





Abstract
Introduction Individuals with interstitial lung disease (ILD) exhibit reduced exercise capacity and exertional hypoxaemia. The role of peripheral (muscle) limitation to exercise tolerance in ILD is not well studied to date.
Methods A prospective cross-sectional study examined skeletal muscle oxygen saturation (SmO2) and regional blood volume of the knee extensors and elbow flexors during incremental limb loading in healthy people and people with varying severity of ILD. Isotonic concentric exercise was performed on an isokinetic dynamometer. SmO2 and regional blood volume were measured by near-infrared spectroscopy over the vastus lateralis and biceps.
Results Thirteen people who were dependent on oxygen, candidates for lung transplant and with severe ILD (forced vital capacity (FVC) 59±20% predicted), 10 people who were not oxygen dependent with mild ILD (FVC 81±17% predicted) and 13 healthy people (FVC 101±14% predicted) were included. Total haemoglobin, a marker of regional blood volume, was lower at task failure in the knee extensors in participants with severe ILD compared to healthy participants (p=0.05). At task failure for both knee-extensor loading and elbow-flexor loading, SmO2 was decreased to similar levels across all groups, but occurred at lower total workloads in the ILD groups (all p<0.01).
Conclusions Overall, people with severe ILD had lower levels of total work and experienced less increase in blood volume in the knee extensors after knee-extensor loading compared to healthy people. Peripheral muscle dysfunction in severe ILD may have contributed to muscle deoxygenation at lower workloads.
Abstract
Muscle deoxygenation occurs at a lower level of lower-limb incremental loading in lung transplant candidates with interstitial lung disease and regional blood volume is attenuated compared to healthy persons http://bit.ly/34z0Qtw
Introduction
Interstitial lung disease (ILD) is a heterogeneous chronic lung condition associated with the disabling symptoms of dyspnoea and fatigue, reduced exercise capacity, lower levels of physical activity and impaired health-related quality of life (HRQOL) [1–4]. Exercise training is recommended in ILD to improve symptoms, exercise capacity and HRQOL [5, 6]. Impairment of gas exchange leading to exertional hypoxaemia is commonly observed in many ILDs and contributes to exercise limitation [3, 7]. The intensity and duration of exercise training is often guided by an adequate arterial blood oxygen saturation measured by pulse oximetry (SpO2); however, SpO2 does not provide information about regional oxygenation of the exercising muscle. There is emerging evidence of peripheral muscle dysfunction in ILD, such as muscle atrophy and reduced skeletal muscle strength and endurance [8]. Reduced functional exercise capacity and physical activity levels are important clinical implications of lower-limb peripheral muscle strength in ILD [4, 9, 10]. The underlying skeletal muscle pathophysiology contributing to muscle dysfunction in ILD is not well studied to date [11]. Reduced arterial oxygen content may result in muscle deoxygenation limiting exercise capacity and performance.
Near-infrared spectroscopy (NIRS) is a noninvasive optical technique that uses differential absorption properties of infrared light to evaluate skeletal muscle oxygen saturation (SmO2) and regional blood volume of the microcirculation (arterioles, capillaries and venules) [12]. Chromophores that can be measured include oxygenated haemoglobin (O2Hb) and deoxygenated haemoglobin (HHb) [13]. Total haemoglobin (tHb), haemoglobin difference (Hb-diff) and SmO2 can be calculated from O2Hb and HHb [13]. NIRS can provide insight into the state of oxygen utilisation and local blood distribution at the level of the tissues [12] and therefore could be used to characterise peripheral muscle dysfunction during exercise. Changes in muscle oxygenation during unilateral resistance loading of a muscle group has not been previously examined in ILD. The overall aim of this study was to examine changes in SmO2 during limb exercise in people with a varying severity of ILD as well as healthy people. The specific objectives were to: 1) examine between and within-group differences in SmO2 and regional blood volume during incremental loading and at task failure; and 2) examine whether systemic arterial oxygen saturation measured by SpO2 is associated with regional SmO2.
Methods
Participants
Three groups were recruited for this study: adults with non-oxygen-dependent mild ILD, oxygen-dependent adult lung transplant candidates with severe ILD and healthy, nonsmoking, age and sex-matched people. Lung transplant candidates were recruited from the lung transplant programme at the University Health Network, Toronto, Canada, where they had been participating in pre-transplant rehabilitation for less than 4 weeks at the time of study recruitment. Participants with mild ILD were recruited from the ILD clinic at the same facility. Healthy people were recruited from a university community and screened with spirometry and a health/fitness facility pre-participation questionnaire [14]. Study recruitment occurred between November 2016 and June 2017 for all groups. Exclusion criteria for all study subjects were: 1) adipose tissue thickness >10 mm at the NIRS monitoring sites (mid-femur and mid-humerus); 2) <45 or >75 years of age; 3) active myositis; and 4) muscle or joint issues that would interfere with testing. In addition, lung transplant candidates were excluded if they were listed as rapidly deteriorating, were hospitalised or were awaiting a re-transplantation or multiorgan transplantation (heart-lung or lung-liver). The study was approved by the University Health Network and the University of Toronto research ethics boards. All participants provided written informed consent.
Protocol
Testing was conducted in a single session.
Adipose tissue and muscle layer thickness
Muscle layer thickness of the knee extensors and elbow flexors of the dominant limb was measured using B-mode ultrasound imaging (5–13 MHz linear transducer, GE Logic E system, GE Medical Systems, Milwaukee, WI, USA). The landmarks were chosen based on the desired placement of the NIRS probes. Specifically, the lateral quadriceps (vastus lateralis and vastus intermedius) were landmarked a third of the distance between the midpoint of the superior border of the patella to the anterior superior iliac spine and 8 cm lateral to this midpoint. The elbow flexors were landmarked a third of the distance between the midpoint between the epicondyles of the humerus to the acromion process. The thenar eminence of the nondominant hand was designated as a control muscle, with skin, adipose and muscle layer thickness measured over the thickest part of the muscle belly.
Muscle oxygenation and regional blood volume
O2Hb and HHb were measured using spatially resolved NIRS (PortaMon and PortaLite, Artinis Medical Systems, BV, The Netherlands) [13]. The following variables were calculated by the software: tHb (O2Hb+HHb), Hb-diff (O2Hb–HHb) and SmO2 (O2Hb/tHb)×100. The subject's skin was cleaned with alcohol and the optodes were secured with tape directly over the ultrasound landmarks. NIRS values (O2Hb, HHb and tHb) were zeroed at the start point of each incremental test. Data were acquired at 10 Hz using NIRS software (Oxysoft, Artinis Medical Systems, BV, The Netherlands). The ultrasound measures of adipose and muscle layer thicknesses were used to determine the depth of light penetration needed to reach halfway through the muscle, and the appropriate transmitter optode was chosen based on this depth for later data analysis using NIRS software.
Isometric peak torque testing
Isometric peak torque of the knee extensors and elbow flexors was measured on an isokinetic dynamometer (Biodex System 4, Shirley, NY, USA) on the dominant limbs using a standard protocol. For the knee extensors, the participant was seated upright with shoulder and hip straps and the axis of the dynamometer was aligned to the knee joint. An isometric test at 90° of knee flexion was performed for 5 s using standardised verbal encouragement followed by a 1-min rest. For the elbow flexors, the participant was seated upright with shoulder, hip and elbow straps, and the axis of the dynamometer aligned to the elbow joint. Their forearm rested on an arm support as they gripped a handle. An isometric test at 60° of elbow flexion was performed. The highest torque of five repetitions was designated as 100% maximal voluntary isometric contraction (MVIC) for both tests.
Incremental loading of knee extensors and elbow flexors
Participants were stratified by sex, age and diagnostic category (healthy, mild ILD and severe ILD) and the assignment of the incremental test order was alternated to ensure balance. At 5 min after completing the isometric testing, the incremental protocol was performed using an isotonic concentric testing mode. As we were interested in task failure and anticipated that healthy participants would be stronger, the initial load was set to 10% of MVIC and increased by 10% MVIC every 2 min until task failure, rather than using an absolute load increase. For the knee-extensor-loading (KEL) protocol, participants were required to contract the knee extensors from 90° to 10° of knee flexion, and for the elbow-flexor-loading (EFL) protocol participants were required to contract the elbow flexors from 60° to 140° of flexion. A duty cycle of 1 s contraction to 5 s rest was used, resulting in 20 contractions over each 2-min increment. A metronome was used to standardise the timing of the contractions. The torque, position and velocity data from the isokinetic dynamometer was sampled at 100 Hz and collected using a real-time, data acquisition system (Biopac Systems Canada Inc. and Acqknowledge software, version 4). Task failure was defined as one of the following: failure to meet the required range of motion (80°) or contraction velocity (80°·s−1) for three successive contractions, participant requested to stop due to fatigue, discomfort or significant cardiorespiratory symptoms (SpO2 <80%, severe dyspnoea or respiratory distress), or excessive muscle compensation was observed. The incremental loading tasks were separated by a rest time of 30 min.
Cardiorespiratory responses
Dyspnoea sensation and rating of perceived exertion for arm and leg fatigue were quantified using a modified Borg 0–10 scale before, during and immediately after KEL or EFL tests [15]. Throughout the incremental loading, SpO2 and heart rate were measured continuously using pulse oximetry (Nonin 4000, Roxon Medi-Tech Inc., Saint-Leonard, QC, Canada). The participants with severe ILD used the same level of supplemental oxygen that they were prescribed for resistance training during their pre-transplant rehabilitation programme.
Statistical analysis
All data were tested for normality using the Shapiro–Wilk test and reported as mean± sd unless otherwise described. Between-group differences in functional characteristics, cardiorespiratory responses to loading and changes in chromophores (O2Hb and HHb) and NIRS-derived variables (SmO2, tHb, Hb-diff) at the end of exercise (task failure) were examined using one-way ANOVA with a subsequent Tukey's post hoc test if significant. Within-group differences in chromophores and NIRS-derived variables at task failure compared to rest were examined using a paired t-test or Wilcoxon signed-rank test. To examine the change during incremental loading, the task duration was divided into quintiles, with differences examined using repeated-measures ANOVA with a subsequent Tukey's (between-group) and Dunnett's post hoc test (within-group) with the reference point as the baseline (resting) measure. To examine the relationship between SmO2 and SpO2 at task failures from KEL and EFL, a Spearman rank correlation analysis was performed. The level of significance for all analyses was p≤0.05. Statistical analysis was performed on SAS statistical software, University Edition. The sample size calculation was based on the effect size on the mean change in biceps O2Hb during elbow-flexor loading in a chronic obstructive pulmonary disease (COPD) population (−15.5) as there were no previous data in ILD; however, the incremental protocols and research design differed [16]. An α of 0.05 and power of 0.9 resulted in an estimated sample size calculation of 15 individuals per group.
Results
Participant characteristics
Thirteen healthy participants, 10 individuals with mild ILD (FVC 81±17% predicted) and 13 oxygen-dependent lung transplant candidates with severe ILD (FVC 59±20% predicted) participated. There was an equal proportion of women in each group. Participant characteristics are described in (table 1). The mean change in O2Hb during elbow-flexor loading was less in our study sample than what was observed in the study of COPD participants used to determine the effect size [16], and a post hoc power calculation revealed that 25 participants per group would be required. As the study may have been underpowered, there is a possibility of a Type II error.
Participant characteristics (n=36)
Incremental loading
The mild and severe ILD groups performed less total work during KEL (p=0.006) compared to the healthy group (table 2 and figure 1). The severe ILD group performed less total work during EFL compared to the healthy and mild ILD groups (p=0.001) (table 2 and figure 1). The severe ILD group had a higher end-exercise dyspnoea than the healthy and mild ILD groups after KEL and EFL (table 2); however, dyspnoea and/or significant oxygen desaturation was not a reason for task failure for any of the participants. Reasons for task failure in all groups included the inability to maintain the specified velocity or range of motion without excessive muscle compensation.
Incremental limb-loading characteristics (n=36)

End-exercise (task failure) muscle oxygen saturation (SmO2) over total workload (n=36). a) Knee-extensor loading (KEL); b) elbow-flexor loading (EFL). ILD: interstitial lung disease.
NIRS outcomes at task failure
At KEL task failure, SmO2 decreased from rest in the healthy and severe ILD groups, HHb increased in the healthy group and tHb increased in the healthy and mild ILD groups (all p≤0.05; figures 2 and 4). There was a lower tHb in the severe ILD group compared to the healthy group (p=0.05; figure 4). At EFL task failure, SmO2 decreased from rest in the mild and severe ILD groups (all p<0.05; figure 3), with no differences in HHb or tHb from rest in any groups. There were no within or between-group differences in the control muscle (thenar eminence) from rest to KEL or EFL task failure.

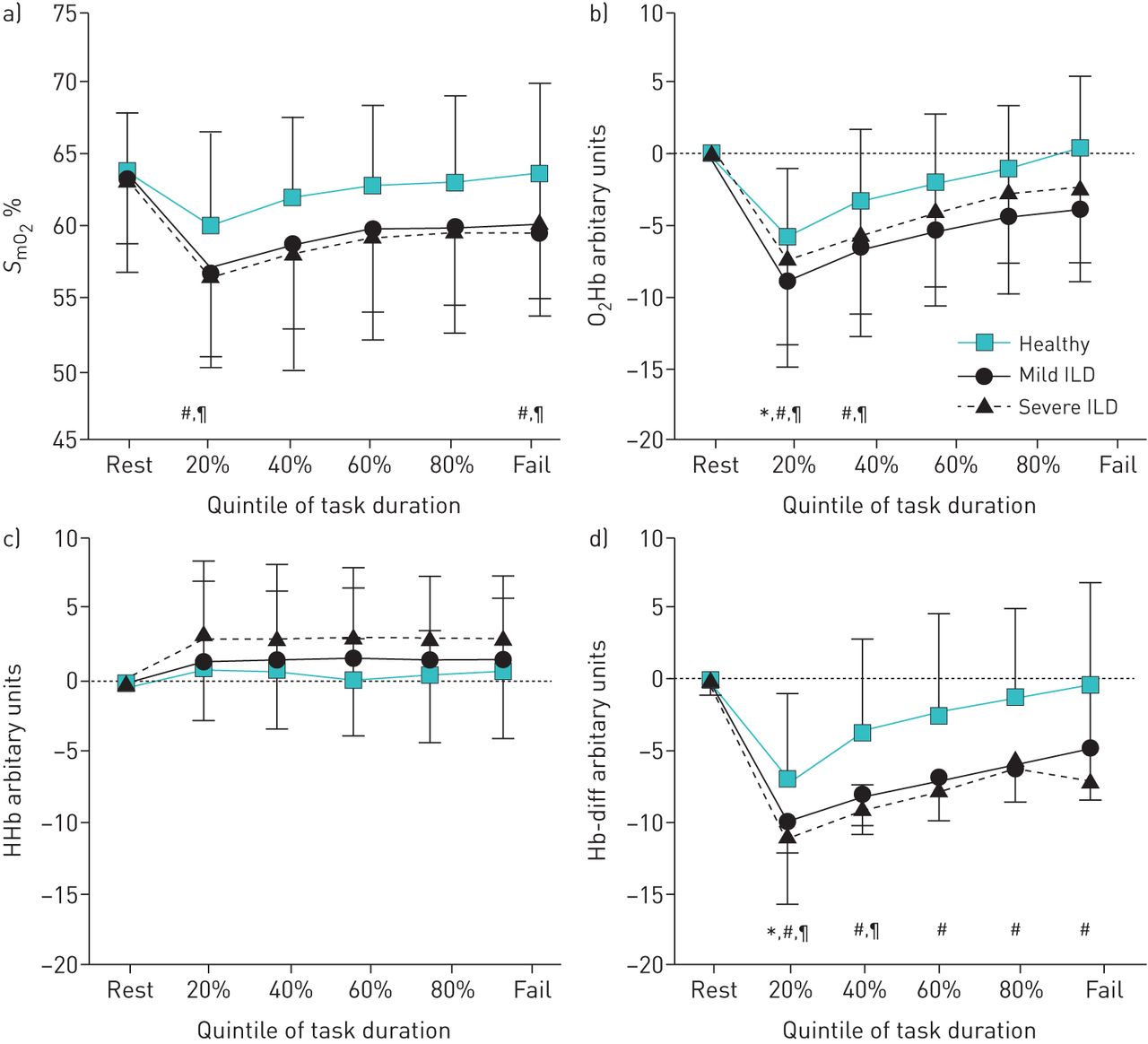
Change in a) muscle oxygen saturation (SmO2), b) oxygenated haemoglobin (O2Hb), c) deoxygenated haemoglobin (HHb) and d) haemoglobin difference (Hb-diff) during incremental knee-extensor limb loading. ILD: interstitial lung disease. *: p≤0.05 for healthy subjects; #: p≤0.05 for severe ILD.

Change in a) muscle oxygen saturation (SmO2), b) oxygenated haemoglobin (O2Hb), c) deoxygenated haemoglobin (HHb) and d) haemoglobin difference (Hb-diff) during incremental elbow-flexor limb loading. ILD: interstitial lung disease. *: p≤0.05 for healthy subjects; #: p≤0.05 for mild ILD; ¶: p≤0.05 for severe ILD.

Change in total haemoglobin (tHb), an estimate of regional blood volume during incremental limb loading. a) Knee-extensor loading; b) elbow-flexor loading. ILD: interstitial lung disease. *: p≤0.05 for healthy subjects; #: p≤0.05 for mild ILD.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between muscle oxygen saturation (SmO2) and arterial oxygen saturation measured by pulse oximetry (SpO2) at task failure following incremental limb loading. a) Knee-extensor loading (KEL); b) elbow-flexor loading (EFL). ILD: interstitial lung disease.
NIRS outcomes during incremental loading
During KEL and EFL there were within-group differences over time for SmO2, O2Hb, HHb, Hb-diff and tHb (all p≤ 0.05 figures 2–4). During KEL, the severe ILD group had a lower O2Hb and Hb-diff at the 20th percentile of task duration compared to rest (figure 2). During EFL both mild and severe ILD had a lower SmO2 at the 20th percentile compared to rest (figure 3). O2Hb was lower during EFL at 20th percentile in all groups (figure 3) and also at the 40th percentile in both ILD groups (figure 3). Hb-diff was lower in all groups at the 20th percentile, lower in the severe ILD group at the 40th percentile and at all time points in the mild ILD group (figure 3).
Relationship between whole body and local muscle oxygenation at task failure
There were no correlations between SmO2 and SpO2 at task failure following KEL and EFL in any of the groups (figure 5).
Discussion
This is the first study to evaluate muscle oxygenation and regional blood volume during incremental loading in ILD. Following upper and lower-limb loading we found a similar level of muscle oxygenation (SmO2, O2Hb, HHb and Hb-diff) in active muscles in participants with mild ILD, oxygen-dependent severe ILD and healthy people; however, deoxygenation occurred at a lower total workload in the ILD groups. Total haemoglobin, reflecting regional blood volume, was lower in the severe ILD group compared to healthy people during lower-limb incremental loading.
Muscle oxygenation measured using NIRS reflects the dynamic balance between local oxygen supply by the microcirculation and oxygen consumption by the mitochondria [12]. SmO2 can decrease due to increased muscle oxygen extraction to support increased workloads, or can decrease from a reduction in oxygen supply/delivery. The increase in HHb after KEL in the healthy group suggests increased muscle oxygen extraction during the incremental loading protocol. The use of supplemental oxygen in the severe ILD group likely had a significant influence on blood flow and oxygen delivery, and subsequently on the NIRS-derived variables. However, we were interested in including these participants in this study as they participate in pulmonary rehabilitation and undergo isotonic resistance loading exercise. SpO2 is often used to prescribe and progress exercise training in pulmonary rehabilitation programmes. However, SpO2 is an indication of oxygen delivery calculated from pulsatile arterial blood, whereas the NIRS signal arises from small vessels (arterioles, capillaries and venules) in the local tissue being monitored, thereby providing additional information on tissue oxygen supply and extraction [12]. In this study, muscle oxygenation was not significantly correlated with SpO2 during isotonic loading.
Although there was a cardiorespiratory response during incremental loading in all groups, it was not a rate-limiting response, as only moderate heart rate levels were reached and dyspnoea scores were low to moderate. The mean oxygen saturation (SpO2) was ≥95% at task failure in both ILD groups, and only two individuals with severe ILD dropped to a SpO2 <90% during KEL. Although arterial oxygen saturation was not significantly reduced, individuals with ILD may have been less able to extract the available oxygen due to peripheral muscle dysfunction [17, 18]. SmO2 at task failure was not reduced from rest in mild ILD during KEL, which may indicate decreased oxygen extraction. When examining peripheral muscle dysfunction in ILD, it is difficult to determine the effect of deconditioning from the effect of the disease process. While we cannot rule out deconditioning, all ILD participants were living in the community and were ambulatory without the use of a gait aid. The mean 6-min walk distance was 83% predicted in participants with mild ILD, and 62% predicted (and close to 400 m) in participants with severe ILD. Additionally, the severe ILD participants were not considered to be too deconditioned so as to be excluded from transplant listing, and all were participating in a rehabilitation programme of aerobic and resistance training for at least 2–4 weeks at the time of the study assessment.
Two studies have examined muscle oxygenation in people with ILD during high intensity aerobic exercise. McNarry et al. [18] examined HHb of the vastus lateralis as an indicator of oxygen extraction during cycling. They found that both pulmonary oxygen uptake and HHb kinetics were slower in people with idiopathic pulmonary fibrosis compared to healthy participants. Keyser et al. [19] examined muscle oxygenation of the gastrocnemius during 10 weeks of high intensity aerobic training and found improved muscle oxygen extraction (increased HHb and difference of O2Hb-HHb) following training without an increase in central oxygen delivery or muscle oxygen availability. In our study, seated isotonic resistance exercise was examined, which likely placed less demand on gas exchange compared to aerobic exercise. Reid et al. [16] examined muscle oxygenation of the elbow flexors during seated incremental EFL in 12 people with moderate-to-severe COPD and found a decreased O2Hb at all time points during loading. An isokinetic loading protocol with set load increments (as compared to a percentage of MVIC) and a greater range of motion and test duration was used, and study participants did not use supplemental oxygen, which may have led to a greater decrease in O2Hb than observed in this study. Mechanisms and the degree of peripheral muscle dysfunction may also differ in COPD compared to ILD.
Blood volume beneath the NIRS optodes (tHb) was lower in the severe ILD group compared to the healthy group during lower-limb incremental loading but not in upper-limb loading. The knee extensors are a larger muscle group than elbow flexors and a higher total workload (in Joules) was reached during KEL than EFL. This may have led to higher cardiorespiratory responses during KEL and a greater blood volume may have been distributed to the respiratory muscles in the severe ILD group. Alterations in vascular response to exercise may have attenuated blood flow redistribution to contracting muscles in ILD. A compromised vascular bed may also have contributed to a reduction in tHb. While hyperoxia has been shown to decrease peripheral muscle blood flow and increase vascular resistance [20], it is not clear whether participants with oxygen-dependent severe ILD were in a state of hyperoxia. Variable performance oxygen delivery devices were used at levels that would provide an estimated inspiratory oxygen fraction of 0.28–0.65. The SpO2 before and after incremental loading was not different from the other two groups.
Limitations
The isotonic workloads were based on an individual's MVIC rather than an absolute load increase, and the trials lasted different lengths of time until task failure. Although loads were increased by 10% of MVIC and NIRS variables were compared at specific time points of total task duration, this protocol did not allow us to examine differences in muscle oxygenation and changes in blood volume among groups at isowork. There were more men recruited, as women tended to have more subcutaneous adipose thickness in the thigh region and were excluded due to the limitations of NIRS. Sex differences were not explored. Only a few centimetres of superficial muscle can be sampled using NIRS. The vastus lateralis is only one muscle involved in knee extension, and as electromyography was not used, we could not measure how much the vastus lateralis was recruited compared to the other muscles of the quadriceps. Although active myositis was an exclusion criterion, conditions such as rheumatoid arthritis and Sjogren's may involve muscle directly and lead to myopathy. There were also two participants with combined COPD and ILD, and COPD may affect muscles in a different way than ILD.
Conclusions
This exploratory study demonstrated that muscle deoxygenation occurred at a lower level of total work in severe ILD and regional blood volume was attenuated compared to healthy persons during lower-limb incremental loading. This provides insight into possible exercise limitations in ILD. A future study examining whether resistance training improves muscle oxygen saturation at higher isotonic workloads in ILD is warranted.
Footnotes
Support statement: This study was funded by an Ontario Respiratory Care Society research grant. L. Wickerson was supported by graduate fellowships from the Canadian and Ontario Lung Associations, and the University of Toronto. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: L. Wickerson has nothing to disclose.
Conflict of interest: S. Mathur has nothing to disclose.
Conflict of interest: D. Brooks has nothing to disclose.
Conflict of interest: L.V. Bonetti has nothing to disclose.
Conflict of interest: L.G. Singer has nothing to disclose.
Conflict of interest: J. Granton does not have any disclosures relating to this study
Conflict of interest: W.D. Reid has nothing to disclose.
- Received March 31, 2019.
- Accepted November 20, 2019.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










