





Abstract
Objectives The aim of this study was to establish whether early pulmonary rehabilitation after severe exacerbation of chronic obstructive pulmonary disease (COPD) reduces mortality and hospital admissions, and increases physical performance and quality of life compared to rehabilitation initiated later in the stable phase of COPD.
Methods In a randomised controlled trial of 150 patients hospitalised with an exacerbation of COPD, participants were allocated to pulmonary rehabilitation either within 2 weeks after discharge or the same rehabilitation programme but initiated 2 months after discharge.
Results Early pulmonary rehabilitation did not prolong time to first hospital admission or time to death (hazard ratio 0.79, 95% CI 0.47–1.23, p=0.33) compared to rehabilitation in stable phase. However, 2 months after inclusion, pulmonary rehabilitation resulted in a significantly better improvement in the incremental shuttle walk test (33.9 m, 95% CI 4.18–63.7, p=0.02) compared to that in the stable phase. The difference in the endurance shuttle walk test was of borderline significance (140 s, 95% CI −2.03–282.76, p=0.05), but there was no significant difference concerning the COPD assessment test (−1.43 points, 95% CI −3.44–0.59, p=0.17).
Conclusion Early pulmonary rehabilitation after acute exacerbation of COPD led to a faster improvement in physical performance compared to rehabilitation initiated later in the stable phase, but did not improve survival or prolong time to hospital readmission.
Abstract
Early pulmonary rehabilitation shortly after #AECOPD leads to a faster recovery in physical performance than initiated in the stable phase. Adherence to rehabilitation is significantly higher when initiated shortly after an exacerbation. http://bit.ly/2S7XsT9
Introduction
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is frequent in severe chronic obstructive pulmonary disease (COPD). AECOPD is among the most common causes of hospitalisation, it increases the decline in lung function and repeated exacerbations are associated with higher readmission rates to hospital and increased mortality [1–3]. Furthermore, severe AECOPD is associated with worsening of symptoms and impairment of physical and psychological wellbeing [4, 5]. Although symptoms after AECOPD usually last 7–10 days, about 20% of the patients have not fully recovered after 8 weeks [6].
Pulmonary rehabilitation plays a key role in the management of COPD. It has a significant impact on reducing symptoms and increasing exercise capacity and quality of life in patients with stable COPD [7]. Due to the deterioration in the patient's physical performance and quality of life during exacerbation, pulmonary rehabilitation initiated immediately after AECOPD is expected to show a larger beneficial effect compared to when it is introduced later in stable COPD. In fact, early pulmonary rehabilitation after AECOPD seems to reduce the risk of recurrent hospital admissions and mortality, although the results have not been uniform, and one large study reported increased mortality [8, 9]. However, in spite of great heterogeneity between the studies, a systematic review by Puhan et al. [10] in 2016 evaluating the effect of early rehabilitation compared to no rehabilitation, concluded that pulmonary rehabilitation is an effective intervention after an exacerbation regarding exercise capacity and health-related quality of life and also found beneficial effects on mortality and hospital admissions. The investigators suggested that the heterogeneity between the results could be explained by the difference in the extensiveness of the rehabilitation programmes and the methodological quality of the studies.
We therefore conducted a randomised controlled trial investigating the effect of a comprehensive and standardised pulmonary rehabilitation programme initiated within 2 weeks after discharge from hospital compared to a similar rehabilitation programme initiated in the stable phase, 2–3 months after discharge, in patients admitted with an AECOPD.
Methods
Study design
This study was an investigator-initiated single centre open-label randomised controlled clinical trial conducted at the Department of Respiratory Medicine at Gentofte Hospital in Denmark. Approval was obtained from the local ethics committee (H-2-2013-143) and the study was registered in ClinicalTrials.gov (NCT02987439). We used sealedenvelope.com to prepare the sequence allocation and the patients were allocated 1:1 to either early or later pulmonary rehabilitation, using sealed opaque envelopes. Participants readmitted to hospital during the study were not randomised again but remained in their initial treatment group.
We assessed data at discharge from hospital at baseline and outcomes at 2 and 6 months follow-up. Mortality and hospital readmissions were recorded at 12 months.
Primary outcome
Composite outcome of 1-year mortality was measured as all-cause mortality at 12 months and readmission was defined as at least one hospital readmission due to any cause in the 12-month follow-up period. This outcome was chosen as it was used in a Cochrane review in 2011 [11].
Secondary outcome
These included: 1-year all-cause mortality and time to death, all-cause hospital readmission and time to readmission, proportion of participants with at least one hospital readmission due to any cause, hospital readmission due to a respiratory cause, exercise performance measured by the incremental shuttle walk test (ISWT) [12] and the endurance shuttle walk test (ESWT) [13], and health-related quality of life measured by the COPD assessment test (CAT) [14].
General care
During hospitalisation, the participants in both groups were given standard medical treatment for AECOPD, optimised prescribed medical treatment of COPD and were instructed in chest physiotherapy [15]. At 3 to 7 days after discharge, baseline spirometry (pulmonary function test (PFT)), Medical Research Council (MRC) dyspnoea scale, CAT, smoking status, ISWT and ESWT were recorded. Information on smoking cessation was given if relevant. Participants were introduced to a telephone hotline operated by a COPD nurse during office hours, where they could seek advice about their COPD. At 2 and 6 months after discharge, smoking status, MRC, CAT, PFT, ISWT and ESWT were recorded.
Early pulmonary rehabilitation group
After discharge, the participants were referred, according to their physical status, to either outpatient rehabilitation in the hospital or in the community or rehabilitation at home. Rehabilitation was initiated within 2 weeks after discharge.
The programme was a standardised 7-week programme with supervised training sessions, consisting of aerobic exercise and strength training twice weekly for 1.5 h and educational session once per week for 1 h. The programme fulfilled the criteria for pulmonary rehabilitation, according to the Danish Health Authority and the British Thoracic Society guidelines [16, 17]. The detailed description of the rehabilitation programme is provided in the supplementary material.
Stable pulmonary rehabilitation group
At the 2-month follow-up, participants in the stable pulmonary rehabilitation group were referred to a similar programme as undertaken by the early pulmonary rehabilitation group.
Study population
Eligible patients were included consecutively between 2013 and 2016 at the Department of Respiratory Medicine, Gentofte Hospital. Inclusion criteria were hospitalisation with an AECOPD, a diagnosis of COPD according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) [18], age >18 years, ability to walk 10 m independently (with or without a walking aid). Exclusion criteria were: life expectancy <6 months due to another disease (such as cancer or severe heart disease), difficulties in understanding and speaking Danish (e.g. due to dementia), residence outside Gentofte Hospital's recruitment area, discharge to a residence other than their own (e.g. nursing home), participation in another rehabilitation programme or inability to provide informed consent.
Figure 1 shows a flowchart with the description of the study design.

Flowchart of the study design. COPD: chronic obstructive pulmonary disease; PR: pulmonary rehabilitation; AECOPD: acute exacerbation of COPD; GOLD: Global Initiative for Chronic Obstructive Lung Disease; PFT: pulmonary function test; MRC: medical research council dyspnoea scale; ISWT: incremental shuttle walk test; ESWT: endurance shuttle walk test; CAT: COPD assessment test.
Statistical analysis
For the sample size calculation, we estimated 1-year mortality in patients without previous hospital admissions to be 15%, the expected reduction in mortality or readmission rate was set at 25% (power 80% and α=0.05) leading to a requirement of 112 participants (56 in each group). The effect size was estimated from the results of the Cochrane review in 2011 [11]. With an estimated dropout frequency of 20%, we recruited 150 participants. We used STATA 13 (STATA Corporation, College Station, Texas, USA) for the statistical analyses and analyses of the primary and secondary outcomes were performed according to the intention-to-treat principle.
Baseline characteristics were analysed with a Student's t-test or Mann–Whitney U-test for continuous data and Chi-squared or Fisher's exact test for categorical data. The primary outcome was analysed with Fine and Gray competing risk analysis with readmission as failure and death as competing risk. For secondary outcomes, we used logistic regression for mortality ratio and readmission ratio, log-rank test and Cox proportional hazards model for survival analysis, and negative binomial regression for relative risk of readmission between groups. Odds ratios (ORs), hazard ratios (HRs) and incidence rate ratios (IRRs) are shown with the control group as reference. Longitudinal data were analysed with a mixed-effects model for CAT, ISWT and ESWT, assuming values were missing at random.
Results
Baseline
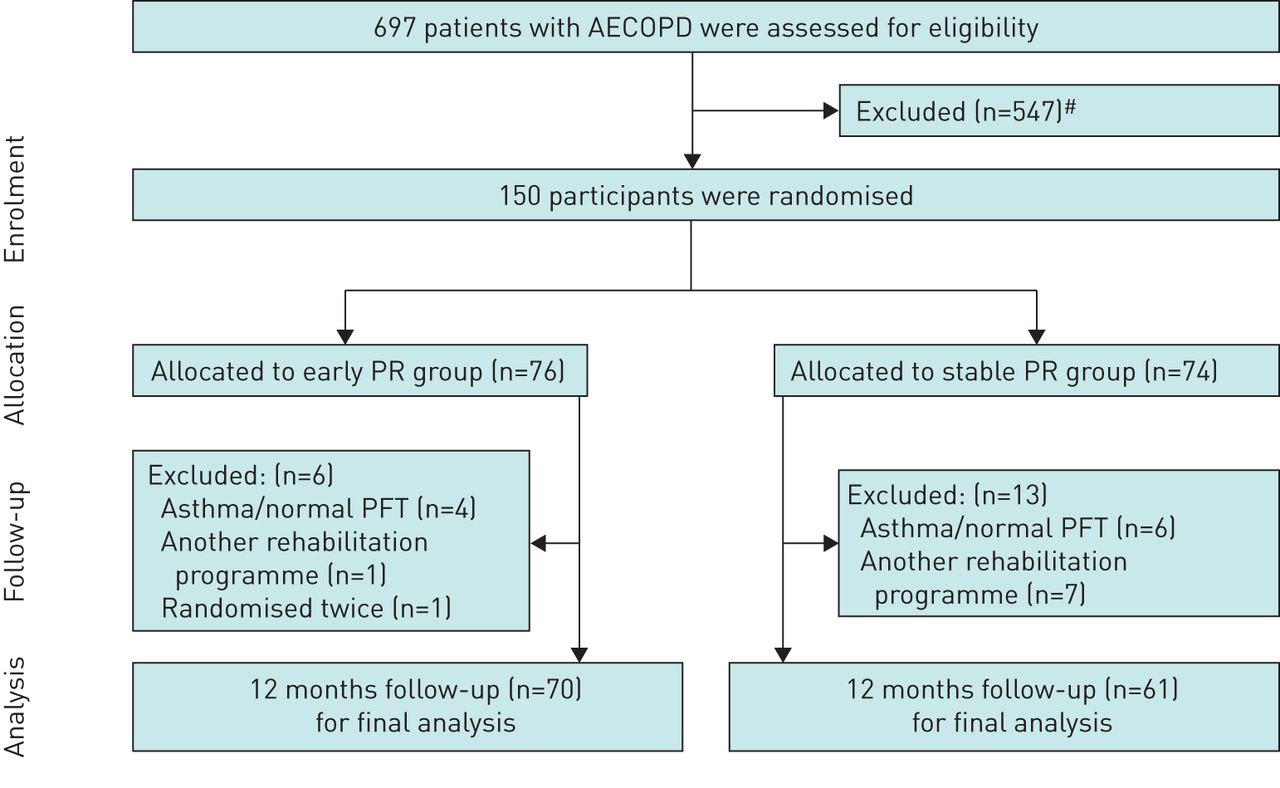
We screened 697 patients hospitalised with AECOPD over a 4-year period. We included 150 participants, with 76 in the early pulmonary rehabilitation group and 74 in the stable pulmonary rehabilitation group. The main reasons for non-inclusion were: declining to participate, estimated short life expectancy and participation in other rehabilitation programmes. Figure 2 shows a flow diagram of the progress throughout the study. One participant was randomised twice by mistake. During the 6-month follow-up period, 6 and 13 participants were excluded in the early and stable pulmonary rehabilitation groups respectively, mainly due to a diagnosis of asthma or start of another rehabilitation programme. This resulted in 70 and 61 participants in the early and stable pulmonary rehabilitation groups, respectively and all were included in the analysis of the primary end-point.

Screening, randomisation and study completion. AECOPD: acute exacerbation of chronic obstructive pulmonary disease; PR: pulmonary rehabilitation; PFT: pulmonary function test. #: excluded (n=547): declined to participate (n=125); death in hospital (n=30); life expectancy <6 months (n=134); other rehabilitation programme (n=126); living in nursing home (n=29); not COPD (n=30); residence outside Gentofte Hospital's admission area (n=73).
Baseline characteristics of the participants are presented in table 1 and showed a generally well-balanced randomisation and they resembles the general COPD population hospitalised with AECOPD in Denmark [19]. However, participants in the stable pulmonary rehabilitation group had a better CAT score.
Baseline characteristics
Adherence
In the early pulmonary rehabilitation group, 58 (83%) participants attended at least one rehabilitation session and 39 (56%) met our a priori definition of adherence (attendance >75% of sessions). The median time to the first session from discharge was 9 days (interquartile range (IQR) 5–15) with a median number of sessions of 13 (IQR 8–16). Forty-seven participants received rehabilitation at the hospital's facilities and five in the community. Six participants were initially trained in their own homes, but only for a few sessions and hereafter to complete the programme in the outpatient setup. In the stable pulmonary rehabilitation group, 32 (53%) had at least one rehabilitation session within 1 year after inclusion with a median number of sessions of 13 (IQR 10–16) and 21 (34%) participants were adherent. The participants in the early pulmonary rehabilitation group were significantly more adherent (OR 2.39, 95% CI 1.11–5.18, p=0.01).
Primary outcome
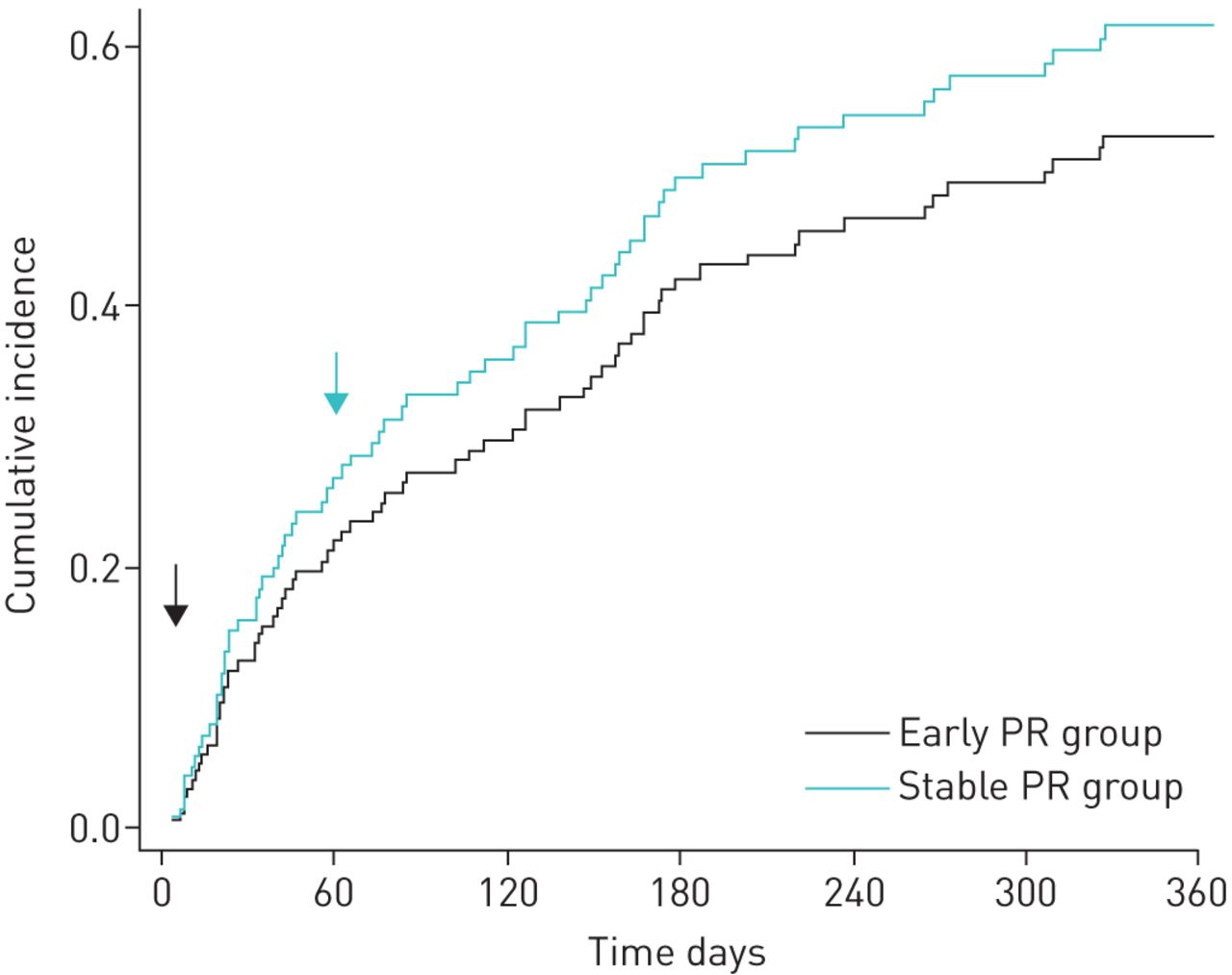
The primary outcome was a composite end-point of hospitalisation or death. In total, 78 participants (42 in the early and 36 in the stable pulmonary rehabilitation group) met this end-point. Except for one patient who died without previous hospital admission, all were readmitted at least once in the 12-month follow-up period. In the competing risk analysis, we found a crude nonsignificant risk (HR 1.03, 95% CI 0.66–1.60, p=0.91) and when adjusted for age, sex, forced expiratory volume in 1 s (FEV1), CAT and ESWT, there was a nonsignificant risk reduction (HR 0.79, 95% CI 0.47–1.23, p=0.33) (figure 3).

Cumulative incidence of hospital readmissions and mortality. Competing risk analysis (Fine and Gray) of hospital readmission with death as competing risk. Adjusted for age, sex, forced expiratory volume in 1 s and COPD Assessment Test. Hazard ratio 0.79 (95% CI 0.47–1.23), p=0.33. Arrows show the start of pulmonary rehabilitation (PR).
Mortality
Out of the 131 participants, 15 died during the study period, resulting in a 1-year-mortality rate of 11%. One person was hospitalised and died before the baseline visit, five died of COPD, four of cancer, three of cardiac causes, one of urosepsis and one of unknown cause. Nine participants died in the early pulmonary rehabilitation group (13%), and six (10%) in the stable pulmonary rehabilitation group. There were no significant differences between the groups with an adjusted OR of 1.05 (95% CI 0.33–3.40) p=0.92. A Kaplan–Meier plot of time to death is shown in figure 4 (log-rank test p=0.59) and using the Cox proportional hazard model, the adjusted HR was 1.04 (95% CI 0.36–3.01) p=0.95.

Mortality. Kaplan–Meier plot showing survival. Log-rank test p=0.59. Arrows show the start of pulmonary rehabilitation (PR).
Hospital admissions
During the 1-year follow-up period, 77 (59%) participants had a total of 218 readmissions due to any cause. In the early pulmonary rehabilitation group, 41 (59%) participants had 128 readmissions versus 36 (60%) in the stable pulmonary rehabilitation group having 90 readmissions. No significant reductions were found in participants with at least one readmission in the early pulmonary rehabilitation group, showing an adjusted OR of 0.57 (95% CI 0.25–1.31) p=0.19 and we observed no significant difference in the time to first hospitalisation, with an adjusted HR of 0.76 (95% CI 0.47–1.24) p=0.28. The number of admissions was also similar (IRR 1.04 (95% CI 0.66–1.65) p=0.85) in the two groups.
Sixty-two (47%) participants had 151 admissions (86 in the early, versus 65 in the stable, pulmonary rehabilitation group) due to a respiratory cause (e.g. AECOPD or pneumonia). We found no significant difference between the groups in participants with at least one respiratory readmission (adjusted OR of 0.66 (95% CI 0.27–1.37) p=0.31) and no difference in the time to respiratory readmission (adjusted HR of 0.78 (95% CI 0.43–1.24) p=0.35).
All analyses on mortality and readmission were adjusted for age, sex and baseline FEV1, CAT and ESWT and no interactions were found.
Exercise performance and quality of life
For physical performance and quality of life, there was significant improvement in both groups from baseline at 2 and 6 months (table 2). Although no statistical difference between groups was found at 6 months, the early pulmonary rehabilitation group gained 72 m in the ISWT at 2 months compared to the gain of 38 m in the stable pulmonary rehabilitation group. This resulted in a difference of 33.9 m (95% CI 4.2–63.7) p=0.02, which is below the minimal clinical important difference (MCID) of 47.5 m [20]. In addition, there were not a significantly greater number of participants who gained 47.5 m in the early pulmonary rehabilitation group (responders) (p=0.07). After 6 months, the difference in ISWT between the two groups diminished to 17.7 m (95% CI −13.3–48.7) p=0.26. There was a trend towards a larger improvement in ESWT in the early pulmonary rehabilitation group at 2 months (140.4 s (95% CI −2.0–282.8) p=0.05) but no difference at 6 months (24.3 s (95% CI −123.4–171.9) p=0.75). The MCID of 186–199 s was not reached [21].
Physical performance and quality of life
Health-related quality of life measured by CAT was not significantly different at either 2 months (−1.4 point (95% CI −3.4–0.6) p=0.17) or 6 months (−1.4 point (95% CI −3.5–0.6) p=0.18) (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Exercise capacity and quality of life. Functional measures in a) incremental shuttle walk test and b) endurance shuttle walk test, and c) quality of life in COPD Assessment Test at baseline, 2 months and 6 months follow-up. PR: pulmonary rehabilitation. *: p<0.05.
Discussion
This study demonstrated that initiating a standardised pulmonary rehabilitation programme shortly after hospitalisation due to severe AECOPD did not improve 1-year survival or reduce 1-year risk of hospital admissions compared to rehabilitation initiated during the later stable phase. Despite that, we found early pulmonary rehabilitation to have consistently greater benefit throughout the first 6 months of follow-up with regard to physical performance assessed by the shuttle walking tests, and additionally, the participants in the early pulmonary rehabilitation group had significantly higher adherence than those initiated their rehabilitation later. However, the differences between the groups regarding performance in the shuttle walking tests diminished after 6 months showing a nonsustained improvement.
In our study, the stable pulmonary rehabilitation group received the same rehabilitation as the early intervention group, only differing in timing. Only one study has previously compared early (within 2 weeks of an exacerbation) with late pulmonary rehabilitation (6 months after exacerbation) [22]. However, this study was underpowered due to recruiting issues, but the conclusion supported our results.
The result on primary outcome came out negative. However, the confidence intervals of the results were wide, suggesting limited confidence that the results confirm lack of effect. The sample size calculation was derived from the highly positive Cochrane review from 2011 on pulmonary rehabilitation in AECOPD, which today seems to have overestimated the effects. Estimated from our results, we would have had to include four times as many participants to see a significant effect of the intervention.
The updated Cochrane review from 2016, European Respiratory Society (ERS)/American Thoracic Society (ATS) guidelines on the management of COPD exacerbations and a systematic review by Ryrsø et al. [23, 24] concluded that early pulmonary rehabilitation implemented 3 weeks after discharge, reduced hospital admissions. But in contrast to these reviews, which compared early pulmonary rehabilitation to no rehabilitation, the present study compares early to late onset rehabilitation. Even though the readmission rate was high in our study, with 59% readmitted due to all causes during the 1-year observation period and 46% due to respiratory causes, we did not find a significant reduction in the risk of either readmissions or exacerbations. Previous attempts to explain divergent findings in earlier trials included lack of comprehensiveness in the rehabilitation programme [9, 25]. As our intervention fulfilled the criteria for a pulmonary rehabilitation programme according to general guidelines, we do not expect it as a likely explanation for our negative finding.
Further, we did not find reduced mortality, which aligns with the ERS/ATS guideline and Cochrane review [23]. The mortality in this study was notably low but this is mainly explained by the exclusion of patients who died in-hospital during admission for AECOPD and before inclusion in the present study.
With regard to exercise capacity, we found a significant improvement in incremental shuttle walk (ISWT) and borderline significance in endurance shuttle walk (ESWT) after 2 months in participants who recieved early pulmonary rehabilitation. However, both differences between groups are below the MCID [20, 21]. At 2 months, which was before initiation of stable rehabilitation, the stable pulmonary rehabilitation group did show a spontaneous large increase in exercise capacity in both ISWT and ESWT. An explanation for this could be natural recovery, which has been seen in previous studies, although not to the same extent [9, 26, 27]. The stable pulmonary rehabilitation group was not allowed to train elsewhere before the 2-month follow-up and seven participants in that group were excluded due to their participation in another rehabilitation programme. Further, the stable pulmonary rehabilitation group did unfortunately not gain the expected effects of the standard rehabilitation programme. This is probably explained by the low adherence to the rehabilitation programme. The early intervention group had an expected improvement in COPD assessment test, as seen in other trials but, as mentioned, we also found a large spontaneous recovery in the stable pulmonary rehabilitation group [28]. Surprisingly, we did not observe the expected worsening in quality of life after 6 months in the intervention group, as seen in other studies [14].
The current study was designed to emulate a regular clinical setting with patients referred to the same standard pulmonary rehabilitation programme as patients with stable COPD, so it would be feasible to implement in daily clinical practice. Uptake of early pulmonary rehabilitation was acceptable at 83% and the adherence was significantly higher in the early compared to the stable intervention group, which is probably explained by the participants' commitment to rehabilitation shortly after a hospitalisation. It was possible to refer patients to early pulmonary rehabilitation, but the challenge was to get them to attend the rehabilitation sessions, even though transportation to the rehabilitation centre was arranged for free.
A key limitation in the current study was the exclusion of eight participants during the study period, mainly due to misclassification of COPD (e.g. at follow-up, they presented a normalised spirometry or a substantial reversibility and thereby fulfilled criteria for asthma)
Another limitation was a similar recruiting problem as seen in other studies investigating the effect of rehabilitation in exacerbations of COPD [22, 29]. Hospital admissions due to exacerbation of COPD in Denmark usually last 3–4 days, and as the patients were asked to participate within the first couple of days after admission; rehabilitation may have seemed overwhelming, which made some patients decline participation, as also seen in other trials [30, 31]. This is a known problem when evaluating pulmonary rehabilitation in an acute setting and may results in a selection bias, making the included participants not representative of the general COPD population. The uptake of early rehabilitation needs to be investigated further especially in the most symptomatic patients (e.g. a referral visit within 1 week after discharge when the patients have recovered from the most severe part of the exacerbation).
Conclusion
We found that early pulmonary rehabilitation after severe exacerbation of COPD seems to accelerate the recovery of exercise capacity, assessed as ISWT, compared to pulmonary rehabilitation initiated later in the stable phase. In addition, we found that early pulmonary rehabilitation was safe and associated with higher adherence to the rehabilitation programme. However, we did not find any effect on mortality or hospital readmission rate.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00173-2019.SUPPLEMENT
Acknowledgements
the authors would like to thank our research and rehabilitation team: M. Rosenberg, A. Behring, P. Kjerrumgaard, H. Rohde, L. Dalhof and H. Riber. In addition, we acknowledge the support of the Department of Respiratory Medicine, Gentofte Hospital, Denmark and the Prevention Fund of the Capital Region in Denmark.
Footnotes
This article has supplementary material available from openres.ersjournals.com
This study is registered at www.clinicaltrials.gov with identifier number NCT02987439. The study group has a long history of data sharing. The data used for the current study will be made available to other researchers. However, the study group has the obligation to assure that data shared are handled in a way that complies with the science ethics permission and the General Data Protection Regulation. Apart from that, the study group has an ambition that data shared are used for sound scientific purposes by researchers. We encourage researchers who find interest in sharing our data, to contact the corresponding author. The corresponding author will then bring this request to the study group. Data will be shared if the abovementioned issues are assessed as compliant.
Author contributions: J.L. Kjærgaard, C.B. Juhl and J.T. Wilcke contributed to the design of the study and conception and acquisition of data. J.L. Kjærgaard and C.B. Juhl analysed data, and J.T. Wilcke provided statistical advice. All authors contributed to the writing of the manuscript, interpreted and critically revised the work. They all approved the final version and are accountable for their part of the work.
Conflict of interest: J.L. Kjærgaard has nothing to disclose.
Conflict of interest: C.B. Juhl has nothing to disclose.
Conflict of interest: P. Lange has nothing to disclose.
Conflict of interest: J.T. Wilcke has nothing to disclose.
Support statement: This study was supported by the Prevention Fund of the Capital Region in Denmark. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received July 11, 2019.
- Accepted December 11, 2019.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










