





Abstract
With a modified circuit, it is feasible to ventilate two patients with one ventilator over a relevant range of compliances. Adding inspiratory resistance allows individual titration of tidal volume, and incorporating one-way valves prevents pendelluft. https://bit.ly/3ex8SYP
To the Editor:
During health crises, including terrorist attacks or pandemics like coronavirus disease 2019 (COVID-19), the number of mechanical ventilators might fall short of the number of patients with severe respiratory failure [1–3]. A possible emergency solution is to ventilate multiple patients with one ventilator. Sharing ventilators was applied anecdotally during the 2017 Las Vegas (USA) shootings and has raised interest in lay media with the current COVID-19 pandemic [4]. However, ventilating two patients with one ventilator can be dangerous when incorrectly applied. Different setups have been published online, but none have reported any technical safety testing.
Technically, two ventilator circuits can be connected in parallel to one ventilator by adding T-connectors to the inspiratory and expiratory limbs. This was first reported using a setup to ventilate four test lungs, but very limited measurements were presented [5]. Another study demonstrated that ventilating four sheep with one ventilator was feasible for 12 h with frequent blood gases and repositioning [6]. In a more detailed laboratory evaluation, it was concluded that a single ventilator to support four patients is possible, but that tidal volume (VT) cannot be controlled for each subject and depends on respiratory compliance [7]. To what extent different lung compliances affect VT distribution was not described, nor the strategies to control VT individually.
The aim of the current study was to design an improved setup to ventilate two patients with one ventilator and evaluate VT distribution at different lung compliances. Furthermore, we aimed to individualise VT by adding inspiratory resistances (Rinsp) in the circuit.
Methods
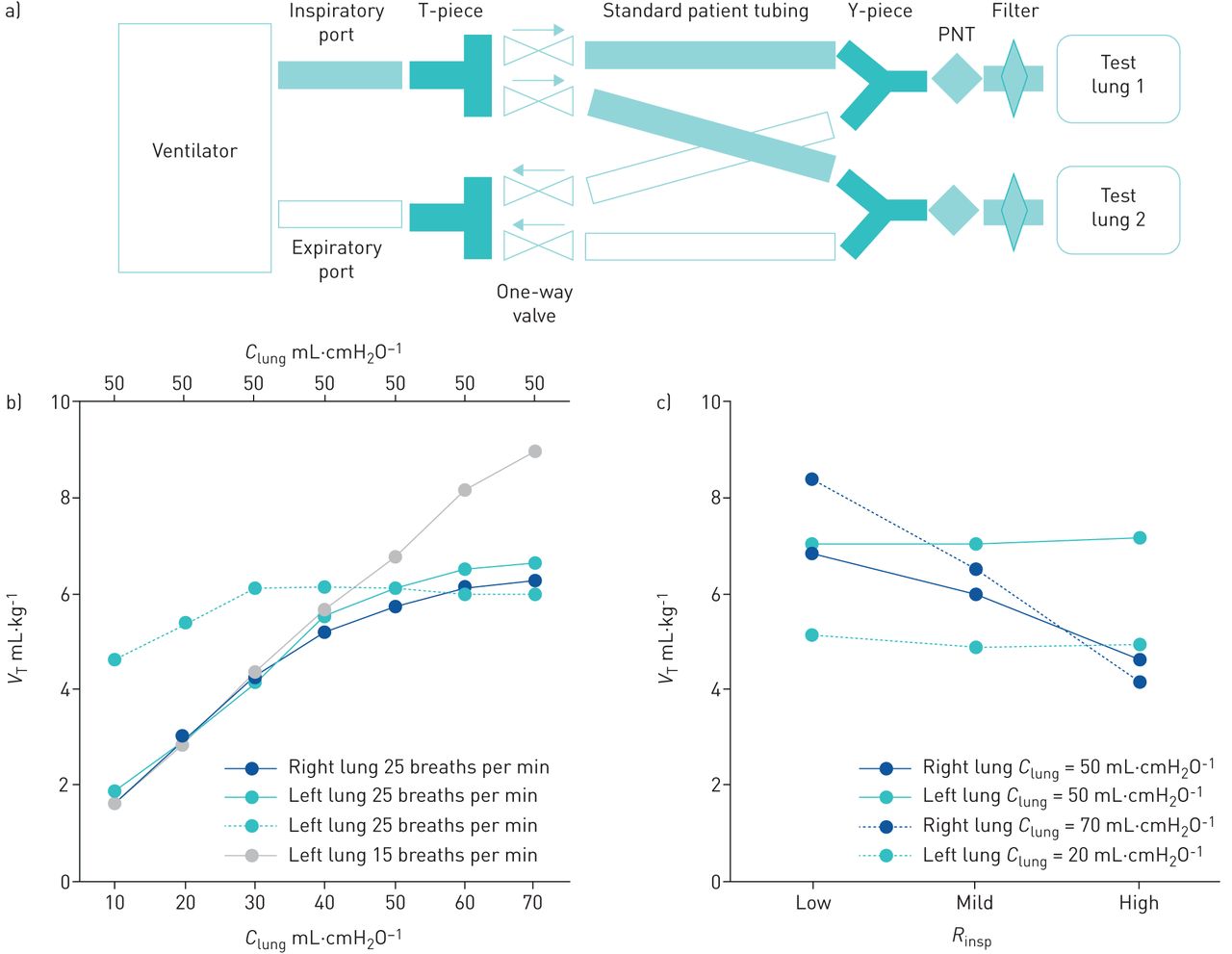
Two breathing circuits (RT380; Fisher & Paykel, Auckland, New Zealand) were connected in parallel to a mechanical ventilator (Evita Infinity V500; Dräger, Lubeck, Germany) by T-connectors with one-way valves (#1954000; Intersurgical, Wokingham, UK) to the inspiratory and expiratory ventilator limbs (figure 1a). The Y-piece of both breathing circuits were connected to a single port of the Dual Adult Lung simulator (Michigan Instruments, Grand Rapids, MI, USA) with calibrated pneumotachographs (Vyntus; Vyaire Medical, Mettawa, IL, USA) and HEPA filters positioned between Y-piece and the test lung.
{kind=link}
a) Experimental setup to connect two patients to one ventilator. Note that the one-way valves in the T-pieces we used were adapted to provide airflow in the shown directions. In our setup, we used a pneumotachograph (PNT) to record separate tidal volumes (VT) and airway opening pressures. In clinical practice, a capnograph or pressure port could also be used to facilitate individual patient monitoring. b) VT distribution between the right and left test lung (blue and green solid lines) at increasing test lung compliance (Clung, lower x-axis) at 25 breaths per min and for the left test lung at 15 breaths per min (grey line). The dashed green line represents VT of the left test lung when Clung,left is kept constant (upper x-axis), while Clung,right is gradually increased (blue solid line, lower x-axis). Note that at very low Clung,right (10–20 mL·cmH2O−1), VT in the left lung becomes lower (dashed green line) despite constant Clung,left. This can be explained by the fast inflation of the right test lung at very low compliance (low time constant), which causes the ventilator to drastically decrease inspiratory flow and thereby averts complete inflation of the left test lung. c) Effect of adding inspiratory resistance (Rinsp) to the right test lung (blue lines). No resistance was added to the left lung. Solid lines represent VT at equal test lung compliances (50 mL·cmH2O−1). Dashed lines represent VT at unequal test lung compliances (Clung,right=70 mL·cmH2O−1, Clung,left=20 mL·cmH2O−1).
Multiple experimental conditions were tested in pressure control (PC) mode (inspiratory time:expiratory time ratio 1:2, positive end-expiratory pressure (PEEP) 12 cmH2O, inspiratory rise time 0.1 s). First, compliance of both test lungs (Clung) was gradually increased (10–70 mL·cmH2O−1) at an inspiratory peak pressure (Ppeak) of 22 cmH2O at 25 breaths per min and thereafter 15 breaths per min. Second, Clung,right was gradually increased while Clung,left was fixed at 50 mL·cmH2O−1. Third, three levels of Rinsp were added to the right test lung by compressing the tube with an adjustable clamp, while no Rinsp was added to the left test lung. Clung was equal in both test lungs (50 mL·cmH2O−1) and Ppeak was set at 30 cmH2O at 15 breaths per min. This experiment was repeated with Clung,right at 70 mL·cmH2O−1 and Clung,left at 20 mL·cmH2O−1. Finally, we simulated coughing by manual compression of one test lung in a setup with and without one-way valves. Measurements for each experimental condition were performed for 1 min. VT to each test lung was calculated as an average over all breaths. VT is expressed in mL·kg−1 considering a patient with a predicted bodyweight of 80 kg.
Results
Figure 1b shows that VT in both test lungs remain comparable when Clung is gradually increased at 25 breaths per min. Due to the longer respiratory time constant at higher compliance and the short inspiratory time there is a deflection in the VT curve, which becomes linear at 15 breaths per min. Increasing Clung,right while keeping Clung,left constant results in a constant VT in the left lung, except for very low compliances. Figure 1c shows that adding resistance to the inspiratory limb of the right test lung decreases VT, while VT in the left test lung remains constant.
In a setup without one-way valves, peak cough pressure, simulated by manual compression of the left test lung, was transmitted to the right test lung (both 10 cmH2O) and 68% of cough volume (190 mL) was inspired by the right test lung. Adding one-way valves to the setup completely prevented this pendelluft effect.
On average, we found that VT measured by the ventilator was 5% higher than the sum of the VT delivered to both test lungs (measured using the pneumotachographs).
Experiments were repeated with other intensive care unit ventilators (Getinge Servo-U/Servo-I, Getinge, Mansfield, UK; Philips Respironics V680, Philips, Guildford, UK; Hamilton Medical G5 and G6, Hamilton Medical, Bonaduz, Switzerland) as well as another breathing circuit (#2000000S, Intersurgical, Wokingham, UK), and provided similar results.
Discussion
The major finding of the current bench study is that with a modified ventilator circuit it is technically feasible to ventilate two patients with one ventilator over a clinically relevant range of compliances in PC mode. Second, adding Rinsp allows individual titration of VT. Third, incorporating one-way valves in the circuit improves safety of the setup by preventing pendelluft.
In agreement with a previous study, VT was distributed evenly between test lungs with a similar compliance [6]. In addition, we tested this over a large range of clinically relevant compliances and found that if compliance changes in one test lung, VT is preserved in the other test lung (except at very low compliance). In other words, changes in respiratory mechanics in one patient will not affect the other patient. This is of clinical relevance because respiratory mechanics in critically ill patients are subject to constant change or differ due to anthropometric differences. Importantly, our findings only apply to PC mode. In volume control mode, changes in respiratory mechanics in one patient, or worse a complete airway obstruction, will distribute VT to the other patient.
By adding Rinsp (i.e. increasing the respiratory time constant) to one test lung, we were able to control VT. As shown in figure 1c, this may facilitate ventilating two patients with different respiratory mechanics with the same protective VT. Note that this only applies when flow does not reach zero at end-inspiration and requires careful monitoring of VT.
In contrast to other studies [5–7], we added one-way valves to the circuit to prevent backflow between patients for two reasons. First, to avoid high pressures, for instance with coughing or airway suctioning, being transmitted to the other patient. Expiratory pressure with coughing may exceed 100 cmH2O. Second, to limit infectious cross-contamination, although this requires further studies.
Recently, multiple professional societies in the USA issued a consensus statement with multiple reasons for avoiding ventilating multiple patients with one ventilator [8]. Many of these reasons apply to volume control modes, which, as discussed here, should be avoided. Furthermore, adding additional Rinsp and one-way valves to the circuit as in our setup allows partial individualisation and prevents pendelluft. Nevertheless, several important practical considerations remain. First, patient breathing effort in PC mode should be absent or ventilator triggering disabled, as triggering by one patient will result in severe patient-ventilator asynchrony for the other patient. This approach is therefore not applicable during weaning. Second, respiratory rate, I:E ratio, inspiratory oxygen fraction and PEEP cannot be individualised. Third, individual monitoring is required and ideally includes capnography, flow and inspiratory pressure near the endotracheal tube, and pulse oximetry. Fourth, alarm settings of VT should be adapted to multiple patients. Stringent alarm limits on VT may be used to monitor whether one of the patient's respiratory mechanics are changing. Finally, we would like to emphasise that our approach is off-label ventilator use and should only be considered in emergency situations, after ethical board approval, consultation of all stakeholders and adequate training.
Sharing ventilators between two patients may be a life-saving rescue intervention in health crisis or in low-resource countries. Future studies should be performed to improve this strategy and further develop clinical safety testing.
Footnotes
Author contributions: F.H.C. de Jongh, H.J. de Vries, L.M.A. Heunks, R. Verdaasdonk and J. Doorduin conceived and designed the study; F.H.C. de Jongh, H.J. de Vries, R.S.P. Warnaar, R. Verdaasdonk and J. Doorduin acquired the data; F.H.C. de Jongh, R.S.P. Warnaar and J. Doorduin analysed the data; F.H.C. de Jongh, H.J. de Vries, R.S.P. Warnaar, E. Oppersma, L.M.A. Heunks, R. Verdaasdonk and J. Doorduin interpreted the data; and F.H.C. de Jongh, H.J. de Vries, R.S.P. Warnaar, E. Oppersma, L.M.A. Heunks, R. Verdaasdonk and J. Doorduin drafted and revised the manuscript.
Conflict of interest: F.H.C. de Jongh has nothing to disclose.
Conflict of interest: H.J. de Vries has nothing to disclose.
Conflict of interest: R.S.P. Warnaar has nothing to disclose.
Conflict of interest: E. Oppersma has nothing to disclose.
Conflict of interest: R. Verdaasdonk has nothing to disclose.
Conflict of interest: L.M.A. Heunks reports a grant from ZonMw (CVID technology grant from Dutch goverment) during the conduct of the study; and a grant from Liberate Medical for expiratory muscle research and a grant from Orion Pharma for a levosimendan study, outside the submitted work.
Conflict of interest: J. Doorduin has nothing to disclose.
Support statement: This study was supported by a grant from “ZonMw program Creative solutions CoVID-19” (number 5000.9953). Funding information for this article has been deposited with the Crossref Funder Registry.
- Received May 8, 2020.
- Accepted May 18, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










