive 3.9 Cy/Flu/TBI 14 Cough, dyspnoea, air hunger Patchy diffuse ground-glass opacities c/w NSIP pattern No Died from pulmonary fibrosis, age 17 years 291-1¶ PARN 13 19.2 25% Restrictive 21 Clubbing, ↓SO2 Increased reticular markings with architectural distortion in upper lung zones suggestive of NSIP Yes, portal Underwent HCT at age 22 years; alive with pulmonary symptoms, age 25 years 6-1 TERC 28 44.6 88% Restrictive 54 Cough, dyspnoea, ↓SO2 Peripheral interstitial and ground-glass opacities with honeycombing in bases bilaterally c/w UIP No Alive on supplemental O2, age 58 years 114-1 TERC 34 56.7 57% Restrictive 56.7 Dyspnoea on exertion Progressive polygonal and reticular opacities both lung bases and upper lobes c/w UIP Alive, has dyspnoea and ↓SO2 on exertion, age 59 years 350-1¶ TERC 44 59.5 61% Obstructive 59.54 Cough, dyspnoea, ↓SO2 Decreased lung volume; both lower lobes with increased interstitial markings in the periphery with areas of honeycombing (UIP and NSIP pattern) No Underwent HCT at age 63 years; died from HCT complications 329-1 TERT 65 69 34% Restrictive 65 Dyspnoea, ↓SO2 Extensive areas of honeycombing and peripheral fibrosis more marked in lung bases c/w UIP No Died from pulmonary fibrosis, age 69 years NCI UPN: National Cancer Institute unique patient number; PFT: pulmonary function test; DLCO: diffusing capacity of the lung for carbon monoxide; HCT: haematopoietic cell transplantation; PD: pulmonary disease; HRCT: high-resolution computed tomography; AVM: arteriovenous malformation; AR: autosomal recessive; UK: unknown; Cy: cyclophosphamide; Flu: fludarabine; TBI: total body irradiation; Bu: busulfan; ATG: antithymocyte globulin; SO2: oxygen saturation; UIP: usual interstitial pneumonia; c/w: consistent with; NSIP: nonspecific interstitial pneumonia; HPS: hepatopulmonary syndrome. #: underwent HCT prior to PFT evaluation; ¶: underwent HCT after the diagnosis of AVM and interstitial fibrosis.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00209-2019.supplement










