





Abstract
Adherence to inhaled corticosteroids (ICS) has been suggested to be poor but long-term follow-ups are lacking. The objective of the present study was to assess adherence to ICS treatment in patients with adult-onset asthma during 12-year follow-up.
A total of 181 patients with clinically confirmed, new-onset adult asthma were followed for 12 years as part of the Seinäjoki Adult Asthma Study. Adherence to ICS was assessed individually as the percentage of true dispensed ICS in micrograms per true prescribed daily ICS in micrograms over 12 years.
Mean 12-year adherence to ICS was 69% (mean±sd dispensed 2.5±1.8 g and prescribed 3.6±1.5 g budesonide equivalent per patient for 12 years), annual adherence varying between 81% (year 1) and 67% (year 12). Patients with good 12-year adherence (≥80%) used oral corticosteroids more often, and had add-on drugs in use and asthma-related visits to healthcare more often. In addition, they showed less reversibility in forced expiratory volume in 1 s and had higher peripheral blood neutrophil counts. However, lung function decline was steeper in patients with poorer adherence (<80%) and this association remained in multiple linear regression analysis. No difference was found in symptom scores, blood eosinophil counts, exhaled nitric oxide or immunoglobulin E between the patients with different levels of adherence.
In patients with adult-onset asthma, adherence to ICS was moderate. Poorer adherence (<80%) to ICS was associated with more rapid decline in lung function but was not associated to symptoms or markers of inflammatory endotypes.
Abstract
Mean long-term adherence to ICS treatment is 69% in patients with confirmed adult-onset asthma. While good ICS adherence (≥80%) is associated with features of more severe asthma, poorer adherence (<80%) predicts more rapid lung function decline. http://bit.ly/37mvh74
Introduction
Inhaled corticosteroids (ICS) are the basis of asthma treatment, reducing airway inflammation, improving lung function, controlling symptoms and reducing exacerbations [1, 2]. When evaluating whether the patients take their medication as prescribed, one of the most settled terms is “medication adherence”, consisting of three essential elements: initiation, implementation and persistence [3]. Objective methods, such as electronic monitoring and electronic health records, or subjective methods, like patient reports, can be used to address medication adherence. Whichever the method used, adherence to ICS treatment has been suggested to be poor [4].
The age of asthma onset has been shown to be a significant factor in distinguishing the phenotypes of asthma [5, 6]. Although a substantial proportion of asthma originates in childhood, recent data from the USA and Finland show that asthma diagnosed at adult age is common, and is in fact the dominant phenotype among women aged 35–40 years [7–9]. Patients with late-onset asthma are usually nonatopic and their response to corticosteroids is poorer than in patients with early-onset disease, and therefore they require more tailored medication [5, 6]. Moreover, asthma rarely remits in patients with adult-onset asthma [5, 6, 10, 11]. Even though many different characteristics of the adult-onset asthma phenotype have been described, adherence to medication remains unstudied.
Possible consequences of poor ICS adherence are decline in lung function, poorer symptom control and quality of life, and increase in asthma-related hospitalisations and costs [12–17]. Low adherence rates have also been associated with increased mortality and morbidity [4, 15, 18]. However, previous studies have usually been cross-sectional or short-term follow-ups and very little is known about the variation of medication adherence between and within persons in long-term treatment. In addition, to enhance reliable comparison of the results of adherence studies, variability in associated calculations and terms needs attention. Many studies based on medical records have used the best information available but the shortages in prescription or dispensation data have led to assumptions in adherence calculations [19–22]. In addition, previous studies have had shortages of information concerning diagnostic criteria, age of asthma onset and duration of asthma, which may all be factors influencing the results [22–25]. Though adherence to ICS has been <50% in recent studies, we hypothesised that when patients have a confirmed diagnosis of asthma and regular ICS in use, they would have better medication adherence than previously described. Therefore, our aim was to assess adherence and its variability in long-term ICS treatment in real-life new-onset adult asthma patients with confirmed diagnoses during 12-year follow-up by using full coverage dispensing data and true prescribed medication.
Methods
Study design and patients
This study is part of Seinäjoki Adult Asthma Study (SAAS), which is a prospective 12-year follow-up study of 257 patients with diagnoses of new-onset adult asthma. Patients were consecutively included in the study during the period 1999–2002 if all of the following criteria were fulfilled: 1) new-onset asthma diagnosed by a respiratory specialist; 2) confirmation of diagnosis by lung function measurements showing variable or reversible obstruction; 3) symptoms of asthma; and 4) age ≥15 years (tables S1 and S2). Importantly, patients with comorbidities or smoking history were not excluded. Study participants gave written informed consent to the study protocol approved by the ethics committee of Tampere University Hospital, Tampere, Finland. More than 94% of the patients diagnosed with novel asthma at the study site were recruited to the study [11]. In 2001, the study population represented >38% of all novel diagnoses of asthma made in adults in the whole geographical area [26].
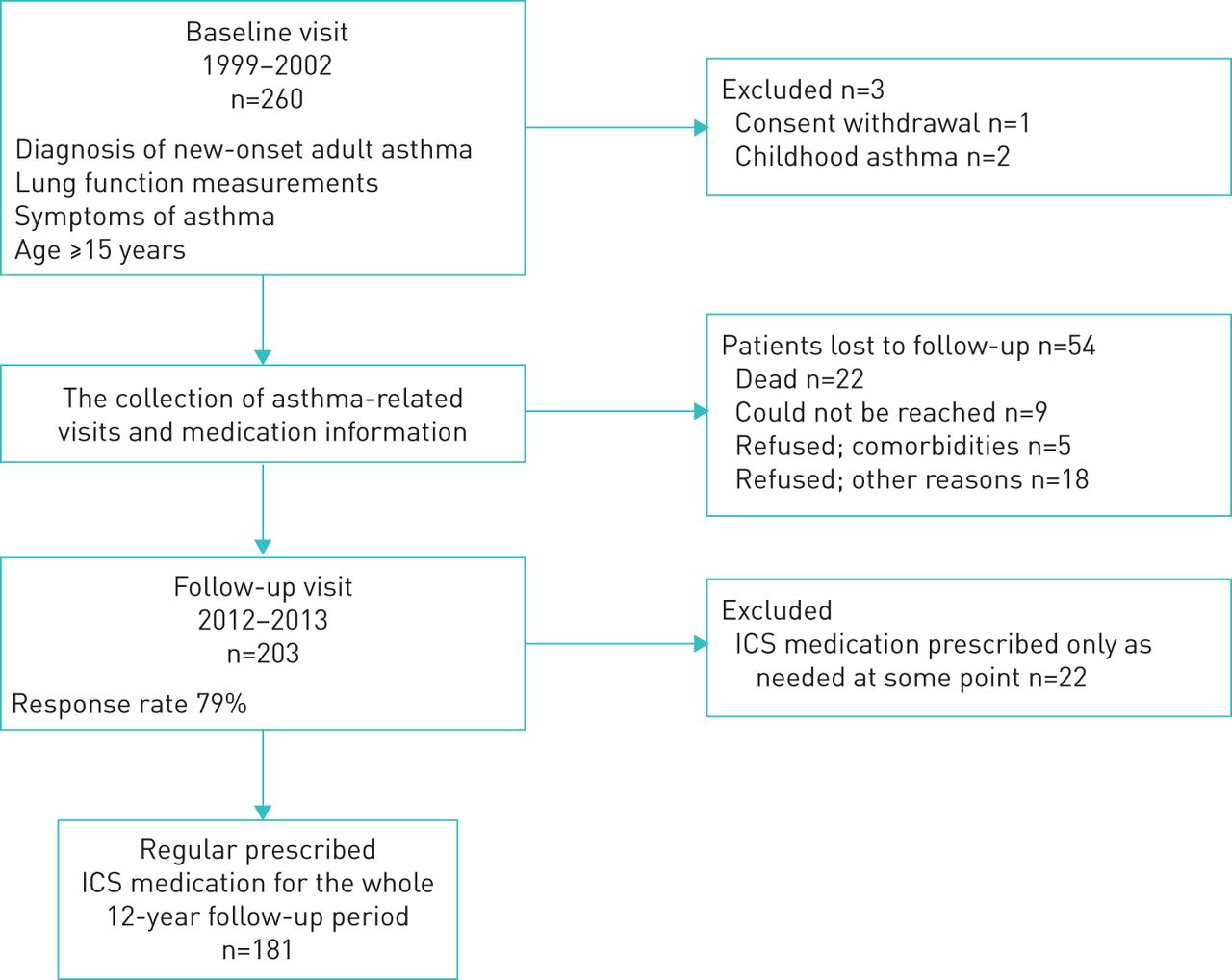
The study protocol has been published previously [27]. A schematic presentation of the study is shown in figure 1. The study was divided in two parts: collection of the original cohort (baseline) and the 12-year follow-up visit. At the baseline visit, data were collected on symptoms, lung function, demographics and initial medication [26]. Patients were followed for 12 years (mean 12.2 years, range 10.8–13.9 years) after the diagnostic visit. From the original cohort of 257 patients, 203 (79%) returned to the 12-year follow-up visit in which asthma status, medication, control and lung function were evaluated (supplementary material). All asthma-related visits and medication information were collected from the whole 12-year follow-up period from medical records. At the baseline visit, regular ICS medication was prescribed, and each patient received asthma education and self-management instructions according to Finnish Asthma Programme [28]. To ensure that the study population included only patients with regular ICS medication, we excluded patients for whom ICS was prescribed only as needed at any point in the follow-up period (figure 1).
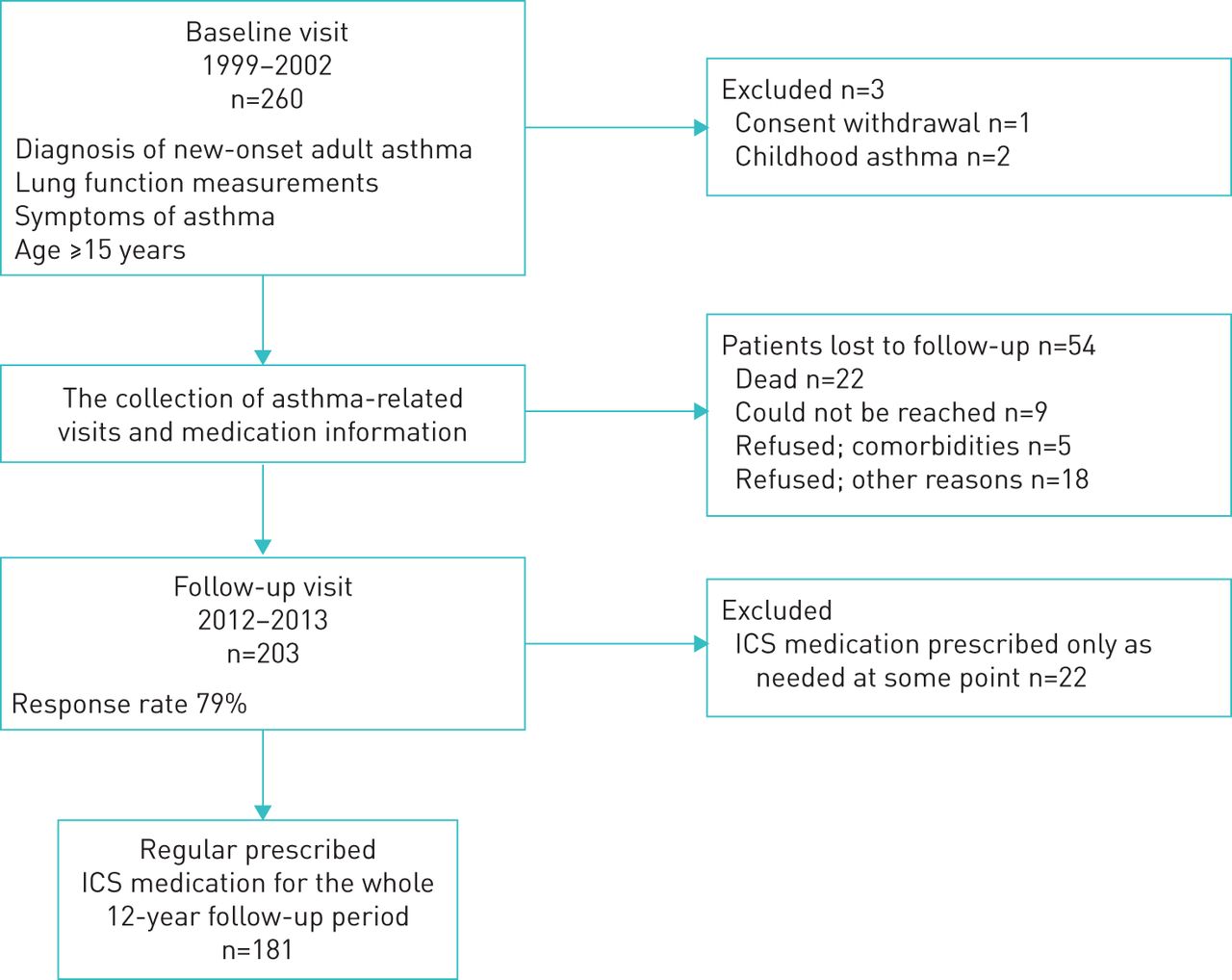
Flowchart of the study. ICS: inhaled corticosteroids.
Computation of adherence
The prescribed dose in each patient for the whole 12-year period was calculated based on medication records as previously described [29]. Shortly, we converted all prescribed ICS doses (ICS in both separate and combination inhalers) to budesonide equivalents and based on that information, calculated annual prescribed ICS medication for each patient. The dispensed ICS and oral corticosteroids were obtained from the Finnish Social Insurance Institution, which records all purchased medication from all Finnish pharmacies (supplementary material). Adherence to ICS was determined as previously described [3], consisting of initiation, implementation and persistence (supplementary material). The 12-year adherence was calculated by using formula 1 and annual adherence was calculated for each patient by using formula 2 (supplementary material). For comparing adherence groups, we used the most common cut-point of 80% [4, 21, 22]. (1)
(1) (2)
(2)
Statistical analyses
The data are presented as mean±sd or median (interquartile range) except in figures, where annual cumulative and daily doses are represented as mean±sem for clarity. Comparison of groups with ≥80% or <80% adherence was analysed by using independent-sample t-tests and Mann–Whitney U-tests for normally and non-normally distributed continuous variables, respectively, and Pearson Chi-squared or Fisher's exact test for categorical variables. To analyse differences between prescribed and dispensed ICS doses in both cumulative and annual manners, the individual patient's area under curve (AUC) was defined and mean AUC values were compared by using paired-samples t-tests. A multivariable logistic regression was performed to predict oral corticosteroid use and multiple linear regression analysis was performed to analyse factors associated with forced expiratory volume in 1 s (FEV1) decline as previously described [30]. The correlation matrix was analysed and explanatory variables not strongly correlated (r<0.7) were included in the analysis. In the linear regression analysis, outliers were removed to ensure homoscedasticity (supplementary material). A p-value <0.05 was regarded as statistically significant. Statistical analyses were performed by using IBM SPSS statistics software, version 24 (IBM SPSS, Armonk, NY, USA) and GraphPad Prism software, version 7.03 (GraphPad, La Jolla, CA, USA).
Results
Patient characteristics
The main characteristics of study patients are shown in table S3. The majority of the patients were female (60%) and half of the patients were current or ex-smokers. At the follow-up visit, patients had higher body mass index (BMI), FEV1 and forced vital capacity (FVC), but lower blood eosinophil counts and symptom scores (Airway Questionnaire 20) than at the baseline.
Long-term adherence for 12 years
The mean 12-year adherence to ICS was 69% across all 181 patients (dispensed ICS 2.5±1.8 g and prescribed ICS 3.6±1.5 g budesonide equivalent per patient for 12 years) (figure 2). To visualise the variation in the long-term adherence in the whole study population, we determined annual adherence for each patient individually. The mean annual adherence gradually declined from year 1 (81%) to year 12 (67%) (figure 3). The prescribed annual daily ICS doses for study patients were high (on average, >800 µg) but patients dispensed significantly lower doses (on average, <800 µg budesonide equivalent) of ICS during the 12-year follow-up (figure 4). If calculated by using the maximum value of the dose range in the prescription instead of the mean value of the range (e.g. in a subject who was prescribed budesonide/formoterol 200/6 µg, one to two puffs twice a day), it affected the mean 12-year adherence by −4.4%. Smoking status or comorbidities did not affect the mean 12-year adherence values (data not shown).

Annual prescribed and dispensed inhaled corticosteroids (ICS) shown as cumulative values (mean±sem) (n=181). p-value represents difference between cumulative prescribed and dispensed ICS as defined by the area under the curve method and paired-sample t-test.

The average annual adherence (mean±sem) during the 12-year follow-up period (n=181).
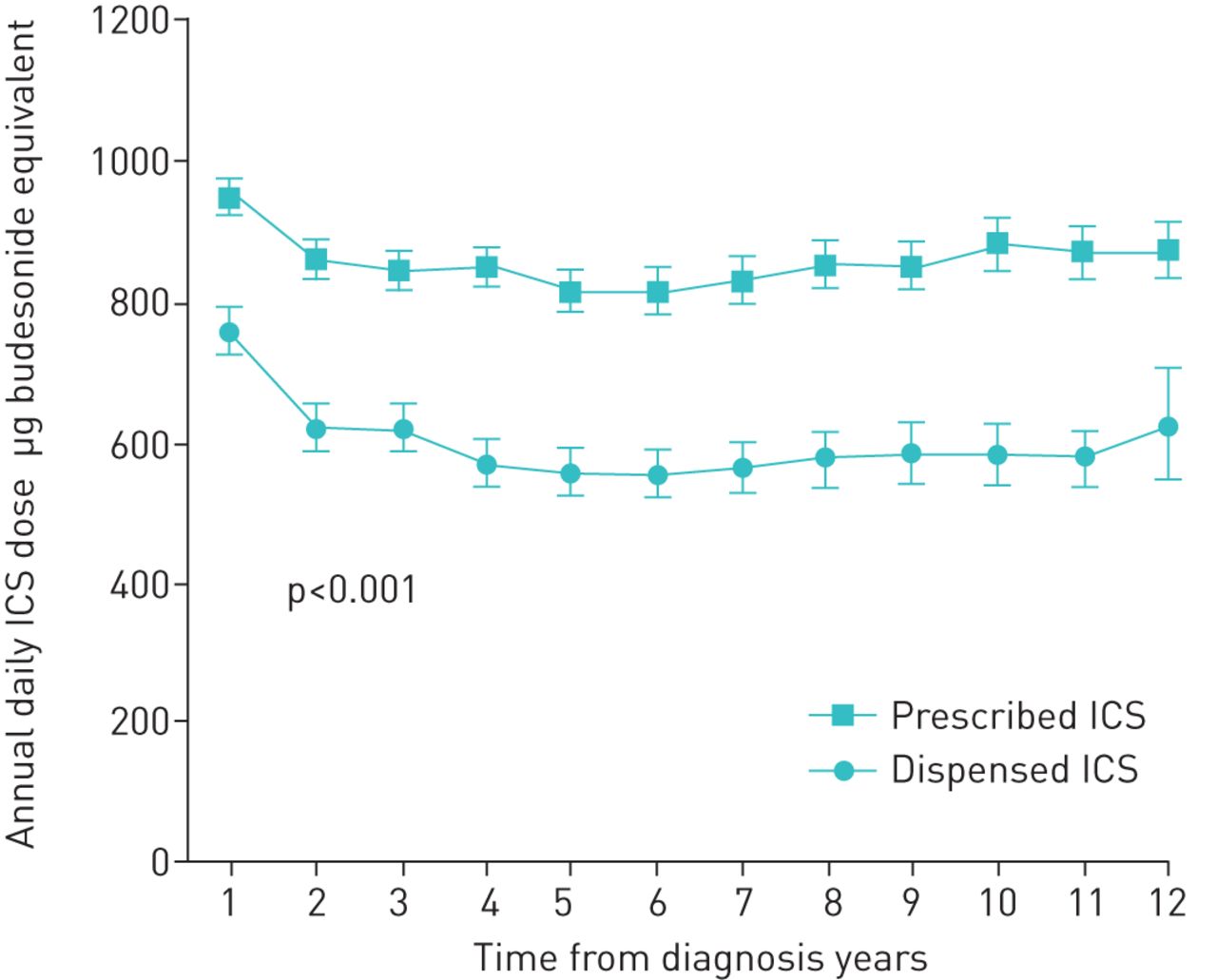
Average annual prescribed and dispensed daily doses of inhaled corticosteroids (ICS) in the 12-year follow-up periods (mean±sem) (n=181). p-value represents difference between cumulative prescribed and dispensed ICS as defined by area under the curve method and paired-samples t-test.
Changes in adherence over 12 years
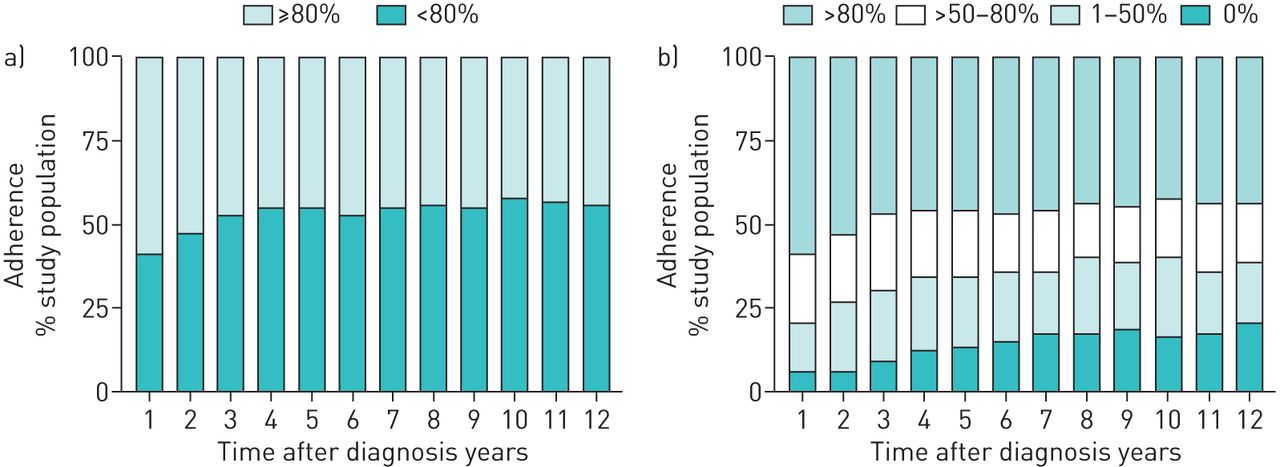
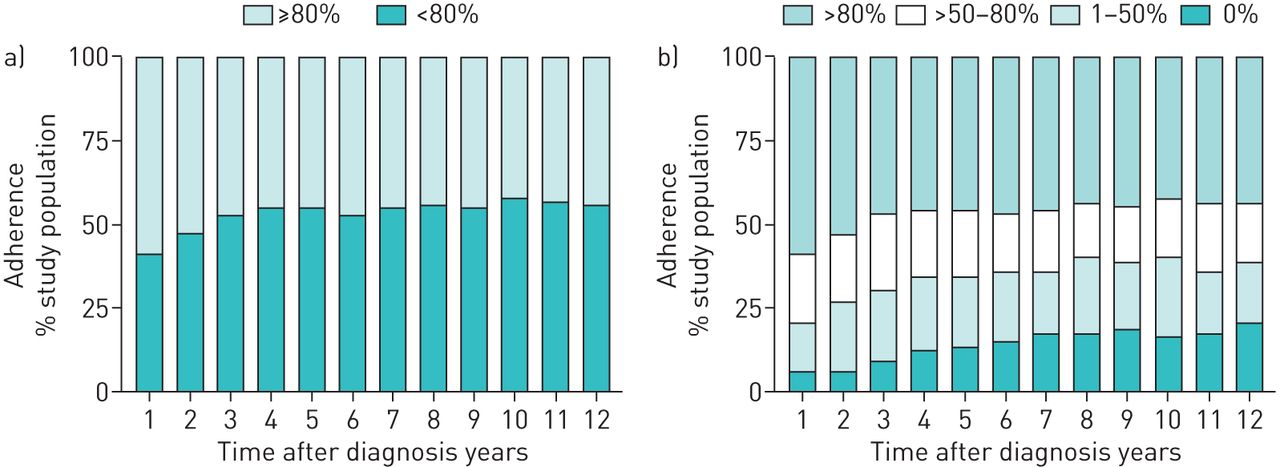
The proportion of adherent patients (≥80%) was highest during the first year after the diagnosis (figure 5). Of the study patients, 17 (9%) had annual ICS adherence rates >80% during the whole 12-year follow-up period. In addition, 55 (30%) of the patients had annual adherence that was always >50%. Annual nonadherence (annual adherence rate 0%) ranged from 6.6% to 20.4% but on average, 14.5±4.6% of the patients were nonadherent during the 12 years (figure 5b). The total number of patients having an annual nonadherent period at least once was 67 (37%), and 1% of the patients failed to collect their first treatment prescription (initiation) [3] and were fully nonadherent to ICS therapy during the whole 12-year follow-up period.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Annual adherence rates a) when using 80% adherence as a cut-off (n=181); and b) when dividing patients into high, moderate or low adherence, and non-adherence during the 12-year follow-up.
Comparison of patients with good or poor 12-year adherence
Average prescribed ICS doses were similar in patients with better (≥80%) and poorer (<80%) 12-year adherence but dispensed ICS doses were only one-third in patients with poorer adherence (table 1). Patients with good 12-year adherence (≥80%) more often had a long-acting β2-agonist (LABA) or any other add-on drug in use, more often reported oral corticosteroid courses and were dispensed higher amounts of oral corticosteroids during the follow-up (table 2 and supplementary material). In addition, they showed less FEV1 reversibility, had higher peripheral blood neutrophils (table 3), had a higher number of asthma-related contacts to healthcare and tended to have more unplanned hospital in-patient days due to asthma (table 2). However, the decline in lung function was steeper in patients with poorer adherence (<80%). There was no difference in symptom scores or other inflammatory markers (blood eosinophils, exhaled nitric oxide fraction (FENO) or IgE) between the subgroups with different 12-year adherences (tables 2 and 3). If a lower cut-point for adherence was used, the results were largely similar. However, patients with ≥50% adherence were more obstructive (lower FEV1/FVC) but did not differ by lung function decline (table S4). Furthermore, we evaluated whether those with one or more completely nonadherent years differed from those without nonadherent years and the results were similar to the main results of the study (table S5).
Characteristics of patients at the 12-year follow-up visit and their medication according to their 12-year adherence
Symptoms and burden due to asthma in patients according to their 12-year adherence
Lung function and markers of inflammation in patients according to their 12-year adherence
Patients with ≥80% adherence reported using oral corticosteroids more often during the follow-up and after adjusting this finding for age >50 years, sex, BMI >30 kg·m−2, pre-FEV1 at follow-up visit and COPD, the association remained (OR 1.99, 95% CI 1.02–3.87; p=0.043). In addition, we carried out multiple linear regression analysis to find out whether poor adherence predicts accelerated lung function decline when adjusted for age, ΔBMI during the follow-up period, sex, FENO >20 ppb, smoking history ≥10 pack-years, blood eosinophils, use of oral corticosteroid courses, FEV1 % pred at baseline and ΔFEV1 (baseline−maximum0–2.5) (table S6). After adjustments, poorer adherence (<80%) remained a significant predictor for FEV1 (in millilitres) decline.
Discussion
In this study, we evaluated both annual and 12-year adherence to ICS from diagnosis to a 12-year follow-up visit in patients with adult-onset asthma. Mean 12-year adherence to ICS was 69%. Patients with good 12-year adherence (≥80%) more often used LABA daily, and had more oral corticosteroid courses and asthma-related contacts to healthcare. In addition, they showed less reversibility of FEV1 and had higher peripheral blood neutrophil counts. However, lung function decline during the follow-up period was steeper in patients with poorer long-term adherence (<80%). These results suggest that in patients with confirmed diagnoses of adult-onset asthma, the mean adherence to ICS is moderate but variance in annual ICS adherence is also common in long-term treatment. Even though good ICS adherence (≥80%) was, overall, associated with features of more severe asthma, poorer adherence (<80%) predicted more rapid lung function decline.
Our study showed that the mean 12-year ICS adherence was 69%, which is in line with the previous studies where overall adherence to asthma treatment ranged 30–70% [4]. However, adherence was higher in our study than in other adherence studies based on electronic medical records, where adherence ranged 21–52% [23–25, 31–33]. Previous short-term studies have suggested a decline in lung function or reductions in symptom control and quality of life because of poor adherence [12, 13, 15, 16, 31]. In our study, for the first time, poorer adherence (<80%) was found to predict more rapid lung function decline long term. It might be argued whether the annual difference of 6 mL in median values is clinically significant but most patients had chronic asthma, which rarely remits, and therefore, the cumulative effect in the long term may have clinical significance. Even though patients with poorer adherence otherwise showed features of less severe disease (e.g. less use of add-on drugs and fewer healthcare visits), indicating that these patients may be less adherent because of the feeling of not needing medication, poor adherence seems to have harmful long-term effects on lung function. Given that reduced lung function is a risk factor for exacerbations [34], these patients might predispose themselves to exacerbations in the long term by not taking their medication. In our study as well as in the previous ones [30, 35], increased eosinophilic inflammation has been shown to associate with more rapid decline in lung function, but in our study, no difference was found in the level of blood eosinophils or FENO between the subgroups with different levels of adherence. However, the blood eosinophil and FENO values were based on a single time-point (12-year follow-up visit), leaving the possibility that the level of inflammation may have been higher for some period during the follow-up in these patients, providing a possible mechanism for steeper lung function decline in less adherent patients.
Despite the mean 12-year ICS adherence being as high as 69%, annual nonadherence was observed in 37% of the patients at least once during the 12-year follow-up period and only 9% of the patients had annual adherence that was always >80%. In summary, individual patients appeared to use ICS periodically under and over the prescribed doses but on average, patients adhered to ICS treatment well during long-term treatment. As symptoms of asthma and airway limitation vary over time [2], patients' adherence behaviour may reflect the nature of asthma as a disease. The reasons behind relatively high rates of adherence in Finnish adult asthma patients are various: 65% reimbursement of asthma medicine expenses, relatively low medicine prices, prescriptions for 1–2 years at time (medication available when needed), cost-free renewal of prescriptions, public health services available for all, lung function measurements at asthma contacts and guidance on correct inhaler use by, for example, specialised asthma nurses and the Finnish asthma programme [28].
Previous studies on adherence to asthma medication have been short-term follow-ups, the most common follow-up time being 12 months [23, 25, 31–33]. SAAS is a 12-year, real-life follow-up study of new-onset adult asthma patients giving information on adherence to ICS over an exceptionally long period. In addition, many studies only included populations from healthcare organisations or insurance databases, meaning that the patient cohort is selected and patients outside these databases are excluded [24, 31, 32]. SAAS has collected extensive 12-year follow-up data including information on all prescribed and dispensed asthma medication of the study patients. Moreover, all new-onset adult asthmatics, i.e. patients with comorbidities and a history of smoking, were included and therefore, the study cohort represents the general adult population with asthma well [26].
Information on the duration of asthma, age of asthma onset and diagnostic criteria used were missing from the previous adherence studies, all of which are factors that could influence adherence [23, 24, 31–33, 36]. In the studies using administrative or other register data only, asthma diagnosis has typically been based on International Classification of Diseases codes found from these records [25, 36, 37], causing unreliability and variation in the correctness of asthma diagnosis. For example, a study in the USA [23] identified that only 8.8% of the patients continued to refill their prescriptions from the index date to year's end, whereas in another study [38], ∼50% of the patients did not renew their initial prescription. In these studies, the average adherence to ICS was poor, which may be partly explained by the absence of strict diagnostic criteria and confirmed asthma diagnosis, leading to inclusion of nonasthmatic subjects in the study. Conversely, many studies based on health records have used the best information available but shortages in prescription or dispensation data have led to assumptions in adherence calculations [19–22]. For example, the total day's supply is often based on pharmacists' estimation, typically assuming the maximum use of prescribed doses (e.g. one to two puffs once or twice a day assumed to be four puffs a day), which can lead to underestimation of adherence [20]. Moreover, Blais et al. [39] noted that when one of the most commonly used measures adherence (proportion of days covered [37]) from administrative data is used, it assumes that the medication is prescribed for chronic daily use, and in cases of suboptimal prescribing, it may lead to underestimation of adherence. In our study, the diagnosis of asthma was made by a respiratory physician, and was based on both typical symptoms and variable or reversible airway obstruction in lung function measurements. Regarding adherence calculations, we examined all prescribed and refilled ICS doses and dose changes for 12 years based on individual patients' medical records and dispensation data, and all patients had regular prescribed ICS medication for the whole follow-up period (supplementary material).
Because our study was based on medical records and pharmacy dispensation data, it has some limitations. Firstly, the medical records were not always complete (shortage of physicians' notes, e.g. missing dose information) but prescribed medication was calculated based on previously confirmed information. Secondly, dispensing of a medicine does not guarantee patients' actual use of ICS nor good inhalation technique. Thirdly, some information on patients' behaviour regarding stepping medication up and down was not available in our study (i.e. patients may have used an action plan during influenza or an exacerbation and doubled the ICS dose). Despite these limitations, electronic medical records are preferred because they enable long observation periods in the assessment of adherence and they are commonly used in evaluation of adherence [4]. Moreover, electronic monitoring devices (EMDs), such as smart inhalers, are the gold standard in precise and reliable monitoring of adherence. Our results showed that adherence to ICS decreased most rapidly during the first 4 years of follow-up and this would potentially be an optimal point for EMD studies.
The results of earlier studies have shown many negative associations as a result of patients' poor ICS adherence [4, 12, 15]. In this study, patients with poorer long-term ICS adherence used remarkably lower ICS doses, less frequently used LABA on daily basis and were less often hospitalised compared to patients with better 12-year ICS adherence. This suggests that patients with poorer adherence (<80%) may have had milder asthma compared to patients with better adherence (≥80%). Therefore, undesirable treatment outcomes should not be regarded only as consequences of poor adherence, since even patients with good adherence may suffer from these outcomes. Patients with better adherence had also higher blood neutrophil counts and showed features of more severe asthma, indicating that some patients may have had non-T2-mediated disease. Future studies should pay more attention to the reasons why undesirable outcomes emerge in patients with good adherence to ICS and whether there would be more effective treatment strategies for these patients [40].
Taken together, we show, for the first time, long-term, 12-year adherence data of patients with adult-onset asthma based on true prescribed and dispensed medication. Clinical patients with objectively confirmed diagnoses of new-onset adult asthma had, on average, moderate adherence to long-term ICS treatment. This suggests that when evaluating patients' adherence, it is important to ensure that study population includes only patients with reliable asthma diagnoses and need for regular ICS medication [36]. In addition, when assessing long-term adherence to ICS, major variability in annual rates of adherence should be considered and, therefore, follow-up periods should be set long enough. In future, adult- and childhood-onset asthma patients should be compared to gain better understanding of the characteristics of adherence in different phenotypes. The new information about adherence characteristics in phenotypes would enhance possibilities to intervene with patients who show signs of inefficient treatment. All in all, our results show that poor adherence to ICS treatment may lead to steeper decline in lung function, which may have negative consequences in the long term. Our findings, therefore, also support performing spirometry regularly, as recommended by the Global Initiative for Asthma. Otherwise, patients with good adherence showed features of more severe asthma in comparison to less adherent patients. These patients need new strategies for their asthma treatment when regular controller medication seems not to be effective enough.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00324-2019.SUPPLEMENT
Acknowledgements
Aino Sepponen (Dept of Respiratory Medicine, Seinäjoki Central Hospital, Seinäjoki, Finland) is gratefully acknowledged for her help through all stages of this work.
Footnotes
This article has supplementary material available from openres.ersjournals.com
This study is registered at www.clinicaltrials.gov with identifier number NCT02733016.
Author contributions: H. Kankaanranta, L.E. Tuomisto, O. Niemelä and P. Ilmarinen conceived and designed the study; I Vähätalo, P. Ilmarinen and P. Nieminen analysed the data; H. Kankaanranta, L.E. Tuomisto, O. Niemelä, P. Ilmarinen and I Vähätalo collected the data; I Vähätalo, P. Ilmarinen and H. Kankaanranta wrote the manuscript; and all authors reviewed and edited the manuscript.
Conflict of interest: I. Vähätalo reports personal fees for a lecture from AstraZeneca outside the submitted work.
Conflict of interest: P. Ilmarinen reports a grant for analysis and write-up of a study and a fee for a lecture from AstraZeneca, and personal fees for lectures from Mundipharma, GlaxoSmithKline and Orion, outside the submitted work.
Conflict of interest: L.E. Tuomisto reports reimbursement of costs for attending international congresses from Chiesi, Boehringer Ingelheim, Orion Pharma and TEVA; reimbursement of costs for a lecture from AstraZeneca; and attendance of an advisory board meeting for Novartis, outside the submitted work.
Conflict of interest: M. Tommola reports personal fees for lectures from AstraZeneca, Pfizer and Chiesi; personal fees for lectures and consultation from Boehringer Ingelheim; and grants from the Orion Research Foundation, outside the submitted work.
Conflict of interest: O. Niemelä has nothing to disclose.
Conflict of interest: L Lehtimäki reports personal fees from ALK, AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Novartis, Mundipharma, OrionPharma, SanofiGenzyme and Teva, outside the submitted work.
Conflict of interest: P. Nieminen has nothing to disclose.
Conflict of interest: H. Kankaanranta reports fees for lectures and consulting, costs for attending an international congress, and a research grant to their institution from AstraZeneca; fees for consulting from Chiesi Pharma AB, SanofiGenzyme and GlaxoSmithKline; fees for lectures and consulting, and costs for attending international congresses from Boehringer Ingelheim and Orion Pharma; fees for lectures and consulting from Novartis; and fees for lectures from Mundipharma, outside the submitted work.
Support statement: This study is funded by the Tampere Tuberculosis Foundation (Tampere, Finland), the Finnish Anti-Tuberculosis Association Foundation (Helsinki, Finland), the Research Foundation of the Pulmonary Diseases (Helsinki, Finland), the Ida Montini Foundation (Kerava, Finland), the Pirkanmaa Regional Fund of the Finnish Cultural Foundation (Helsinki, Finland), Allergy Research Foundation (Helsinki, Finland), Competitive State Research Financing of the Expert Responsibility Area of Tampere University Hospital (Tampere, Finland) and the Medical Research Fund of Seinäjoki Central Hospital (Seinäjoki, Finland). None of the sponsors had any involvement in the planning, execution, drafting or write-up of this study. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received November 21, 2019.
- Accepted February 6, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










