





Abstract
Introduction Nonadherence to treatment remains an obstacle to tuberculosis (TB) control worldwide. The aim of this study was to evaluate the feasibility of using video directly observed therapy (VDOT) for supporting TB treatment adherence in Uganda.
Methods From May to December 2018, we conducted a pilot cohort study at a TB clinic in Kampala City. We enrolled patients aged 18–65 years with ≥3 months remaining of their TB treatment. Participants were trained to use a smartphone app to record videos of medication intake and submit them to a secured system. Trained health workers logged into the system to watch the submitted videos. The primary outcome was adherence measured as the fraction of expected doses observed (FEDO). In a secondary analysis, we examined differences in FEDO by sex, age, phone ownership, duration of follow-up, reasons for missed videos and patients' satisfaction at study exit.
Results Of 52 patients enrolled, 50 were analysed. 28 (56%) were male, the mean age was 31 years (range 19–50 years) and 35 (70%) owned smartphones. Of the 5150 videos expected, 4231 (82.2%) were received. The median FEDO was 85% (interquartile range 66%–94%) and this significantly differed by follow-up duration. Phone malfunction, uncharged battery and VDOT app malfunctions were the commonest reasons for missed videos. 92% of patients reported being very satisfied with using VDOT.
Conclusion VDOT was feasible and acceptable for monitoring and supporting TB treatment. It resulted in high levels of adherence, suggesting that digital technology holds promise in improving patient monitoring in Uganda.
Abstract
Video directly observed therapy is feasible and acceptable for supporting and monitoring TB treatment adherence in a low-resource setting like Uganda. Digital health interventions hold promise as alternative methods for improving patient care. http://bit.ly/2Hxnvwu
Introduction
The End TB Strategy envisions a world free of tuberculosis (TB): zero deaths, disease and suffering due to TB by 2035 [1]. Nonadherence to treatment remains a major obstacle to TB control because it reduces cure rates, prolongs infectiousness and contributes to the emergence of acquired multidrug-resistant strains [2–5]. Nonadherence to treatment is a challenge particularly in sub-Saharan Africa, where TB rates can be as high as 800 per 100 000, yet resources for healthcare delivery are limited [1]. Adherence support and monitoring interventions improve TB treatment outcomes compared to unsupervised, self-administered treatment [5, 6]. Innovative approaches to improve care and prevention must be explored in order to make the goals of the End TB Strategy a reality [7].
Directly observed treatment (DOT) is a standard strategy that was established to ensure adherence to treatment in the early 1990s but proper implementation has proved difficult to achieve worldwide [6, 8]. In sub-Saharan Africa, the practice of DOT is limited by a severe shortage of healthcare workers coupled with weak public health systems in which most TB programmes operate [9, 10]. Previous studies in Uganda showed that only 16% of TB clinics implemented DOT properly due to a shortage of health workers [11]. Furthermore, only 63% of DOT workers consistently supervised treatment [12] whereas 26% of patients did not properly adhere to their prescribed treatment [13]. Community-based strategies to enhance the implementation of DOT have utilised volunteers, family members or patient peers as treatment supporters. However, the success of such DOT models remains limited by reliance on the efforts of unpaid workers [14, 15]. Studies show that nonadherence can be due to forgetfulness, a false perception of wellbeing, drug side-effects, stigma, long distances to health facilities coupled with long waiting times [16–21]. Novel alternative approaches that address these gaps are urgently needed.
In 2015, the World Health Organization established a Global Task Force on Digital Health for TB to support the development of digital health innovations to improve care and prevention [22, 23]. In 2017, video directly observed therapy (VDOT) was endorsed as an alternative to DOT for monitoring treatment where possible [7]. VDOT enables the patient to use a smartphone to record videos of their daily pill intake without face-to-face interactions with the health providers. VDOT can overcome the limitations of in-person DOT at the patient and health system levels. For example, VDOT studies have shown that the distance barrier is mostly eliminated [24–26], patients have greater autonomy to choose when and where to take their medications [25, 27], the costs of travel are minimised [24, 28], and providers can support a higher number of patients, thus increasing the health system efficiency [24, 29].
Previous studies in high-income [26, 27, 30–32] and low-income countries [9, 33] have reported high adherence and patient satisfaction with VDOT. One study from Kenya showed the promise of digital health interventions for supporting TB treatment success [34]; however, no published studies exist on the use of VDOT in Africa. The aim of this study was to determine the feasibility and acceptability of VDOT for monitoring and supporting treatment adherence in the Ugandan context.
Materials and methods
Study setting
Uganda is a unique setting for testing and adopting VDOT because it is classified as a high-burden country for TB and HIV, with an estimated 80 000 new TB cases each year according to the national prevalence survey [35]. By March 2018, the number of mobile phone users had increased to 24.8 million, representing a 71% cellular penetration rate, mostly concentrated in the cities [36]. Kampala City, Uganda's capital, is residence to ∼25% of TB patients. The TB Control Program is responsible for providing free diagnosis, treatment and case management services to all patients. Adherence monitoring and support are delivered mostly through community-based DOT by designated treatment supporters. The treatment supporters can be trained community health volunteers, family members or friends. TB medications are provided free of charge and patients are expected to return to the health clinics for monthly prescription refills until they complete the 6–8-month regimen for drug-susceptible disease.
Study design
We conducted a pilot prospective single-arm cohort study that included patients with active TB attending an outpatient clinic supported by the Uganda National TB Program in Kampala City. Eligible patients were 18–65 years old with confirmed drug-susceptible TB and had ≥3 months remaining to complete TB treatment. Patients were excluded if they had confirmed multidrug-resistant TB, or a documented cognitive, visual or motor disability that would interfere with recording videos. Patients were also excluded if they did not have access to electricity to charge a smartphone. Consecutive patients presenting at the clinic were invited to participate regardless of smartphone ownership (figure 1). Sample size determination was guided by pragmatic parameters such as cost and human resources. The main objective of the pilot was to determine feasibility and not to test a hypothesis; therefore, no power calculations were performed.

Flow diagram of video directly observed therapy (VDOT) procedures. TB: tuberculosis; PIN: personal identification number.
Description of VDOT System
Treatment monitoring was performed using an asynchronous VDOT. This involved a smartphone application (app) that enabled patients to record videos while swallowing each dose of medication and upload them to a secure cloud server to be accessed and viewed later by health workers. A detailed description of the app is published elsewhere [27, 32]. The app worked with an Android (Google LLC, Menlo Park, CA, USA) or iOS (Apple Inc., Cupertino, CA, USA) smartphone and time-stamped videos were automatically sent by the app through third- or fourth-generation (4G) cellular networks or Wi-Fi. The app prevents videos from being viewed, edited or deleted by users on the smartphone, thus ensuring confidentiality and fidelity of the videos. After successful upload, the videos are automatically deleted from the smartphone. Participants used either their own smartphone or were loaned a 4G smartphone by the study. Cellular internet data charges were prepaid weekly at ∼US$1.00 and sent directly to the participants' phone to ensure videos would be sent in a timely manner.
Study participants received automatic daily short text reminders 1 h before the scheduled medication doses and 1 h after only if a video was not received. Trained research staff logged into an internet-based, password-protected client management system to watch the uploaded videos and document whether they observed the pills being swallowed. A predefined protocol adapted from the TBeDOT toolkit published by the US Centers for Diseases Control and Prevention was followed [37]. If a video was not sent within 24 h, the research staff followed up with the participant by a phone call to ascertain if a medication dose was taken and to report reasons for failing to send the video, and provided necessary support.
Study enrolment procedures
Clinic nurse providers at the study site invited consecutive patients to participate in the VDOT pilot. Two trained research staff screened prospective participants for eligibility and enrolled them into the study. After the informed consent process and documentation, participants received VDOT training conducted in English or Luganda, and lasting ∼30 min. The participants were allowed to practice logging into the app using an assigned personal identification number, recording and submitting videos, and to ask questions. Participants received a packet with written instructions on how to use the VDOT app and a “pill mat” to help them organise their pills before making their videos. During follow up, retraining was provided to participants as needed in cases of difficulties with navigating the app.
Data collection and follow-up
A baseline interview was administered to collect information about participants' sociodemographics, phone ownership, previous experience with technology including smartphone, internet, taking photos or videos, and frequency of use in the last 3 months. Additional clinical information about date of diagnosis, duration on treatment and other medications was collected from the clinic records. Study participants returned to the clinic for their routine monthly visit to refill prescriptions, and for evaluation at 2, 4 and 6 months, per the standard of care. Exit interviews were conducted at the end of the observation period to evaluate satisfaction with VDOT and difficulties with using the VDOT system.
Ethical considerations
The study was approved by the institutional review boards at the University of Georgia, Athens, GA, USA (approval number STUDY00004974), and the Higher Degrees, Research and Ethics Committee at Makerere School of Public Health, Kampala (approval number 562) in Uganda. Participants provided written informed consent in their preferred language, either English or Luganda. Participants were reimbursed for an equivalent of US$3.00 at baseline and follow-up to cover travel expenses that were related to VDOT visits.
Statistical analyses
We reported baseline summary statistics including means, standard deviations, medians, interquartile ranges and percentages with 95% confidence intervals. Experience with using phone functions was assessed using a Likert scale from 1 to 10 (1: not all comfortable; 10: very comfortable) then responses were collapsed into three groups (8–10: very comfortable; 4–7: somewhat comfortable; 0–3: not comfortable) or not applicable if a person did not use the feature. The primary outcome was adherence measured as the fraction of expected doses observed (FEDO) through VDOT. FEDO has also been used in prior studies [32] because it allows for standardisation of adherence measurement when there are unequal observation periods across participants who are enrolled after initiating treatment. Doses were only counted as “taken” if the research staff observed all pills being swallowed in the video. In a secondary analysis, we evaluated differences in FEDO by sex, age, phone ownership and duration of observation. We also calculated the total observed and unobserved doses reported as self-administered treatment. Other outcomes included reasons for missed videos and participant satisfaction with VDOT at exit of the study. Data were analysed using STATA/SE 15.1 software (StataCorp, College Station, TX, USA).
Results
Participants’ baseline characteristics
Between May and December 2018, 68 patients were invited to participate, of whom nine were ineligible and seven refused. Of those who refused, two men did not have time or interest, one male student was attending boarding school where cell phones were prohibited, one woman could not record herself for religious reasons and three younger women needed to seek permission from family members who had provided them with the cell phones but never returned. Two female participants were withdrawn within 1 week of enrolment (one developed a mental illness and the other was a caregiver of a very sick child). 50 participants were included in the final analysis.
28 patients (56%) were male and the mean age was 31 years (range 19–50 years). Most (96%) owned cell phones and 35 (70%) owned smartphones. The VDOT app was installed on the personal smartphones of 21 (42%) patients and 29 (58%) used loaned study phones. Detailed baseline characteristics of study participants are shown in table 1.
Baseline characteristics of video directly observed therapy (VDOT) study participants (N=50)
Participants’ baseline experience with mobile phone technology
Nearly half (42%) of patients used a social networking site daily, 44% accessed the internet using a cell phone daily and 44% had used WhatsApp (Facebook Inc., Menlo Park, CA, USA). Overall, 78% were very comfortable making and receiving phone calls, 70% with texting messages, 72% with taking pictures and 50% with recording videos with the cell phone (results not shown).
Access to TB services, and concerns and preferences related to treatment at baseline
Most participants (54%) travelled by public transportation to the clinic and 34% experienced some difficulty with transportation (table 2). The mean cost for a round trip to the TB clinic was less than US$2.00, with a self-reported median travel time one-way of ∼30 min and a waiting time of 15 min. Patients expressed concerns about family members (36%) and neighbours or friends (50%) learning about their TB status. 82% of patients preferred phone calls as a way of communicating with the health providers.
Baseline access to tuberculosis (TB) services, and concerns and preferences related to treatment (N=50)
Adherence with VDOT and reasons for missed video submission
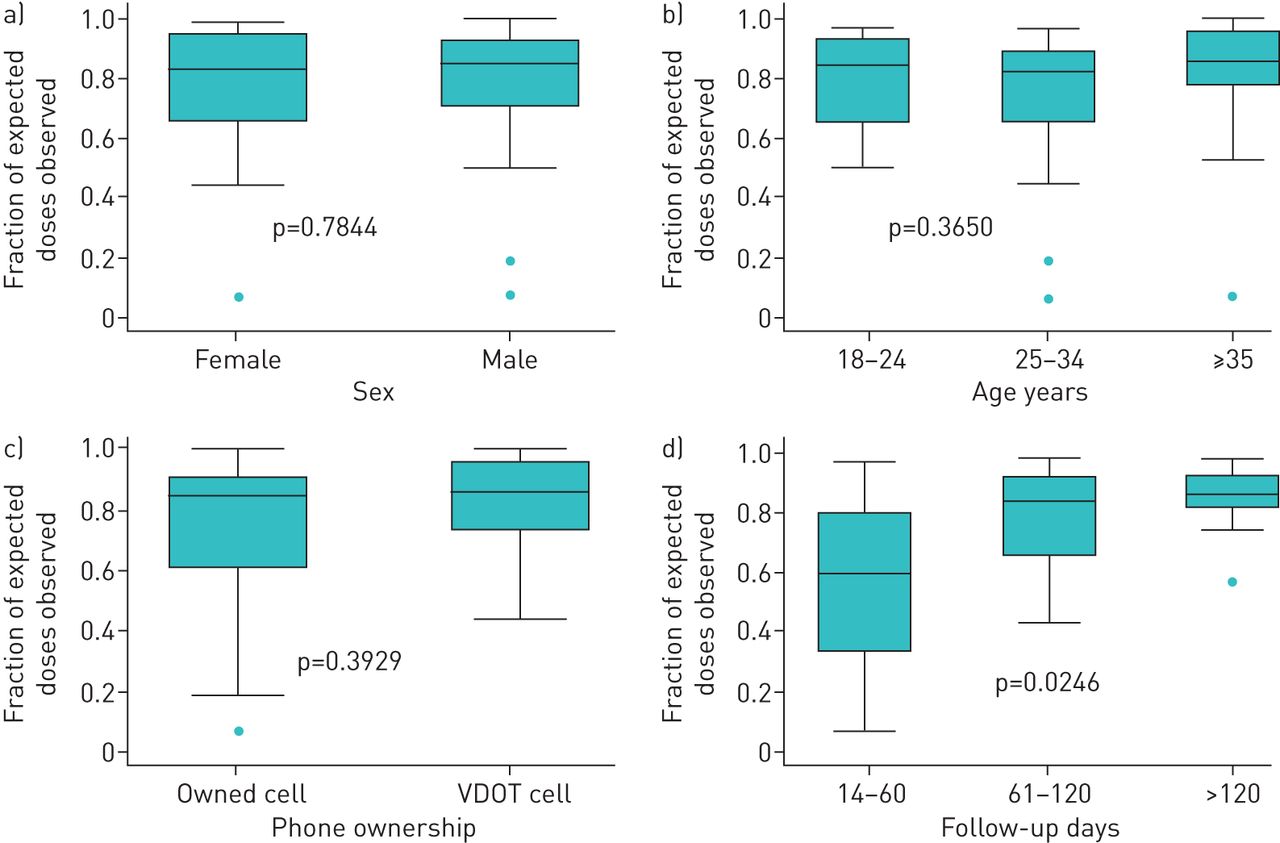
Cumulatively, 5150 videos were expected from participants during the study period and 4231 (82.2%) were received. The mean period of observation was 103 days (range 14–208 days). The median FEDO was 85% (table 3). Median FEDO did not differ significantly by sex, age group, or by phone status or phone use (loaned or personal) for VDOT. However, median FEDO significantly differed by duration of follow-up (p<0.05); the longer the duration, the higher the FEDO (figure 2).
Adherence to video directly observed therapy (VDOT) and reasons for missed video submission (N=50)
{kind=link}
{kind=link}
Boxplots of fraction of expected doses observed stratified by a) sex, b) age, c) phone ownership and d) follow-up duration. p-values based on Kruskal-Wallis test for comparison of medians. VDOT: video directly observed therapy.
Of the 919 missed videos, 541 (58.8%) represented doses that were not observed via video but were reported as self-administered treatment. The top three reasons reported by patients for missing video submission were phone malfunction (32%), dead phone batteries (24.2%) and possible technical problems with VDOT app (11%). Additional reasons for missed videos are shown in table 3.
Participants’ experiences with VDOT at exit of study
Overall, most participants favoured the use of VDOT for treatment monitoring. 98% were satisfied with using VDOT and 88% found VDOT easy to use while all participants said they would recommend it to other patients (table 4). More than half of the patients reported that they rarely or never experienced problems with the VDOT app or the cellular network while uploading videos. The majority (80%) shared their VDOT experience with family members and 38% with friends or workmates.
Participants' reported experiences using video directly observed therapy (VDOT) at exit of the study
Discussion
We found that VDOT was feasible and acceptable for monitoring TB treatment adherence in Kampala, Uganda, which is a high-burden setting. To our knowledge, there is no published study on the use of VDOT in this urban setting. Patients successfully recorded and submitted a high fraction of the expected videos to the VDOT system. Moreover, patients using VDOT were able to submit videos 7 days a week, including weekends, providing a more complete picture of medication dosing than the standard in-person DOT, which typically covers a 5-day period. A few prospective participants refused to enrol in VDOT for lack of time or needing to seek permission from other family members. We identified some technical challenges with smartphones and uncharged batteries leading to missed video submissions, but most participants were satisfied with using VDOT. These results are consistent with previous studies [27, 30–32, 38] and add to the evidence base that supports digital health as a promising intervention for supporting TB treatment in African settings [34].
In Uganda, adherence estimates, as measured by TB treatment completion rates, range from 67% to 77% according to the TB Control Program and health sector performance reports [39, 40]. In our study, the median FEDO of 85% using VDOT was similar to 88.4% reported by a study in Vietnam [9]. In contrast, a lower adherence of 74% was reported from a recent study in Kampala among patients attending two public TB clinics using standard DOT [13]. Other studies of VDOT in the USA, Mexico, Belarus and the UK showed adherence ranging from 77% to 98% among TB patients [26, 27, 31, 32]. The differences in adherence results between our pilot study and other VDOT studies could be explained by variations in technological infrastructure and population samples. To ensure nonadherence was addressed in a timely manner, the research staff assessed actual medication doses swallowed even when videos were not submitted. Importantly, we accounted for an additional 10% of doses that were self-administered, potentially increasing the estimated overall adherence to 92%. When using VDOT, the follow-up process could inherently improve patient–provider interactions and engagement beyond the routine observation [9].
The World Health Organization has updated TB treatment guidelines to include the use of digital health interventions such as VDOT as alternatives to in-person DOT when operational conditions are appropriate for healthcare providers and patients [7]. The baseline experiences with cell phones and the use of internet among participants show that this patient population was comfortable with the technology providing insights into future readiness for digital health interventions in Uganda. With the rapid expansion in mobile network coverage and smartphone ownership in resource-limited settings, such interventions are poised to become more feasible and scalable [41]. A key question that must be answered is: what will it cost to implement digital technologies? A study evaluating potential cost and impact of digital technologies for supporting TB treatment in high-burden settings projected up to 58% in cost savings when using medication monitors and video observed therapy [42]. But more studies on cost and cost-effectiveness of mobile technology interventions are needed to inform the local programme context. A preliminary cost analysis of the implementation of our VDOT pilot study is underway.
Stigma and privacy issues when using digital technologies in TB management are potential concerns that must be carefully considered [43]. In our study, patients reported that they were concerned about their family members, friends or neighbours finding out about their TB status, which could suggest underlying fear of being stigmatised. TB-associated stigma is a social determinant of health and has negative impacts on individuals including delays in seeking care, delays in TB diagnosis and nonadherence to treatment [44]. In relation to privacy, 18% of participants reported that they failed to record videos because of fear of being seen by someone. However, 78% perceived VDOT as more confidential than in-person DOT. In a similar VDOT study in California, USA, Garfein et al. [32] found comparable results, of 8% and 98% respectively, on the same issues. Although the evidence is limited, these findings may suggest that patients perceived using VDOT as more private as it relates to their TB status. This is consistent with a mixed-methods study by Wade et al. [38] in which most respondents felt that the videophone service improved patients' privacy.
For future adoption and scale-up of VDOT, TB programmes should address the main reasons that prevented video submission. For example, use of solar power banks or solar-powered smartphones could become future solutions to the problem of dead phone batteries. Phone malfunctions might have been due to the lower quality of cheap personal smartphones. TB programmes may need to set minimum requirements of the devices to be used for VDOT interventions. Despite some technological challenges, most participants were satisfied with using VDOT, suggesting that the benefits might have outweighed the difficulties faced from the patients' perspective. Previous studies indicate that a high level of patient satisfaction with services generally predicts high levels of adherence to TB treatment [45].
Our pilot results may not be generalised to the whole of Uganda because we used a convenience sample of participants at an urban TB clinic; nonetheless, we gained preliminary insights about feasibility of using of VDOT. Self-selection could have biased the results towards overestimation of adherence in our study. Due to limited resources, we did not evaluate important clinical outcomes such as sputum culture conversion and cure. However, it is reasonable to assume that better adherence should result in improved clinical outcomes. We cannot draw conclusions about effectiveness of VDOT since there was no control group. Therefore, comparative studies to evaluate efficacy of VDOT are logical next steps. Implementation research is needed to further understand potential barriers and facilitators for adoption or effective scale-up of digital health intervention in the context of local TB programmes.
Conclusions
VDOT was feasible and acceptable as a method of monitoring and supporting adherence among patients receiving TB treatment in urban Uganda. A relatively large proportion of the missed videos were due to technical malfunctions rather than a loss of patients' motivation to submit their videos of medication intake. Evaluating the implementation process of digital technologies in comparative studies is an important next step in strengthening TB patient care in low-resource settings [46].
Acknowledgements
We acknowledge the study participants and thank the research team members, Nicholas Kawuki, Joan Namatovu and Jonah Lubega at the Lubaga study site under Makerere University, Kampala, Uganda. We acknowledge the support of the Epidemiology in Action Research Group, collaborators at the University of Georgia (Christopher Whalen, Robert Kakaire and Paula Davis-Olwell) and Makerere University School of Public Health (Noah Kiwanuka). We thank Kelly Collins of SureAdhere Mobile Technology Inc. who provided training and technical assistance to the research team during the implementation of the VDOT system in Uganda.
Footnotes
Author contributions: J.N. Sekandi conceptualised and led the implementation of the study; S. Zalwango, E. Buregyeya, D. Nakkonde and J. Turinawe contributed to the design, data collection, analysis, interpretation and manuscript preparation. K.K. Dobbin, L. Atuyambe and R.S. Garfein contributed to conceptualisation, design, interpretation and manuscript preparation; S. Olowookere and E.G. Tucker contributed to data entry, analysis, interpretation and manuscript preparation; and S. Turyahabwe contributed to design, technical interpretation and manuscript preparation.
Conflict of interest: J.N. Sekandi has nothing to disclose.
Conflict of interest: E. Buregyeya has nothing to disclose.
Conflict of interest: S. Zalwango has nothing to disclose.
Conflict of interest: K.K. Dobbin has nothing to disclose.
Conflict of interest: L. Atuyambe has nothing to disclose.
Conflict of interest: D. Nakkonde has nothing to disclose.
Conflict of interest: J. Turinawe has nothing to disclose.
Conflict of interest: E.G. Tucker has nothing to disclose.
Conflict of interest: S. Olowookere has nothing to disclose.
Conflict of interest: S. Turyahabwe has nothing to disclose.
Conflict of interest: R.S. Garfein is a cofounder and the Chief Science Officer of SureAdhere Mobile Technology, Inc.
Support statement: This study was funded by the University of Georgia's Global Research Collaboration Grant, Office of Global Engagement and the Office of the Vice President for Research. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received July 12, 2019.
- Accepted February 11, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










