





Abstract
Introduction Cervical lymphadenopathy in lung cancer indicates advanced disease. The presence of mediastinal lymphadenopathy is commonly associated with involvement of neck lymph nodes and some studies suggest routine neck ultrasound (NUS) in this group of patients. We conducted a two-phase study looking at training a respiratory physician to perform ultrasound-guided neck lymph node aspiration in patients with suspected lung cancer.
Methods In the first phase of the study, one of the authors underwent training in NUS according to predetermined criteria. The adequacy of sampling was prospectively recorded. In the second phase, consecutive patients with suspected lung cancer and mediastinal lymphadenopathy underwent NUS and sampling of abnormal lymph nodes. The outcomes were the adequacy of samples for pathological analysis and molecular analysis, prevalence of cervical lymphadenopathy, and change in stage.
Results Following the period of training, 35 patients underwent neck node sampling with an overall adequacy of 88.6% (95% CI 78.1–99.1%). Cervical lymph node involvement was confirmed in 13 out of 30 patients with lung cancer (43.3%, 95% CI 25.5–62.6%). Further immunohistochemistry and molecular studies were possible in all patients when it was required (nine cases). NUS led to nodal upstaging in four out of 30 (13.3%) cases.
Conclusion Training a respiratory physician to perform NUS and needle sampling to an acceptable level is feasible. Benefits of embedding this procedure in lung cancer diagnosis and pathway staging need to be explored in further studies.
Abstract
It is feasible to train respiratory physicians to perform ultrasound-guided sampling of cervical lymph nodes. In lung cancer patients with mediastinal lymphadenopathy, 43% had cervical lymph node involvement with reduction in the number requiring EBUS. http://bit.ly/33LekBa
Introduction
Lung cancer prognosis and mortality remain poor, as currently >60% of patients present with advanced disease (stage IIIB or IV), where the only treatment options are noncurative systemic drug therapies and/or radiotherapy [1]. Accurate staging is required to inform on management, with respiratory physicians being the key interface, as the receivers of referrals and as part of the multidisciplinary teams. Furthermore, an expedited diagnostic and staging process is needed to avoid any deterioration in the functional status of patients rendering them unfit for treatment. To achieve such an expedited pathway where possible, the safest, highest yield diagnostic procedure should be performed to achieve both a diagnosis and a stage while providing enough tissue for analysis for targeted treatments such as immunotherapy and tyrosine kinase inhibitors [2].
Cervical lymph nodes are frequently involved in lung cancer [3]. The presence of cervical lymphadenopathy in patients with lung cancer is consistent with N3 or M1b disease depending on which level is involved, with significant impact on prognosis [4]. Clinical examination is unreliable, while staging computed tomography (CT) scans may not include the full neck in some centres [5]. Ultrasound examination confers the optimal assessment. Among patients with mediastinal lymphadenopathy, cervical lymph nodes were found to be involved in up to 50% of cases [6], leading to some guidelines recommending neck ultrasound (NUS) in patients with suspected lung cancer and bulky mediastinal lymphadenopathy [2]. Cervical node disease might also impact the radiotherapy planning fields and their involvement should therefore be accurately determined in such circumstances.
Needle sampling of cervical lymph nodes under direct ultrasound guidance is a safe and low-cost option. However, access to radiology for such a procedure might limit its time-saving value as a part of the diagnostic pathway. The literature supports the performance of such procedures by nonradiologists [7, 8], but no prospective studies have been performed for respiratory physicians and nor is training standardised. In this study, we aimed to prospectively assess the feasibility of training a respiratory physician to perform routine NUS and subsequent needle sampling of lymph nodes among patients with suspected lung cancer and mediastinal lymphadenopathy before endobronchial ultrasound (EBUS).
Methods
This was a prospective study conducted in Galway University Hospital (Galway, Ireland). The study was conducted in two phases. In the first phase, one of the authors (M.A.) was trained in performing NUS and cervical lymph node sampling, and sampling adequacy was recorded prospectively. This author had Level 1 Royal College of Radiologists training and limited experience performing EBUS when the study was commenced. In the second phase, a prospective study of NUS in patients with suspected lung cancer and mediastinal lymphadenopathy was conducted.
Phase 1: training the respiratory physician in NUS and needle sampling
Training in NUS and lymph node sampling was performed in a tertiary lung cancer centre (University Hospitals Plymouth NHS Trust, Plymouth, UK) supported by a fellowship from the European Respiratory Society under supervision of a respiratory physician (C.D.) with 5 years of experience in NUS and lymph node sampling.
The training structure was divided into five blocks. 1) Supervised NUS examination, including a predetermined number of normal and abnormal NUSs and achieving specified competencies requiring identification of normal and abnormal structures in the neck as outlined in table 1. 2) Attendance at the neck lumps clinic led by radiologists and ear, nose and throat surgeons, and observing procedures. 3) A period of observation in the pathology department to further understand the optimal sampling requirements. 4) Use of simulation tools (gelatine model with node-like structures for real-time ultrasound guidance practice). 5) Supervised neck node sampling with use of needle/core needle handling further supported by D.B.
Requirements for neck ultrasound (NUS) training: procedure numbers and competencies to be acquired
List of equipment used for ultrasound-guided needle sampling of cervical lymph nodes
The duration of training was 8 h per week for 10 weeks. Competencies listed in table 1 were assessed at the end of the training period. A prospective record of all NUS and needle sampling procedures performed was kept, including the adequacy and diagnostic yield of all samples over time.
Phase 2
Setting
In Galway University Hospital, all patients referred with suspected lung cancer are assessed in the interventional respiratory unit through a rapid access service. All patients have thorax and upper abdomen CT with contrast followed by further workup according to CT findings, but a diagnostic procedure such as bronchoscopy, EBUS or pleural fluid sampling is usually performed on the same day as CT in most patients. Positron emission tomography (PET) was done for patients with evidence of potentially curable disease on initial CT.
Patients
All consecutive patients with suspected and later confirmed primary lung cancer and evidence of mediastinal lymphadenopathy on CT that were referred to the interventional respiratory unit in Galway University Hospital were approached to participate in the study. Written informed consent was obtained. Exclusion criteria included age <18 years, history of any malignancy apart from nonmelanoma skin cancer and inability to give informed consent. Mediastinal lymphadenopathy was defined as a short diameter on CT of ≥10 mm.
Procedures
Neck ultrasound
A NUS was performed in all patients included. The ultrasound examination was performed with patients lying in a semisupine position using a linear ultrasound probe with a frequency of 5–12 MHz using one of two machines: Zonare Z.One Ultra (Zonare, Mountain View, CA, USA) or Hitachi EUB-7500A (Hitachi, Tokyo, Japan). Initially, the thyroid isthmus was identified and, once visualised, the probe was moved laterally to identify the carotid artery and internal jugular vein. The probe was then oriented horizontally and moved to assess the anterior cervical chain, and this was again repeated with the probe oriented vertically. The posterior cervical chain was then assessed before finally assessing the supraclavicular fossa. The same was repeated for the contralateral neck. The lower cricoid border was used as the landmark to differentiate N3 and M1 lymph nodes.
Needle sampling
If any neck lymph nodes were identified, these were further assessed for size, shape, hilar structures and necrosis. Lymph nodes with a short axis >5 mm were considered targets for sampling, and nearby vascular structures and location relative to the pleural lining were considered before proceeding. Sampling was performed under direct ultrasound visualisation following informed written consent. The equipment used in the sampling kit is outlined in table 2. The area was cleaned using chlorhexidine wash and 1% or 2% lidocaine was applied intradermally and subcutaneously to provide local anaesthesia. A sterile sheath was applied to the ultrasound probe. Under direct ultrasound guidance, a 22G needle was used to obtain samples. The first pass was used to make slides and two or three further passes were performed with samples sent in a formalin container. If well tolerated and technically feasible, two or three core needle biopsies (CNBs) were obtained from lymph nodes using an 18G SuperCore needle (Aragon Medical Devices, Frisco, TX, USA) with all material sent in a formalin container.
Lung cancer workup
As this was a pilot study, all lung cancer workup was continued as standard unless the results from neck lymph node sampling came back positive before a planned diagnostic procedure, in which case this was cancelled. This meant that based on the setting in Galway University Hospital it was expected that some patients would have both EBUS- and NUS-guided sampling performed in the same session.
Outcomes
The primary outcomes of interest in the study were 1) the diagnostic yield of malignant cervical lymphadenopathy defined as pathological evidence of cancer in neck lymph node samples consistent with a lung primary and 2) adequacy of needle sampling. Secondary outcomes included 1) patient-reported experience assessed by a visual analogue of discomfort associated with needle neck sampling and EBUS, and 2) the proportion of patients that had nodal upstaging. Patients who underwent both EBUS- and NUS-guided needle sampling were asked which procedure they preferred and why. The suitability of neck samples for molecular analysis when indicated was also reported. Potential complications of needle sampling (significant bleeding requiring prolonged compression and infection) were also recorded.
Statistical analysis
Categorical variables are reported as frequencies and percentages with associated 95% confidence intervals; continuous variables are reported as mean and standard deviations or median and interquartile range. Cumulative sampling adequacy rate is reported as percentage over time. A p-value of <0.05 was considered significant. Minitab 18 (Minitab, State College, PA, USA) was used to conduct the statistical analysis. As this was a pilot study, sample size was not calculated.
Ethics and trial registration
The study was approved by the Galway University Hospital research ethics committee (approval 54/08) and registered at ClinicalTrials.gov with identifier number NCT03970564.
Results
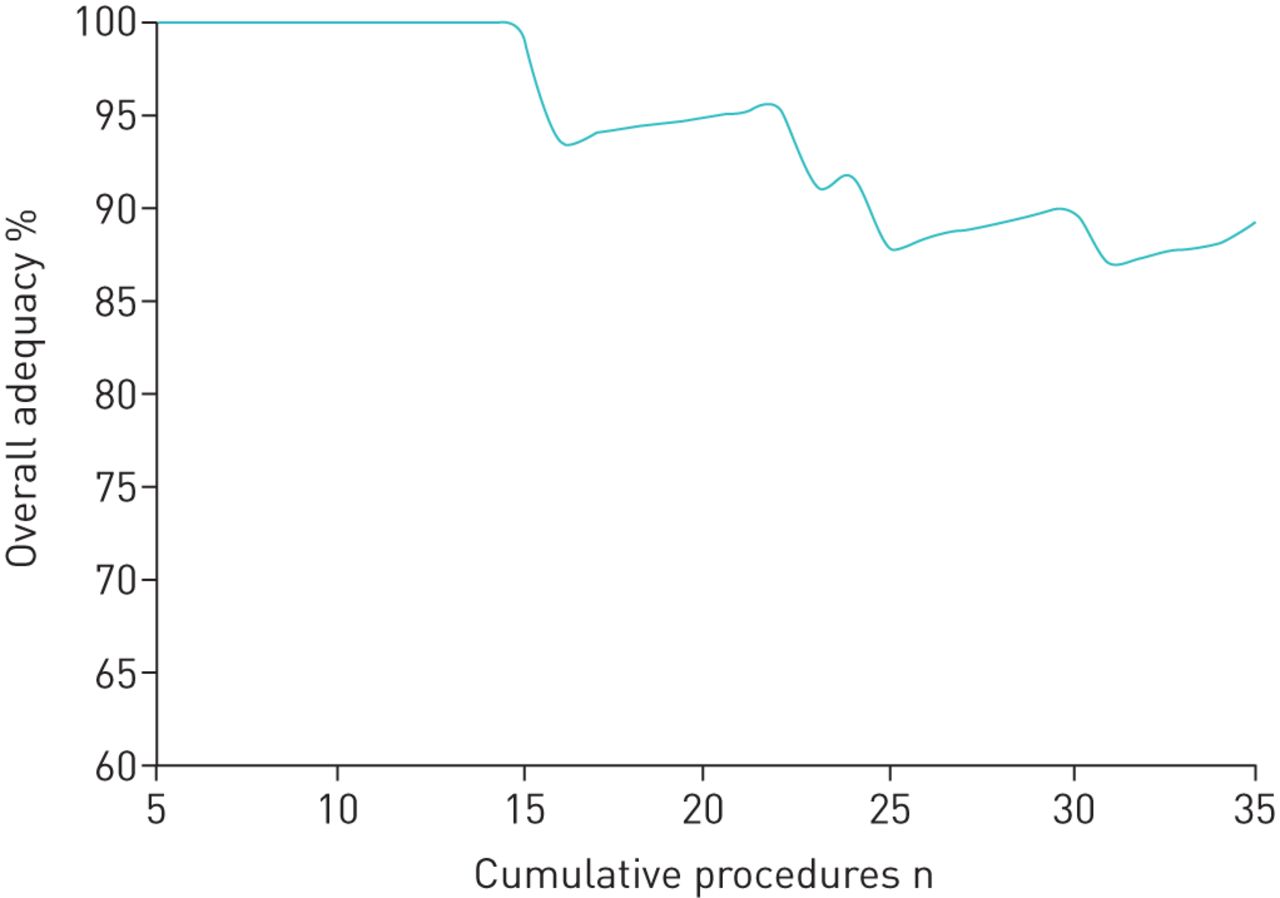
Training commenced in NUS in October 2016 and the study was completed in May 2018. During this period, 146 NUSs were performed with 35 needle sampling procedures in 28 patients. Fine-needle aspiration (FNA) was performed in all 28 cases and CNB in seven (25%) cases. The overall sampling adequacy was 88.6% (95% CI 74.1–95.5%) (FNA 89.7% versus CNB 85.7%; p=0.76). Figure 1 shows the cumulative overall sampling adequacy over time. No adverse events were reported for any of the procedures.

Cumulative adequacy of cervical lymph node sampling over time.
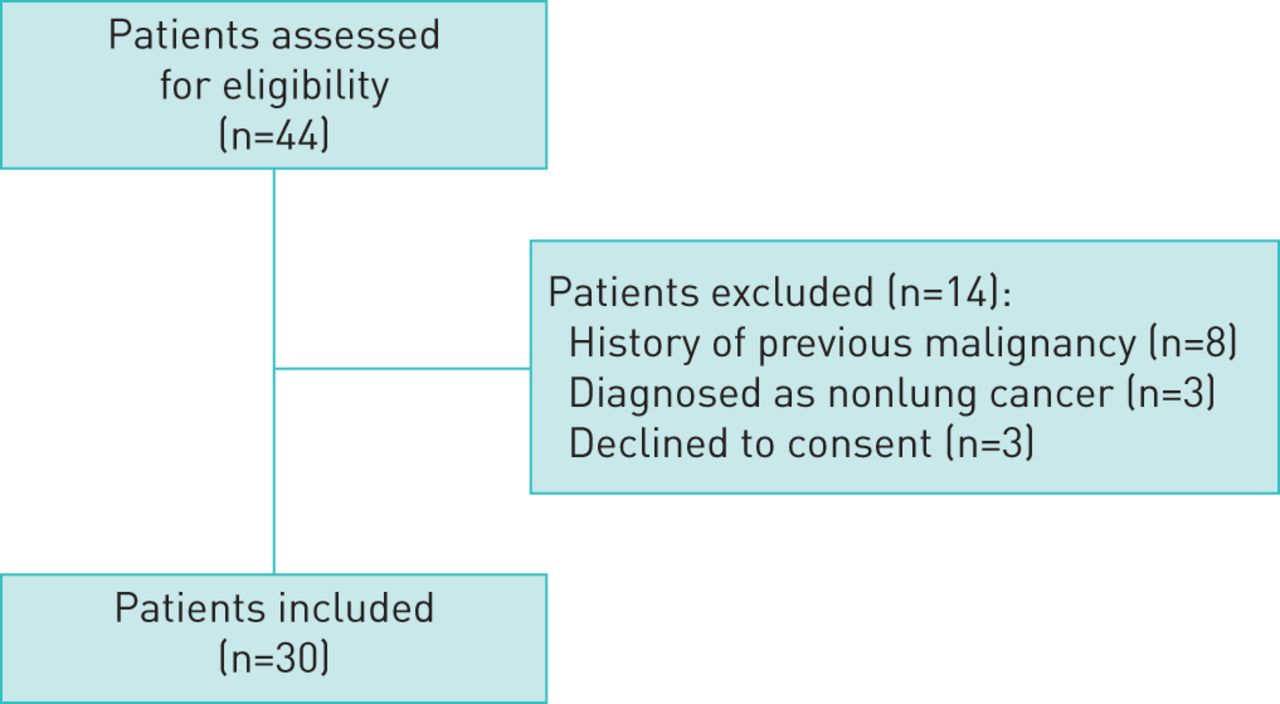
During the second phase of the study (February 2017–May 2018), 44 patients meeting the inclusion criteria were identified; 30 were included in the final study analysis (figure 2). Among those included, 76.7% (n=23) were referred through the rapid access clinic, while 23.3% (n=7) presented through the emergency department. Table 3 shows the baseline characteristics of all patients included and the clinical stage on the initial CT.

{kind=link}
{kind=link}
Participation flowchart detailing breakdown of patients assessed for inclusion in the second phase of the study.
Baseline characteristics of all patients included in the second phase of the study
Enlarged cervical lymph nodes were detected in 14 out of 30 (46%) patients and sampling was performed in all cases. Sampled material was adequate in 13 out of 14 (92.9%) cases. A diagnosis of metastatic cervical lymphadenopathy from lung cancer was confirmed in 13 out of 30 (43.3%, 95% CI 25.5–62.6%) cases. Mean lymph node short diameter was 11±4 mm. All lymph nodes were located below the cricoid cartilage. Location of lymphadenopathy in the 13 cases was right side in six cases, left side in one case and bilateral in six cases. Immunohistochemistry was possible in all samples. No significant complications were reported after any of the procedures. PET-CT was performed in 13 out of 30 (43.3%) cases. In this group that had PET-CT, six out of 13 cases had evidence of cervical lymphadenopathy and four out of six cases were confirmed on ultrasound-guided FNA with a false-positive rate for PET of 33.3%. PET-CT was not associated with any false negatives.
Molecular analysis was requested on six samples from patients with adenocarcinoma and was possible in all cases. Testing for programmed death ligand-1 was also requested and performed in three cases.
Performing NUS led to upstaging the clinical nodal status from cN2 to cN3 in four cases (13.3%). Overall, NUS-guided lymph node sampling was the only procedure performed to obtain tissue in seven out of 30 (23.3%) cases, but four out of seven (57.1%) in those presenting through the emergency department. Other procedures to obtain tissue samples were performed in 23 out of 30 (76.7%) patients, including EBUS in 17 cases, bronchoscopy in five cases, pleural tap in one case and mediastinoscopy followed by surgical resection in one case.
Data on patient experience were available for only six patients who underwent both neck lymph node sampling and EBUS in the same session. When asked in the recovery room which procedure would the patient prefer, four picked neck lymph node sampling compared with two that picked EBUS. All patients reported they would definitely be willing to return for both procedures if required.
Discussion
In this prospective study, we showed that it is feasible to train a respiratory physician to perform ultrasound-guided cervical lymph node needle sampling and maintain an acceptable level of sampling adequacy. At no stage did the cumulative sampling adequacy fall below 85%, which is the recommendation made by the Royal College of Radiologists for nonradiologists performing ultrasound-guided neck sampling [9]. The overall sampling adequacy was 88.6% and adequacy for FNAs was 89.7%. Sampling adequacy did seem to fall initially, likely due to sampling of more challenging lymph nodes over time.
The study showed a significant proportion of patients with lung cancer and mediastinal lymphadenopathy also had cervical lymph node involvement when NUS was performed routinely by a trained respiratory physician. The proportion of patients that had cervical lymph node involvement in the study was 43.3%, consistent with similar previous studies. Kumaran et al. [6] performed routine NUS conducted by radiologists in 101 patients with suspected and later on confirmed lung cancer, and found evidence of cervical lymph node involvement in 50% of cases, with nine out of 101 (9%) patients upstaged from radiographical N2M0 to N3M0 disease. A comparison of routine neck CT, ultrasound and palpation for the detection of cervical lymphadenopathy in 50 patients with lung cancer regardless of nodal stage on CT confirmed malignant cervical lymphadenopathy in 40% [3].
Ultrasound-guided cervical lymph node sampling is appealing as a procedure to be embedded in the diagnostic and staging pathway for lung cancer patients, especially if done by respiratory physicians. This can be considered as a test of choice following discussion at a diagnostic multidisciplinary team meeting when planning investigations for patients with suspected lung cancer on an individual basis, especially in cases with borderline performance status. Such a procedure can be performed in the clinic, does not require sedation with the logistic implications of a recovery time and is cheaper compared with other nodal staging procedures, e.g. EBUS and mediastinoscopy. In addition, a previous study showed PET-CT had only limited added staging benefit when done following NUS in patients with at least N2 disease on CT scan [10].
Within this study, six patients underwent both EBUS- and NUS-guided FNA in the same session, and there was no difference in the level of discomfort reported for the two procedures or the level of willingness to return for a repeat procedure was high (although the study was not powered to detect a difference in patient-reported outcomes between the two procedures). Further molecular studies were possible in all cervical lymph node samples when this was required, supporting the findings in a previous retrospective study of 171 cervical lymph nodes sampled from patients with lung cancer where further molecular studies were feasible in 85% of cases [11].
The study had some limitations. As this was a study with one operator, it is not possible to say whether the results were generalisable. Factors that might affect sampling adequacy such as lymph node size were not accounted for. The study was not designed to assess the impact of routine NUS on the average time to a final diagnosis/stage and this will need to be examined prospectively in a randomised study.
This study demonstrates the feasibility of training respiratory physicians to perform ultrasound-guided cervical lymph node sampling to an acceptable standard. Based on this study and previous literature, we recommend considering NUS through a multidisciplinary meeting in a selected group of patients, but not routinely. At this time PET-CT would likely be part of that decision making. Embedding routine NUS performed by respiratory physicians in the pathway of investigating patients with suspected lung cancer can potentially lead to more accurate staging in addition to time and cost savings, but this will need to be examined in further studies, which will likely include PET-CT as part of the algorithm
Footnotes
This study is registered at ClinicalTrials.gov with identifier number NCT03970564.
Support statement: M. Ahmed acknowledges receipt of support from the European Respiratory Society (fellowship STRTF 2016-7508). Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: M. Ahmed has nothing to disclose.
Conflict of interest: C. Daneshvar has nothing to disclose.
Conflict of interest: D. Breen has nothing to disclose.
- Received July 19, 2019.
- Accepted November 27, 2019.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










