





Abstract
High-resolution CT assessment of airway volumes after bronchial thermoplasty (BT), together with model predictions regarding the efficacy and underlying mechanism of action of the treatment, combine to help to elucidate the underlying mechanism of BT http://bit.ly/2WPHY6y
To the Editor:
Bronchial thermoplasty (BT) is a recent treatment for moderate-to-severe asthma in which the airway smooth muscle (ASM) layer is targeted directly using thermal energy delivered during bronchoscopy. Although direct targeting of the ASM is appealing because of its role in bronchoconstriction in asthma, BT is not widely used because direct physiological effects after treatment (e.g. changes forced expiratory volume in 1 s (FEV1) or the concentration of methacholine required to decrease FEV1 by 20%) have not been shown consistently [1–3]. Instead, clinical response is demonstrated through indirect measurements, such as improved Asthma Control Questionnaire (ACQ) and Asthma Quality of Life Questionnaire scores, and reduced use of rescue medication [1, 2], acknowledging that there is also a considerable placebo component [3]. These findings leave doubt about the efficacy and mechanism of action of BT. Recent work, however, has demonstrated a direct change in a new physiological measure, namely airway volume assessed by high-resolution computed tomography (CT) [4].
We have also previously suggested, based on model predictions, that the principle mechanism of BT is redistribution of flow patterns due solely to structural changes in the treated airways [5]. The model incorporates extensive post mortem structural data from human subjects with different degrees of asthma severity, and key aspects of the model included airway–parenchymal interactions where inflated alveoli distend bronchial passages. Regional flow relationships are maintained within the model such that obstruction in proximal airway segments disrupts flow to the lung periphery. Importantly, the model only “treated” the same large airways that are targeted in normal BT practice, by mathematically reducing the thickness of the ASM layer to the level reported in biopsy studies. Using this approach, we predict that the effects of treatment propagate functionally to the peripheral airways via these flow patterns, but this does not necessarily involve structural changes to the peripheral airways. These functional effects are difficult to demonstrate clinically because they are very small at baseline but increase with the degree of ASM activation and disease severity [5]. Safety considerations preclude inducing these situations in the clinic, but they should still occur in uncontrolled situations outside the clinic, and subsequently manifest in indirect measures like the ACQ and rescue medication use.
In this letter, we show that changes in airway volumes, assessed in patients by high-resolution CT at both functional residual capacity (FRC) and total lung capacity (TLC), agree with model predictions for the changes in the volume of BT-treated airways. All patients met the definition of severe asthma, despite high-dose inhaled corticosteroids and dual long-acting bronchodilators; detailed subject characteristics are given in the figure 1 caption. Data were acquired and analysed using the same methodology as used in our previous study [4] but with new data from eight additional patients (now 18 in total). High-resolution CT imaging studies in this protocol were performed at baseline and then again 4 weeks after the left lung underwent BT treatment, but prior to any treatment of the right lung, which therefore served as a control. Note that the conventional treatment order was altered to allow the untreated right lung to serve as a control mid-treatment [4].
{kind=link}
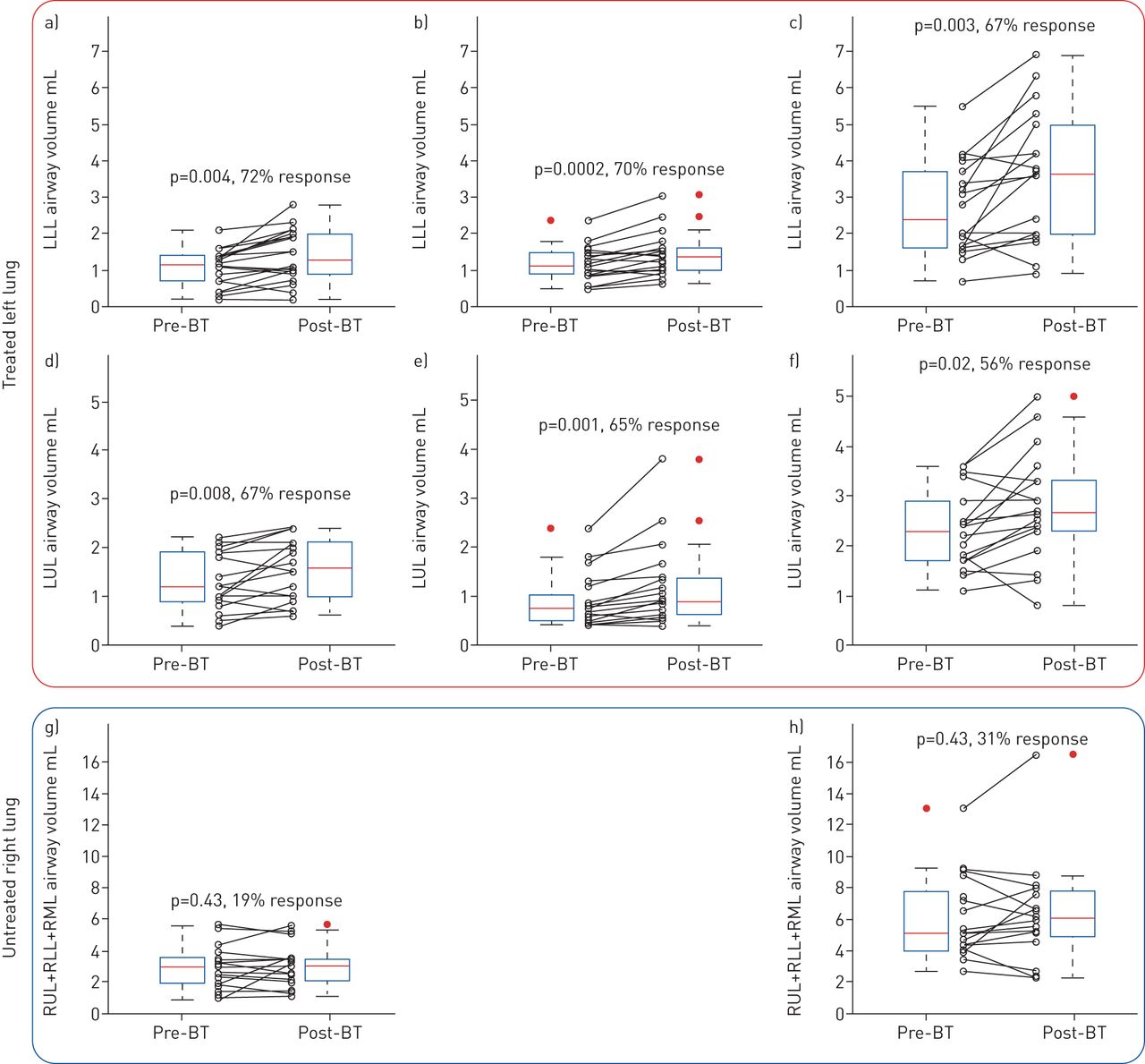
Comparison of volume of bronchial thermoplasty (BT)-treated airways in a, c, d and f) each patient as assessed by computed tomography (CT) (eight patients) and model predictions (20 simulations). CT measurements at a, d and g) functional residual capacity (FRC) and c, f and h) total lung capacity (TLC) are compared with b and e) model predictions. Model predictions are for fatal asthma at a low level of airway smooth muscle activation [5]. The response threshold is defined as an increase in airway volume that exceeds half of the interquartile range of the intervisit variability, as assessed on the untreated right side (∼8.5% at FRC and ∼17% at TLC). p-values reflect paired t-tests. The untreated right lung was not modelled. Subject characteristics were as follows. Males: seven out of 18 patients; mean±sd age 57.6±14.2 years; BMI: 32.1±7.2 kg·m−2; cigarettes: 10 never-smokers, eight ever-smokers; Asthma Control Questionnaire (ACQ) score (baseline): 3.5±0.9; oral steroids: 15/18 mg·day−1, mean 14.3±15.8 mg·day−1; forced expiratory volume in 1 s: 44.9±13.7% pred; ACQ score after one lung treated: 2.4±1.2. The protocol was prospectively reviewed and approved by the Peninsula Health Human Research Ethics Committee. LLL: left lower lobe; LUL: left upper lobe; RUL: right upper lobe; RLL: right lower lobe; RML: right middle lobe.
Figure 1 shows the changes in airway volumes, broken down by lobe and lung volume, expressed as paired box plots. Volumes acquired by CT (18 patients) are given both at FRC and TLC, and these are compared with simulations (N=20, tidal breathing average; data from [5]). The top row (figure 1a–c) shows observations and predictions for the left lower lobe (LLL) and the middle row (figure d–f), for the left upper lobe (LUL); the left column (figure 1a and d) gives CT data at FRC; the centre column (figure 1b and e), the model predictions (tidal average); and the right column (figure 1c and f) the CT data at TLC. As in the study by Langton et al. [4], reported airway luminal volumes are summed from the lobar and segmental airways, and branches down to 2 mm in diameter, as reported on an independent, commercial basis by FLUIDDA (Kontich, Belgium). These airways are assumed to be BT-treated. In the model, BT-treated airway volumes are computed directly.
In both the LUL and LLL, treated airway volumes show significant increases at FRC and TLC, and in model predictions, as well as consistent response rates. Model predictions agree very well with the CT-acquired volumes. For comparison, the airway volumes in the untreated right lung are shown in figure 1g and h at FRC and TLC respectively; as in our previous study [4], no significant changes were observed in the untreated right lung. Treatment responses were not significantly different between the LUL and LLL. It is also worth noting that the high-resolution CT data were acquired before and after an inspiratory capacity manoeuvre, while the model assumed tidal breathing; this precludes direct, quantitative comparison of the two, but it is reasonable to assume that the airway volume changes observed in tidal breathing should lie between those observed at FRC and at TLC. The relationship between change in airway volume at TLC and change in ACQ score was also assessed but did not reach statistical significance (p=0.14, consistent with [4]). However, a global measure such as the ACQ may respond more strongly to treatment of both sides and so firm conclusions await the availability of the full data set with both lungs treated.
What does this tell us about the underlying mechanism of BT? First, this is evidence of a direct, physiological effect of BT, to compliment previous reports of changes in total lung volumes [6]. Unlike indirect measurements (e.g. ACQ), no placebo component is likely. Second, the characteristics of the response agree extremely well between predictions and observations, supporting the model predictions for post-BT airway behaviour and therefore consistent with the hypothesis that treatment of a relatively small number of large airways can modulate downstream flow patterns, resulting in subsequent improvements in global function. Some untreated airways with diameter >2 mm may be measured by CT, but downstream changes in smaller airways are not directly assessed by CT but could be assessed by hyperpolarised gas magnetic resonance imaging [7], and indeed we may hope to see this done in the near term [8, 9]. Establishing the mechanism of BT provides an opportunity for better patient selection and/or predicting response to therapy [10].
Further understanding might also be obtained by analysing airway volumes not just on a lobe-by-lobe basis, but on a more detailed airway-by-airway basis. A mixed response is perhaps to be expected, with some airways showing dilation and increased flow in response to BT, while others exhibit no change or even a reduction in calibre. This might be thought of as a kind of paradoxical constriction, as compared with expected dilation – akin to paradoxical dilation in response to contractile stimulus [11]. Model predictions show just such a response: a mean 15.9% increase in treated airway volume, with 60% of treated airways showing a >5% increase and 51% of airways increasing >10%. The mixed response is evident in the airways predicted to decrease in volume: 20% decreasing >5% and 11% decreasing >10%. This mixed response is broadly consistent with the limited data available from BT on a segmental basis [7]. Comparable airway-by-airway data from CT remain to be tested in future pending improvements in image registration or perhaps using optical coherence tomography [12, 13]; when available, it will further aid our understanding of the processes behind BT.
In closing, this report extends our previous findings [4] and those of Donovan et al. [5], and clearly demonstrates improvement in lung physiology after BT. It is the opinion of the authors that the field is moving in the right direction in considering methods of assessment beyond conventional lung function.
Footnotes
Conflict of interest: D. Langton has nothing to disclose.
Conflict of interest: P.B. Noble has nothing to disclose.
Conflict of interest: F. Thien has nothing to disclose.
Conflict of interest: G.M. Donovan has nothing to disclose.
- Received October 1, 2019.
- Accepted November 5, 2019.
- Copyright ©ERS 2019
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










