





Abstract
Few studies have examined the contribution of life-course factors in explaining familial aggregation of chronic lung conditions. Using data from the 1958 British Birth Cohort, a life-course approach was used to examine whether, and how, exposure to risk factors through one's life explained the association between parental respiratory disease history and symptomatic airflow obstruction (AO). Cohort participants (n=6212) were characterised in terms of parental respiratory disease history and symptomatic AO at 45 years. Life-course factors (e.g. smoking, asthma and early-life factors) were operationalised as life period-specific and cumulative measures. Logistic regression and path analytic models predicting symptomatic AO adjusted for parental respiratory disease history were used to test different life-course models (critical period, accumulation- and chain-of-risks models). While some life-course factors (e.g. childhood passive smoking and occupational exposure) were individually associated with parental respiratory disease history and symptomatic AO, asthma (OR 6.44, 95% CI 5.01–8.27) and persistent smoking in adulthood (OR 5.42, 95% CI 4.19–7.01) had greater impact on the association between parental respiratory disease history and symptomatic AO. A critical period model provided a better model fit compared with an accumulation-of-risk model and explained 57% of the effect of parental respiratory disease history on symptomatic AO. Adulthood asthma and smoking status explained around half of the effect of parental respiratory disease history on chronic obstructive pulmonary disease. Beyond smoking history, the combination of parental respiratory disease history and adulthood asthma may provide an opportunity for early diagnosis and intervention.
Abstract
Adulthood asthma and smoking explain half of the effect of parental respiratory disease history on symptomatic airflow obstruction. Use of a life-course approach and models may help clarify mechanisms behind associations in intergenerational lung health. http://bit.ly/2PIzGf4
Background
Adult offspring of people with chronic obstructive pulmonary disease (COPD) have nearly 60% higher odds of developing COPD compared with people without a parental history [1]. This relationship may be explained by a complex interaction of COPD risk factors [2], which are present throughout a person's life course [3]. The parent–offspring COPD association may be explained by genetic factors (such as in α-1 antitrypsin deficiency [4]), intergenerational smoking behaviour [5] or similar environmental exposures during cohabitation [3] typically during the offspring's early life. Parental behaviour and socioeconomic status may influence their offspring's behaviour and occupational opportunities, which may alter the lung-function trajectory [6, 7]. Studies identifying associations between COPD and factors potentially related to parental history of COPD [8, 9] have commonly focused on individual risk factors without considering how these risk factors relate to parental history of respiratory disease and its relationship to offspring lung health.
Life-course epidemiology models may assist in understanding intergenerational associations of lung health [10]. For instance, the critical period model emphasises exposure to a stimulus during a specific time period (e.g. in utero exposure to smoking) [11]. The chain-of-risk model proposes that one factor (e.g. prematurity) may lead to another factor (e.g. childhood asthma), which is associated with later-life health outcomes (increased risk of COPD in later life) [8, 12]. A third model, the accumulation-of-risk model, hypothesises that exposure to different risk factors at different stages in life can have an additive effect [12] (e.g. longer periods of biomass exposure being associated with greater lung-function decline [13]).
To our knowledge no previous studies have comprehensively investigated the combined influences of parental and life-course factors on later-life lung health using a combination of spirometry results and respiratory symptoms as an outcome measure. This study aimed to use a life-course approach to investigate parental and life-course influences on the development of respiratory symptoms with airflow obstruction (AO) in adulthood using data from the National Child Development study (1958 birth cohort). The primary objectives were to examine 1) associations between parental respiratory disease history and known life-course factors for symptomatic AO in offspring; and 2) associations between offspring life-course factors associated with parental respiratory disease history and symptomatic AO at 45 years using critical period, accumulation-of-risk and chain-of-risk life-course models.
Methods
Study population
The National Child Development study (1958 cohort) began as a study on perinatal mortality that examined factors associated with stillbirth and infant mortality [14]. The initial assessment included 17 416 births occurring during a specific week of 1958 in England, Scotland and Wales [14]. Immigrants born outside the United Kingdom (UK) but born in the same week (n=920) were included until age 16 [14]. Up until 2013, nine sweeps of data collection were completed with data on education, health, social, and economic circumstances collected from the cohort throughout their childhood (at birth, 7, 11, 16 years) and adulthood (23, 33, 42 years) [14, 15]. Biomedical data were collected from 9377 cohort members when they were 45 years old [16]. Details on recruitment and participation rate at each sweep has been reported [16]. Approval from relevant ethics committees and consent from participants were obtained for each sweep of data collection [17].
Measures
Measures used in this study are briefly described below with further details provided in the supplemental material.
Outcome variable
Offspring symptomatic AO was operationalised as airway obstruction defined as ratio of forced expiratory volume in 1 s (FEV1) to forced vital capacity (FVC) <0.7 [2] at 45 years together with reported respiratory symptoms (cough, phlegm, shortness of breath or wheeze) at 42 years as per previous studies [2, 18].
Parental history
Data on parental respiratory disease history were collected from the cohort member's mother during the cohort's childhood. If the mother was not available, data were collected from the father (or mother-figure) during the cohort's childhood. Participants were considered to have a positive parental respiratory disease history if the participant's mother had a respiratory illness during pregnancy, or if either parent in the household had any respiratory medical history when the cohort member was 11 and 16 years after the first sweep.
Life-course factors
COPD risk factors during specific life periods were identified from the literature [2, 3, 19], including exposure to smoking (passive and personal smoking), social class, asthma, early-life factors (birthweight, preterm birth, pneumonia in childhood) and environmental exposure (biomass and occupation exposure). Table 1 summarises how these factors were operationalised for specific life periods (in utero/at birth, childhood, adulthood) or as cumulative measures using data available from seven sweeps of data collection. Data of some factors were available at multiple time points (e.g. passive smoke exposure at 23 years, 33 years and 42 years) were analysed as a single critical period measure (ever or never passive smoke exposure in adulthood) (see also supplemental material).
Summary of COPD risk factors operationalised with respect to life period
Statistical analysis
Associations between parental respiratory disease history and individual offspring life-course factors were first individually tested using Chi-squared or independent sample t-test as appropriate to reduce the pool of relevant life-course factors. Life-course factors that were found to be related to parental respiratory disease history (based on statistical significance level of α=0.1) were then used in logistic regression models to assess their relationships with offspring symptomatic AO. A more liberal α was used in this first step of analysis to include potentially relevant life-course factors in the second step of the analysis.
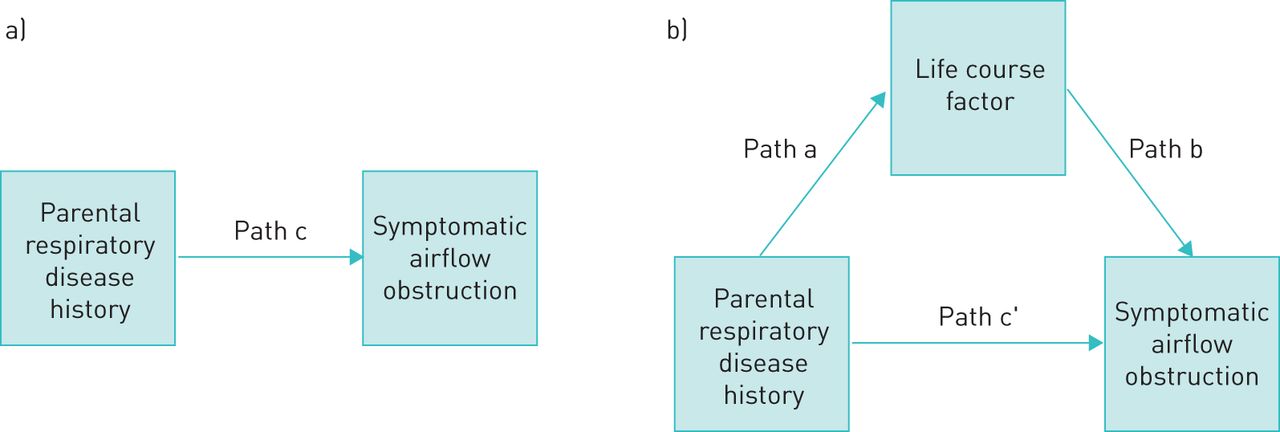
Life-course factors of a given type (smoking, social class, asthma, others) were first examined separately through path analysis [20]. This method allowed both direct and indirect (or mediated) effects between an exposure (parental respiratory disease history) and an outcome measure (symptomatic AO) to be assessed (figure 1). Using this model, the total effect (i.e. direct and indirect) of parental respiratory disease history on airway obstruction with respiratory symptoms in cohort members was tested (figure 1a, path c). The total indirect effects is a product of path a and b [21]. Individual life-course factors were separately added in the same model to establish whether they satisfied criteria for mediation as per Baron and Kenny [21]: 1) whether parental history was related to the life-course factor (figure 1b, path a); and 2) whether the individual life-course factors were related to symptomatic AO (figure 1b, path b) while accounting for parental respiratory disease history.

{kind=link}
a) Total association between parental respiratory disease history and airway obstruction and respiratory symptoms. b) Indirect (path a and b) and direct (path c') associations between parental respiratory disease history and airway obstruction and respiratory symptoms through life-course factors.
Where relevant, we investigated potential critical period, accumulation-of-risk and chain-of-risks models as per previous studies [22] (see supplementary material for details). The contribution of individual or chain-of-life-course factors to the parental history–offspring symptomatic AO relationship was tested by estimating indirect effects of parental history on offspring symptomatic AO through these factors using path analysis.
Where a combined model, including all life-course factors (of any types) found to be related to offspring, symptomatic AO was estimated to assess whether associations remained significant after inclusions of other factors. Critical period factors and cumulative measure variables were tested in separate models due to the overlap between the variables. When appropriate, correlation between inter-related variables (e.g. smoking and social class) were specified. The proportion of the total effect mediated was estimated from total indirect effects divided by the total (direct and indirect) effects and used to allow comparison across models. This measure is used as a measure of effect size for mediation and has been shown to perform well in samples >500 [23]. The Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) were used to compare model fit with lower values indicating better model fit [24].
All models were adjusted for sex and recent chest infection (past 3 weeks prior to when spirometry was performed at the biomedical sweep at age 45 years). To maximise the analytical sample, multiple imputation was used on variables with >5% missing data [25]. Model testing was conducted on the resulting 10 imputed datasets using the MPlus software (version 8.0, Muthen & Muthen, Los Angeles, CA, USA) [26]
Results
Study sample
Of the 1958 cohort (n=18 336), 9377 participated in the biomedical assessment at 45 years, with lung-function data available for 9090 individuals and data on presence/absence of respiratory symptoms (at 42 years old) available in 8804 individuals. Of these, parental respiratory disease history data were available in 7298 individuals, with a different proportion of missing data in the life-course variables of interest (supplementary figure 1). The final analytic sample included 6212 participants.
Parental respiratory disease history and life-course factors in offspring
Of the total analytic sample, 3.7% reported a positive parental respiratory disease history, 6.2% had symptomatic AO and 50.9% were female. Sex was not associated with parental respiratory disease history.
A summary of the prevalence and associations between parental respiratory disease history and life-course factors in offspring are presented in table 2. Factors associated with parental respiratory disease history included all smoking exposures (except passive smoking exposure in adulthood), social class and asthma at each life stage (and the cumulative measure), low birth weight, childhood pneumonia and adult occupation exposure.
Descriptive statistics of life-course factors in the study sample
Associations between parental respiratory disease history, life-course factors and symptomatic AO
Cohort members with parental respiratory disease history had 91% greater odds (95% CI 1.23–2.97) of developing symptomatic AO compared to those without parental history after adjusting for sex and recent chest infection. Life-period-specific factors related to smoking, social class, asthma and other risk factors were added separately to this base model (table 3, Models 1–4a–c). Parental respiratory disease history and symptomatic AO remained associated when individual life-course factors were added, with the exception of models, including adulthood asthma (Model 3b and c).
Models detailing associations between parental respiratory disease history, individual life-course factors and symptomatic airflow obstruction (outcome), by category (smoking, social class, asthma and others)
Childhood passive smoking and adulthood smoking were related to symptomatic AO when tested separately (Model 1a and b). While the overall or total indirect effect was higher when both childhood passive smoking and adulthood smoking were included (Model 1c) compared to adulthood smoking alone (Model 1b), childhood passive smoking was no longer significantly related to symptomatic AO in this model and adulthood smoking contributed most to the indirect effect. Greater cumulative exposure to smoking was associated with higher odds of symptomatic AO (Model 1d). Social class models revealed that only social class at 42 years was associated with symptomatic AO (Model 2c), with greater odds of symptomatic AO being found with lower social class (SC3: manual and SC4: unskilled). However, there was also evidence for a cumulative effect of social class (Model 2d). Asthma in childhood and adulthood were both related to symptomatic AO when tested separately (Models 3a and b) or jointly (Model 3c), although the only significant indirect effect (p<0.001) was through adulthood asthma. Model 3d indicated a dose–response relationship where cumulative asthma was associated with higher odds of symptomatic AO. Other factors including pneumonia and occupational exposure were also individually associated with symptomatic AO (Model 4b and c).
Combining different types of life-course factors
Factors individually related to symptomatic AO were combined into a critical period model operationalised for specific life periods (Model 5a, table 4) or an accumulation-of-risk model (Model 5b) for cumulative measures. The combined critical period model indicated that only adulthood smoking and childhood and adulthood asthma remained related to symptomatic AO, with evidence of specific indirect pathways through both adulthood persistent smoking (estimate (se)=0.141(0.052), p=0.006) and adulthood asthma (estimate (se)=0.185(0.054), p=0.001). This model explained 58% of the effect of parental respiratory disease history on symptomatic AO. The proportions specifically mediated by adulthood asthma and persistent smoking were 30% and 23% respectively.
Associations between parental respiratory disease history, combined life-course factors and symptomatic airflow obstruction (outcome)
Model 5b (accumulation-of-risk model) included the three cumulative exposure variables, together with childhood pneumonia and occupational exposure. No cumulative exposure measures were available for lifetime pneumonia and occupational exposures, thus only critical period measures of these measures were included in this model. In the accumulation-of-risk model, only cumulative smoking exposure and cumulative asthma measures were associated with greater odds of symptomatic AO and significant indirect effects (table 4). This model explained 51% of the effect of parental respiratory disease history on symptomatic AO, with the proportions of the total effect mediated through accumulation of asthma and accumulation of smoking exposure being 17% and 19%, respectively. Comparison of model fit indices indicated that the critical period model (model 5a) had better fit compared with the accumulation-of-risk model (model 5b).
Discussion
In this sample, adulthood asthma and smoking status together explained about half of the effect of parental respiratory disease history on symptomatic AO. Despite the final model demonstrating that most of the effects were driven by adulthood factors on asthma and smoking, there was also evidence of cumulative effect of exposure behind the development of respiratory impairment and conditions in people with parental respiratory disease history. Beyond smoking history, the combination of parental respiratory disease history and lifetime asthma history may provide an opportunity for early diagnosis and intervention.
Findings of this study were consistent with analysis of an Australian longitudinal cohort study which illustrated the impact of childhood risk factors (including childhood asthma, parental asthma history and exposure to maternal smoking in childhood) that were worsened by adulthood factors (personal smoking and adulthood asthma) [9, 27]. While Bui et al. [27] adjusted for parental asthma history and other childhood risk factors when assessing the associations between asthma and different lung-function trajectories, the focus was not on identifying life-course factors that could explain the relationship between parental respiratory disease history and symptomatic AO in the offspring. In contrast, our study sought to specifically investigate the inter-relationships between these factors and their cumulative effects and provided evidence for the contributing role of chain and accumulation of risk related to asthma and smoking over the life course in explaining the parent–offspring lung health link.
As demonstrated in this analysis, intergenerational transmission of smoking behaviour is complex. When only smoking factors were included (Model 1c), results suggest the chain-of-risk model might be more plausible than an early-life critical period model. While the smoking chain-of-risk model was no longer significant when other life-course factors were considered (Model 5a), the dose–response relationship between the level of smoking exposure and odds of symptomatic AO (Model 5b) indicate support for the cumulative effects of smoking. Genetic and twin studies indicate that the intergenerational transmission of smoking behaviour is probably influenced by the interaction between genes and environment [28, 29]. Exposure to passive smoking has been reported to be predictive of initiation of smoking and smoking status in early adulthood [30]. Parental smoking behaviour has been shown to influence adolescent offspring's initiation of smoking [31]. In addition to social learning of the parent's smoking behaviour, attitudes towards smoking may also be transmitted from parents onto their offspring [32]. This is also reflected in studies that examined the influence of the parent's lifetime smoking trajectory (e.g. never smoker, smoked but quitted, started smoking at an early age and were persistent smokers) on the risk of their adolescent child's initiation of smoking [33]. Individuals who start smoking at a young age and persist into early adulthood (31 years) are more likely to have parents who smoked with lower perceived consequences of smoking [34].
Consistent with findings from previous longitudinal studies, childhood and adulthood asthma were individually associated with poorer later-life lung health [8, 35]. Our findings indicate that the presence of adulthood asthma in the offspring had a significant influence on the association between parent and offspring lung health. While there was no evidence to directly support a chain-of-risk model (parental history through childhood asthma and adulthood asthma to symptomatic AO), the accumulation-of-risk model provided support for the effects of cumulative asthma (Model 5b). The timing of asthma onset has previously been reported to result in differences in the increased risk of AO in current smokers and approximately 27% of people with COPD also have asthma [36]. Bronchodilator reversibility is a key feature distinguishing between asthma and COPD; however, recent findings have indicated that reversibility may not effectively distinguish between the two conditions [37]. As only prebronchodilator spirometric measures were available in this dataset, the outcome of this analysis was not condition-specific.
The presence of respiratory symptoms is a key indicator for consideration of whether to use spirometry to diagnose COPD [2]. Compared with contemporaneous estimates of COPD (2.2% in 2003), a relative high proportion of cohort had symptomatic AO in this study (6.2%) [38, 39]. Those meeting the criteria of symptomatic AO at 45 years probably represent individuals with specific lung-function trajectories, where they may not have obtained their maximal lung function, have accelerated decline in lung function or a combination of both [27]. Repeated analysis using data from cohort members at a more advanced age with post-bronchodilator spirometry may allow greater resolution of mediators and models that explain the relationship between parental respiratory disease history and COPD in offspring.
The major strength of this study was the availability of a range of life-course information collected at multiple time points from a large sample of participants, which allowed the exploration of various life-course factors and their mediation role in the relationship between parental respiratory disease history and cohort AO and respiratory symptoms. A comprehensive list of life-course factors selected from current consensus and evidence on life-course factors were examined in this study [2, 3, 19]. While there was sample attrition within the 1958 cohort at each wave of data collection, the 45-year sample consisted of over 50% of the original cohort and is considered broadly representative of the surviving 1958 cohort [16].
We acknowledge some limitations in this study. Findings of this study may be influenced by healthy survivor bias (supplemental table 1), comparison between key variables indicated a significant difference between the original cohort and the analytic sample which effects the generalisability of the results to the original cohort. Data on parental respiratory disease history were collected across three sweeps (cohort age 0–16 years) and were only available at a system level. Based on the maternal age when the 1958 cohort was born, parental respiratory disease history data were only available until the mothers were in their mid-forties. It is likely that the self-reported positive parental respiratory disease history (3.7%) may be an under-estimate, as it does not capture parental respiratory disease history at an age when chronic lung disease may be more prevalent [2]. The analyses assumed that parental respiratory disease history preceded life-course factors. Future studies with longitudinal data on parental respiratory disease history are needed to verify this assumption.
A recent analysis examined lifetime occupational history and identified selected occupations associated with increased COPD risk in never-smokers and never-asthmatics [37]. Future studies should use a validated job exposure matrix to classify potential occupational exposure, which would minimise the risk of misclassification of potential occupational exposure. Analysis of life-course social trajectories and evaluating the interactions between life-course factors may provide further insight into how this may impact on intergenerational lung health. Some COPD risk factors (e.g. biomass exposure in childhood or outdoor air pollution) were also not explored, as data were not available. Future studies should also evaluate the interactions between smoking and life-course factors
Conclusion
We propose that use of a life-course approach and models can clarify mechanisms behind development of respiratory impairment and conditions in offspring of people with respiratory disease history. The critical period model, including adulthood asthma history and persistent smoking explained the association between parental respiratory disease history and symptomatic AO at 45 years. The analysis provided some evidence supporting the effects of early-life factors and cumulative exposure impacting on the association. Beyond smoking history, the combination of parental respiratory disease history and asthma history may provide an opportunity for early diagnosis and intervention.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00343-2019.SUPPLEMENT
Acknowledgements
We are grateful to the Centre for Longitudinal Studies, University College London Institute of Education, for the use of these data and to the UK Data Service for making them available. However, neither the Centre for Longitudinal Studies nor the UK Data Service bear any responsibility for the analysis or interpretation of these data.
Footnotes
This article has supplementary material available from openres.ersjournals.com
Support statement: L.S.K. Li was supported by an Australian Government Research Training Program Scholarship during the conduct of the study. The funder has no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: L.S.K. Li reports an Australian Government Research Training Program Scholarship during the conduct of the study and grants from the Physiotherapy Research Foundation outside the submitted work.
Conflict of interest: M.T. Williams reports grants from the Medical Research Future Fund Rapid Applied Research Translation Impact Grant Scheme and the Physiotherapy Research Foundation, outside the submitted work.
Conflict of interest: K.N. Johnston has nothing to disclose.
Conflict of interest: P. Frith has nothing to disclose.
Conflict of interest: E. Hyppönen has nothing to disclose.
Conflict of interest: C. Paquet has nothing to disclose.
- Received December 17, 2019.
- Accepted December 17, 2019.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










