





Figures
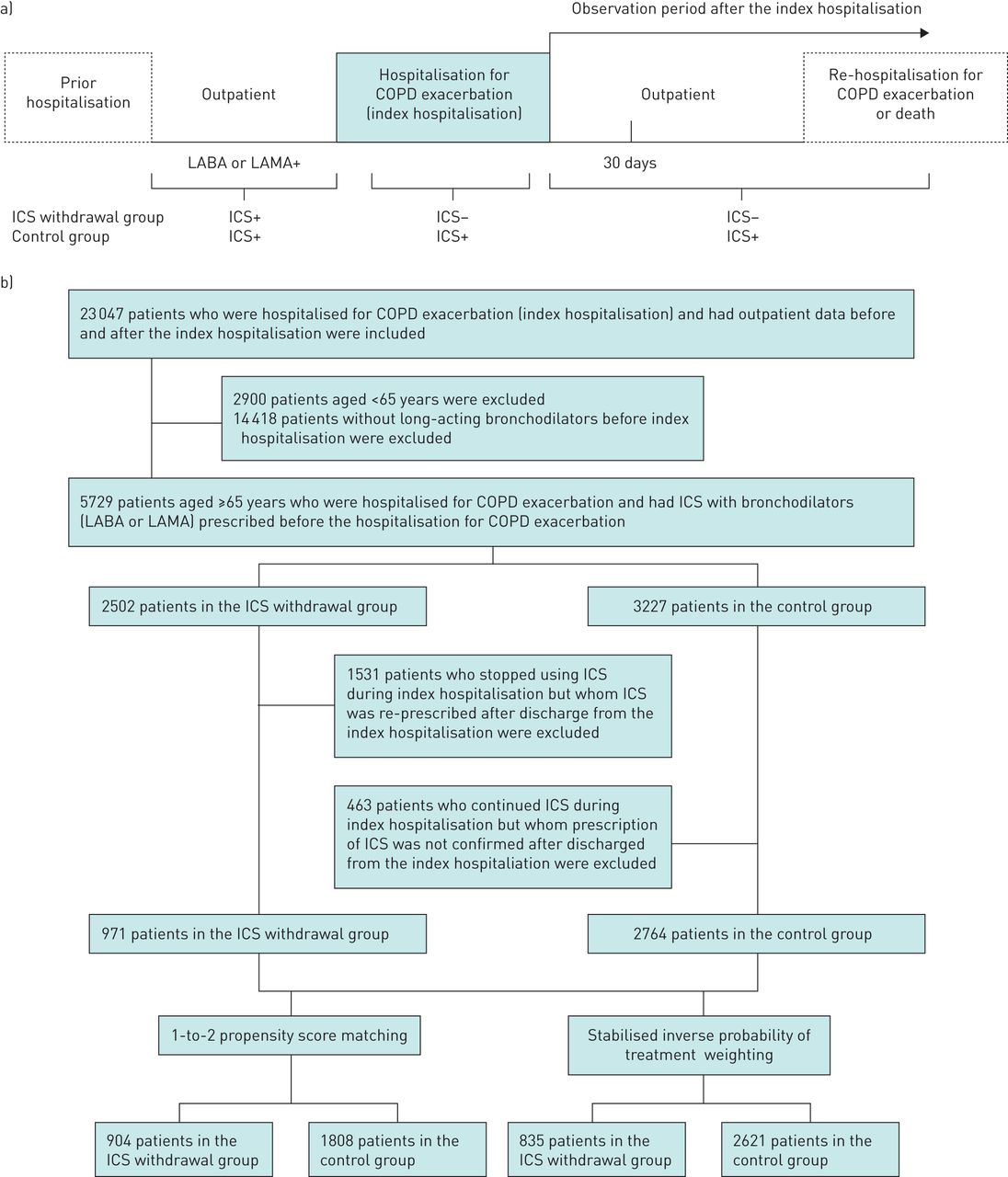
- FIGURE 1
Schematic diagram of study groupings. a) Study schematic showing each period evaluated in the study. Variables defining patient characteristics and comorbidities were obtained from the hospitalisation for COPD exacerbation, outpatient data, and data from prior hospitalisations. The outcomes were re-hospitalisation or death and incidences of prescriptions at 30 days and 1 year after the hospitalisation. The ICS withdrawal group was identified by discontinuation of the prescription during and after the hospitalisation for COPD exacerbation. b) Flow diagram of the study patients. LABA: long-acting β2-agonist; LAMA: long-acting muscarinic antagonist; ICS: inhaled corticosteroid.
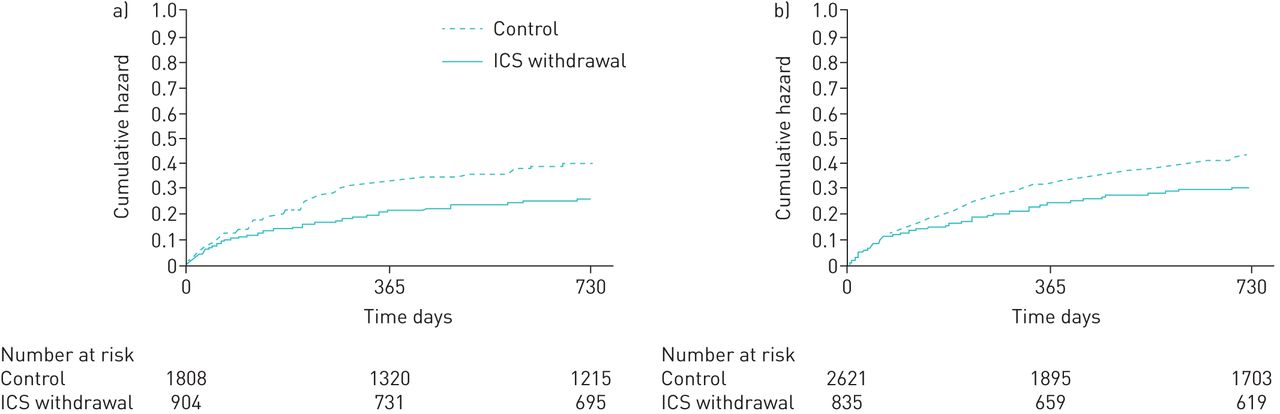
- FIGURE 2
Cumulative hazard curves for hospitalisation for re-exacerbation or death after hospitalisation for exacerbation in patients with chronic obstructive pulmonary disease (COPD) aged ≥65 years with or without inhaled corticosteroid (ICS) withdrawal. Results for a) 1–2 propensity score-matched population; and b) stabilised inverse probability weighted population.

{kind=link}
{kind=link}
Tables
- TABLE 1
Baseline characteristics of patients with COPD with and without inhaled corticosteroid (ICS) withdrawal, before and after 1–2 propensity score (PS) matching and after stabilised inverse probability weighting (IPTW)
Characteristic All patients 1–2 PS matching Stabilised IPTW ICS withdrawal (n=971) Control (n=2764) smd ICS withdrawal (n=904) Control (n=1808) smd ICS withdrawal (n=872) Control (n=2591) smd Males 84.0% 79.0% −12.9% 84.0% 82.0% −5.6% 80.0% 81.0% 0.7% Fiscal year 2010 4.1% 10.1% −23.6% 4.1% 3.9% 1.1% 7.3% 8.3% −3.4% 2011 9.4% 17.0% −22.6% 9.4% 8.7% 2.5% 16.8% 14.6% 6.0% 2012 13.8% 20.2% −16.9% 13.8% 12.9% 2.8% 18.7% 17.8% 2.4% 2013 18.3% 18.4% −0.4% 18.3% 20.7% −6.3% 16.3% 18.6% −5.9% 2014 25.0% 19.9% 12.4% 25.0% 25.2% −0.5% 21.4% 22.2% −1.9% 2015 29.4% 14.5% 36.8% 29.4% 28.6% 1.8% 19.4% 18.6% 2.1% Season at admission Spring 23.7% 24.9% −2.8% 23.7% 24.3% −1.4% 23.6% 24.0% −1.0% Summer 24.4% 22.2% 5.4% 24.4% 25.1% −1.5% 23.3% 23.3% 0.1% Autumn 24.4% 23.1% 3.1% 24.4% 24.8% −0.8% 24.2% 24.2% 0.1% Winter 27.4% 29.8% −5.3% 27.4% 25.8% 3.6% 28.9% 28.5% 0.8% Residential region Hokkaido and Tohoku 10.1% 10.6% −1.8% 10.1% 10.2% −0.5% 8.8% 10.8% −6.6% Kanto 30.6% 35.6% −10.6% 30.6% 29.9% 1.7% 36.2% 34.1% 4.5% Chubu 15.7% 15.7% 0.0% 15.7% 14.8% 2.5% 13.9% 15.2% −3.7% Kansai 16.0% 16.0% 0.2% 16.0% 16.1% −0.2% 14.6% 15.4% 2.1% Chugoku, Shikoku, Kyushu and Okinawa 27.5% 22.0% 12.8% 27.5% 29.0% −3.2% 26.4% 24.5% 4.3% Hugh–Jones dyspnoea score at admission 1 10.8% 9.5% 4.3% 10.8% 11.2% −1.2% 9.6% 9.5% 0.2% 2–3 33.7% 32.2% 3.2% 33.7% 30.9% 6.0% 32.7% 32.7% 0.0% 4–5 45.7% 51.8% −12.3% 45.7% 48.2% −5.1% 50.9% 50.3% 1.2% Missing 9.7% 6.4% 12.2% 9.7% 9.6% 0.4% 6.8% 7.5% −2.6% ADL at admission (Barthel Index score) 100 37.1% 37.9% −1.7% 37.1% 35.0% 4.3% 35.4% 37.4% −4.1% 0–90 49.0% 46.4% 5.2% 49.0% 50.8% −3.7% 48.4% 47.6% 1.5% Missing 13.9% 15.7% −5.0% 13.9% 14.2% −0.6% 16.2% 15.0% 3.4% ADL at discharge (Barthel Index score) 100 55.4% 62.4% −14.3% 55.4% 53.4% 4.1% 57.8% 59.8% −4.0% 0–90 36.0% 29.8% 13.2% 36.0% 36.7% −1.6% 34.7% 31.9% 6.1% Missing 8.6% 7.8% 3.1% 8.6% 9.9% −4.4% 7.4% 8.3% −3.2% Smoking index 200–599 9.0% 9.8% −2.8% 9.0% 7.5% 5.2% 8.9% 9.3% −1.2% ≥600 49.4% 48.3% 2.3% 49.4% 49.8% −0.7% 48.3% 49.3% −2.1% Missing 41.6% 41.9% −0.7% 41.6% 42.7% −2.2% 42.8% 41.4% 2.9% Age years 77.8±7.0 76.9±6.6 13.9 77.8±7.0 78.1±6.9 −4.2 77.5±7.1 77.2±6.7 0.4 Body mass index kg·m−2 20.5±3.9 21.3±4.0 −19.9 20.5±3.9 20.3±3.7 3.4 20.8±4.1 21.0±4.0 −4.1 Frequency of hospitalisation before hospitalisation for COPD exacerbation 0.84±1.3 0.59±1.2 18.5 0.84±1.3 0.98±2.1 −8.1 0.83±1.2 0.77±1.6 4.4 Observation period before hospitalisation for COPD exacerbation days 1055.4±574.0 847.0±571.3 35.9 1058.2±576.7 1055.4±610.1 0.5 912.7±567.4 913.9±587.4 −0.2 Data are presented as mean±sd unless otherwise stated. smd: standardised mean difference; ADL: activities of daily living.
- TABLE 2
Comorbidities during hospitalisation and treatments for COPD with and without inhaled corticosteroid (ICS) withdrawal, before and after 1–2 propensity score (PS) matching and after stabilised inverse probability weighting (IPTW)
All patients 1–2 PS matching Stabilised IPTW ICS withdrawal (n=971) ×100 Control (n=2764) ×100 smd ICS withdrawal (n=904) ×100 Control (n=1808) ×100 smd ICS withdrawal (n=872) ×100 Control (n=2591) ×100 smd Comorbidity Lung cancer 0.14% 0.08% 16.8% 0.14% 0.14% −0.2% 0.12% 0.11% 3.9% Other malignancy 0.10% 0.07% 12.5% 0.10% 0.11% −2.2% 0.08% 0.08% −1.1% Diabetes/abnormal glucose tolerance 0.21% 0.22% −2.4% 0.21% 0.22% −3.5% 0.27% 0.22% 11.5% Bone fracture/osteoporosis 0.06% 0.07% −2.1% 0.06% 0.07% −4.0% 0.05% 0.07% −4.7% Interstitial pneumonia 0.11% 0.05% 24.5% 0.11% 0.11% −0.9% 0.07% 0.07% 2.6% Bronchial asthma 0.37% 0.66% −61.0% 0.37% 0.39% −4.6% 0.58% 0.58% −0.2% Bronchiectasis 0.24% 0.22% 4.2% 0.24% 0.21% 7.2% 0.22% 0.22% −0.6% Pneumothorax 0.04% 0.03% 3.1% 0.04% 0.04% −2.6% 0.04% 0.03% 1.6% Pulmonary thromboembolism 0.00% 0.01% 3.8% 0.00% 0.00% 4.7% 0.01% 0.01% −0.2% Mycobacterium infection 0.02% 0.01% 10.9% 0.02% 0.02% 2.6% 0.01% 0.01% −0.5% Mycotic infection 0.02% 0.02% 0.6% 0.02% 0.03% −6.5% 0.02% 0.02% −1.7% Cor pulmonale 0.02% 0.02% 2.2% 0.02% 0.02% −0.8% 0.02% 0.02% 0.7% Congestive heart failure 0.21% 0.22% −0.8% 0.21% 0.20% 2.9% 0.22% 0.22% 0.2% Ischaemic heart disease 0.14% 0.14% 1.8% 0.14% 0.14% −0.3% 0.17% 0.14% 9.6% Tachycardia 0.11% 0.10% 3.8% 0.11% 0.11% 1.1% 0.11% 0.10% 0.5% Autoimmune disease 0.04% 0.03% 7.5% 0.04% 0.05% 5.0% 0.03% 0.03% 1.2% Stroke 0.03% 0.02% 5.0% 0.03% 0.03% −0.3% 0.02% 0.03% −1.5% Liver dysfunction 0.03% 0.02% 5.3% 0.03% 0.05% −9.2% 0.03% 0.03% 0.7% Renal failure 0.04% 0.03% 5.2% 0.04% 0.05% −2.4% 0.03% 0.03% −1.6% GORD 0.19% 0.22% −6.9% 0.19% 0.22% −5.9% 0.23% 0.23% 0.4% Constipation or ileus 0.17% 0.15% 4.6% 0.17% 0.16% 1.9% 0.20% 0.16% 11.2% Prostate hypertrophy 0.11% 0.10% 3.7% 0.11% 0.10% 4.5% 0.10% 0.10% −1.1% Treatment, categorical data Before hospitalisation Home ventilatory support 0.02% 0.02% −0.3% 0.02% 0.02% 0.8% 0.03% 0.02% 5.9% Home oxygen therapy 0.25% 0.29% −9.3% 0.25% 0.24% 0.8% 0.29% 0.28% 2.5% Both LAMAs and LABAs 0.24% 0.20% 8.3% 0.24% 0.24% −1.3% 0.24% 0.22% 4.8% LAMAs only 0.58% 0.67% −17.4% 0.58% 0.59% −0.6% 0.64% 0.65% −1.6% LABAs only 0.46% 0.36% 20.7% 0.46% 0.47% −2.3% 0.42% 0.40% 5.4% SABAs or SAMAs 0.43% 0.56% −27.2% 0.43% 0.44% −2.0% 0.54% 0.51% 5.5% Theophylline 0.32% 0.47% −31.2% 0.32% 0.33% −0.5% 0.45% 0.43% 4.6% Expectorants 0.75% 0.76% −1.9% 0.75% 0.74% 1.5% 0.71% 0.75% −9.2% Antibiotic prescriptions per 30 days 0.23% 0.31% −11.9% 0.23% 0.20% 5.0% 0.26% 0.28% −2.8% Macrolides per 30 days 0.11% 0.19% −19.4% 0.11% 0.09% 8.6% 0.14% 0.16% −5.2% TMP/SMX combination per 30 days 0.03% 0.02% 4.5% 0.03% 0.02% 4.2% 0.02% 0.02% −2.0% Anti-MRSA drugs per 30 days 0.00% 0.00% 5.5% 0.00% 0.00% 2.4% 0.00% 0.00% 1.5% Antifungal agent per 30 days 0.00% 0.00% −0.9% 0.00% 0.00% −2.8% 0.00% 0.00% −0.6% Medication for influenza per 30 days 0.00% 0.00% −3.6% 0.00% 0.00% −2.5% 0.00% 0.00% −0.0% Oral corticosteroids per 30 days 0.10% 0.18% −15.8% 0.10% 0.09% 3.1% 0.15% 0.16% −1.6% i.v. corticosteroids per 30 days 0.06% 0.13% −14.3% 0.06% 0.07% −3.7% 0.10% 0.11% −2.3% At and during hospitalisation Ambulance transport 0.22% 0.23% −1.7% 0.22% 0.21% 4.4% 0.21% 0.23% −4.2% ICU admission 0.01% 0.02% −6.1% 0.01% 0.02% −4.6% 0.02% 0.03% −1.4% Corticosteroids 0.37% 0.58% −41.8% 0.37% 0.38% −1.8% 0.50% 0.52% −3.8% Aminoglycosides 0.01% 0.01% −2.6% 0.01% 0.01% −3.4% 0.01% 0.01% −2.4% Carbapenems 0.13% 0.13% 0.9% 0.13% 0.14% −2.6% 0.14% 0.13% 2.3% Anti-MRSA drugs 0.02% 0.01% 6.8% 0.02% 0.03% −2.1% 0.03% 0.02% 8.2% Macrolides 0.24% 0.33% −22.1% 0.24% 0.23% 2.4% 0.29% 0.30% −2.2% Fluoroquinolones 0.29% 0.31% −3.3% 0.29% 0.28% 2.3% 0.30% 0.30% −0.8% Mechanical ventilation 0.06% 0.06% −0.6% 0.06% 0.07% −4.3% 0.08% 0.07% 5.9% Haemodialysis 0.01% 0.01% 4.6% 0.01% 0.01% 3.0% 0.01% 0.01% −1.2% Nasal tube feeding 0.02% 0.01% 7.2% 0.02% 0.01% 1.3% 0.02% 0.01% 7.2% Surgery under general anaesthesia 0.00% 0.00% −1.6% 0.00% 0.00% 6.3% 0.00% 0.00% −2.8% Prescription of LABAs/LAMAs 0.05% 0.01% 25.7% 0.05% 0.05% 0.0% 0.02% 0.02% −0.9% Prescription of LAMAs 0.24% 0.60% −77.3% 0.24% 0.25% −1.0% 0.25% 0.22% 7.7% Prescription of LABAs 0.26% 0.19% 16.9% 0.26% 0.27% −2.6% 0.49% 0.50% −1.1% Discharge to home 0.92% 0.97% −22.8% 0.92% 0.91% 4.0% 0.95% 0.95% 0.8% Treatment, numerical data Mean±sd Mean±sd Mean±sd Mean±sd Mean±sd Mean±sd Length of stay days 19.3±20.0 19.3±15.9 1.7 19.4±20.3 19.9±14.2 −2.9 20.0±21.4 19.4±15.3 3.7 smd: standardised mean difference; GORD: gastro-oesophageal reflux disease; LAMA: long-acting muscarinic antagonist; LABA: long-acting β2-agonist; SABA: short-acting β2-agonist; SAMA: short-acting muscarinic antagonist; TMP/SMX: trimethoprim/sulfamethoxazole; MSRA: methicillin-resistant Staphylococcus aureus; ICU: intensive care unit.
- TABLE 3
Hazard ratios (HRs) and 95% confidence intervals of re-hospitalisation for COPD exacerbation or death after 1–2 propensity score (PS) matching and stabilised inverse probability weighting (IPTW) in the inhaled corticosteroid (ICS) withdrawal group versus the control group
Re-hospitalisation or death Study population ICS withdrawal Control HR (95% CI) p-value 1–2 PS matching All 904 1808 0.65 (0.52–0.80) <0.001 Comorbid asthma 330 684 0.67 (0.50–0.91) 0.010 Without asthma 574 1124 0.68 (0.51–0.90) 0.008 Stabilised IPTW All 835 2621 0.71 (0.56–0.90) 0.005 Comorbid asthma 481 1513 0.82 (0.57–1.18) 0.294 Without asthma 353 1108 0.58 (0.45–0.75) <0.001 - TABLE 4
Incident rate ratios (IRRs) and 95% confidence intervals of post-discharge frequency of outpatient antimicrobial and corticosteroid prescriptions after 1–2 propensity score (PS) matching and stabilised inverse probability weighting (IPTW) in the inhaled corticosteroid (ICS) withdrawal group versus the control group
Observation period Prescription IRR (95% CI) p-value 1–2 PS matching 30 days Antimicrobials 0.94 (0.73–1.23) 0.668 Corticosteroids 0.97 (0.72–1.31) 0.856 1 year Antimicrobials 0.78 (0.63–0.98) 0.029 Corticosteroids 0.78 (0.60–1.02) 0.067 Stabilised IPTW 30 days Antimicrobials 0.90 (0.63–1.31) 0.598 Corticosteroids 1.06 (0.76–1.47) 0.733 1 year Antimicrobials 0.65 (0.51–0.83) 0.001 Corticosteroids 0.76 (0.56–1.02) 0.065
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary tables 00246-2019.supptables
FIGURE S1 Cumulative hazard curves for hospitalization for re-exacerbation or death after hospitalization for exacerbation in patients with chronic obstructive pulmonary disease (COPD) aged ≥65 years with or without ICS withdrawal. Results for (A) 1-to-2 propensity score-matched population; and (B) stabilized inverse probability of treatment weighted population. ICS, inhaled corticosteroids 00246-2019.figureS1
FIGURE S2 Cumulative hazard curves for hospitalization for re-exacerbation or death after hospitalization for exacerbation in patients with chronic obstructive pulmonary disease (COPD) aged ≥40 years with or without ICS withdrawal. Results for the 1-to-2 propensity score-matched population are shown. (A) All patients. (B) Patients aged ≥70 years. (C) Patients aged <70 years. ICS: inhaled corticosteroids 00246-2019.figureS2
FIGURE S3 Cumulative hazard curves for hospitalization for re-exacerbation or death after hospitalization for exacerbation in patients with chronic obstructive pulmonary disease (COPD) aged ≥40 years with or without ICS withdrawal. Results for the stabilized inverse probability of treatment weighted population are shown. (A) All patients. (B) Patients aged ≥70 years. (C) Patients aged <70 years. ICS: inhaled corticosteroids 00246-2019.figureS3
{kind=link}










