





Abstract
Background The increasing incidence of life-threatening Pneumocystis pneumonia (PCP) in non-HIV immunocompromised patients is a global concern. Yet, no reports have examined the prognostic significance of pre-existing interstitial lung disease (ILD) in non-HIV PCP.
Methods We retrospectively reviewed the medical records of non-HIV PCP patients with (ILD group) or without (non-ILD group) pre-existing ILD. The clinical features and outcomes of the ILD group were compared with those of the non-ILD group. Cox regression models were constructed to identify prognostic factors.
Results 74 patients were enrolled in this study. The 90-day mortality was significantly higher in the ILD group than in the non-ILD group (62.5% versus 19.0%, p<0.001). In the ILD group, patients with a higher percentage of bronchoalveolar lavage fluid neutrophils had worse outcomes compared to those having a lower percentage (p=0.026). Multivariate analyses revealed that pre-existing ILD (p=0.002) and low levels of serum albumin (p=0.009) were independent risk factors for 90-day mortality. Serum levels of β-d-glucan were significantly reduced after treatment of PCP in both groups, whereas levels of Krebs von den Lungen-6 (KL-6) significantly increased in the ILD group. In the ILD group, the 90-day mortality of patients with increasing KL-6 levels after treatment was significantly higher than those with decreasing levels (78.9% versus 0%, p=0.019).
Conclusion In non-HIV PCP patients, pre-existing ILD is associated with a poorer prognosis. Prophylaxis for PCP is needed in patients with pre-existing ILD under immunosuppression.
Abstract
Pre-existing interstitial lung disease (ILD) is an independent prognostic risk factor for non- HIV Pneumocystis pneumonia (PCP). Prophylaxis for PCP is needed in patients with pre-existing ILD under immunosuppression. http://bit.ly/37BGZuK
Introduction
In recent years, the incidence of Pneumocystis jirovecii pneumonia (PCP) in AIDS patients has decreased due to the use of chemoprophylaxis with highly active antiretroviral therapy [1, 2]. However, PCP in non-HIV immunocompromised patients is increasing because immunosuppressive therapies and chemotherapeutic agents have been frequently used in a broad range of diseases, including malignancies and autoimmune disorders [3]. The mortality rate of PCP in non-HIV patients ranges from 19.6% to 52.9% [4–6], which is significantly higher than in HIV-infected patients [1, 6, 7]. Several risk factors, including female sex, co-infections, solid tumours, severe respiratory failure, high lactate dehydrogenase (LDH) levels, delay of initial treatment, low serum albumin and chronic pulmonary diseases, have been reported to be associated with a poor prognosis in non-HIV patients with PCP [5–8]. Few studies, however, have investigated the potential association with pre-existing interstitial lung disease (ILD), which often coexists with underlying diseases such as connective tissue disease (CTD) and lung cancer. Although a high incidence of PCP has been observed in patients with idiopathic pulmonary fibrosis (IPF) receiving corticosteroid therapy [9], it is unclear whether pre-existing ILD is associated with the prognosis of non-HIV PCP patients.
Several studies have described the association of severe infection with a poorer prognosis in patients with ILD [10–12]. Moua et al. [11] reported an in-hospital mortality rate of 49% for fibrotic ILD with acute respiratory failure (ARF) due to various causes including infection. In another study, in-hospital mortality of ILD patients with ARF was 66% [12]. Thus, the mortality of ILD with ARF was relatively high compared with acute respiratory distress syndrome (ARDS) [13, 14]. However, the impact of infection caused by specific pathogens like P. jirovecii on pre-existing ILD remains unclear.
Therefore, we hypothesised that pre-existing ILD would be a risk factor associated with high mortality in non-HIV patients with PCP, and we conducted a multicentre retrospective study to elucidate clinical features and outcomes of this population.
Methods
Patient selection
We retrospectively reviewed medical records of patients who were diagnosed with PCP, with or without pre-existing ILD, who were treated at Kumamoto University Hospital (Kumamoto, Japan) and two affiliated hospitals between December 2008 and December 2018. All patients who were admitted with a diagnosis of PCP were screened for eligibility. Inclusion criteria comprised: 1) acute symptoms including fever, cough, sputum and dyspnoea; 2) newly developed high-resolution computed tomography (HRCT) findings compatible with PCP [15] after developing symptoms; and 3) positive microbiological tests for P. jirovecii confirmed by PCR or Gomori methenamine silver (GMS) stain of samples from bronchoalveolar lavage fluid (BALF) or sputum. Patients with HIV infection or patients whose levels of β-d-glucan in the observational period were <11 pg·mL−1, which was the cut-off value used by the WAKO assay, were excluded. Enrolled PCP patients were subdivided into two groups (ILD group and non-ILD group) according to the presence or absence of pre-existing ILD. HRCT findings of PCP and pre-existing ILD were reviewed by two pulmonologists (S. Hamada and H. Ichiyasu) who were blinded to the patient information. The study protocol was approved by the institutional review board of each participating institution (Kumamoto University Hospital, approval number 1694; Kumamoto Chuo Hospital, approval number 6503; Minamata City General Hospital and Medical Center, approval number 1901).
Definition of pre-existing ILD
Pre-existing ILD was defined according to clinical features and HRCT findings (i.e. pre-existing ground-glass opacity (GGO), consolidation and reticulation shadow in both lung fields). Patients with idiopathic interstitial pneumonias (IIPs), including IPF, were diagnosed according to the international consensus classification of the American Thoracic Society/European Respiratory Society [16]. CTD-ILD, chronic hypersensitivity pneumonia (CHP), chronic eosinophilic pneumonia (CEP), asbestosis and radiation pneumonitis were diagnosed in accordance with established criteria [17–21]. HRCT findings of pre-existing ILD were classified using a previously published clinical practice guideline [22] into two groups: usual interstitial pneumonia (UIP) and non-UIP patterns.
Analysis of BALF
Bronchoalveolar lavage (BAL) was performed through a fibreoptic bronchoscope using standard techniques. The BALF was pooled and centrifuged at 200g for 5 min at 4°C. Cells from BALF samples were resuspended in 10 mL normal saline. The cell differentials were performed on slides prepared in a Cytospin 3 (Shandon, Pittsburgh, PA, USA) centrifuged at 150g for 2 min and stained with a modified Wright–Giemsa technique (Diff-Quik; Sysmex, Kobe, Japan).
Outcomes
The primary outcome was the comparison of PCP-related mortality between the ILD group and non-ILD group. We defined the day when treatments of PCP were initiated as day 0. The patients were followed for 90 days. PCP-related death was defined as death by respiratory failure after diagnosis of PCP. Patients withdrawn from the study due to other causes were censored. Secondary outcomes included the identification of prognostic factors of PCP and changes in serum markers (β-d-glucan and Krebs von den Lungen-6 (KL-6)).
Data collection and statistical analysis
All clinical and laboratory data were collected from patients' medical records. Laboratory examination, HRCT and BAL were performed after the day of developing symptoms, defined as the onset of PCP. Continuous variables are expressed as median (interquartile range) and were compared using the Mann–Whitney U-test. For categorical variables, Fisher's exact test was performed. Survival analysis for all-cause mortality was performed using the Kaplan–Meier method with log-rank test. Cox proportional hazards regression models were used for univariate and multivariate analyses to determine the significant predictors of 90-day mortality, after adjusting for covariates of which the p-values were <0.1. The Wilcoxon signed rank test was used for comparisons of β-d-glucan and KL-6 levels before and after PCP treatment, and between ILD and non-ILD groups. A p-value <0.05 was considered to indicate statistical significance. All statistical analyses were performed using the Statistical Package for the Social Sciences version 20.0 (SPSS Inc., Chicago, IL, USA).
Results
Baseline characteristics
A total of 139 patients were admitted with a diagnosis of PCP during the study period, of whom 89 patients met inclusion criteria (figure 1). 15 patients were excluded due to a HIV-positive diagnosis (n=12) or lack of elevated serum β-d-glucan (n=3). A total of 74 patients were included (ILD group: n=32; non-ILD group: n=42). No significant differences were observed between the two groups with regards to sociodemographic or baseline clinical variables (table 1). Diagnostic procedures for PCP were performed by GMS stain on BALF (25.7%), PCR on BALF (51.4%) and PCR on sputum (31.1%), with no differences between the two groups. There were significant differences in median KL-6 (p=0.001) and arterial oxygen tension (PaO2)/inspiratory oxygen fraction (FIO2) ratio (p=0.025). The median percentage of BALF neutrophils was significantly higher in the ILD group than in the non-ILD group (p=0.012).

Inclusion and exclusion flow diagram. PCP: Pneumocystis pneumonia; GMS: Gomori methenamine silver; ILD: interstitial lung disease.
Patient characteristics
Clinical diagnosis and HRCT pattern of ILD
The clinical diagnosis and HRCT patterns of ILD are shown in table 2. Eight out of 17 patients with IIPs were diagnosed with IPF. 15 patients with non-IIPs were diagnosed with CTD-ILD (n=11), CHP (n=1), CEP (n=1), asbestosis (n=1) and radiation pneumonitis (n=1). 11 patients (34.4%) showed a UIP pattern by HRCT.
Clinical diagnosis and high-resolution computed tomography (HRCT) patterns of interstitial lung disease (ILD)
Treatment for PCP
Therapeutic interventions performed during the study are shown in table S1. There were no significant differences in median days from onset to the initiation of therapy between the ILD group (8.0 days) and non-ILD group (10.3 days). Most patients were treated with trimethoprim/sulfamethoxazole (TMP/SMX) and adjunct corticosteroids. High-dose corticosteroid pulse therapy was applied to 15 patients (46.9%) in the ILD group, which was significantly higher than in the non-ILD group (9.5%, p<0.001).
Outcomes and prognostic factors of PCP
The 90-day mortality rate was 37.8% (28 out of 74) in all subjects and significantly higher in the ILD group (62.5%, 20 out of 32) than in the non-ILD group (19.0%, eight out of 42; p<0.001) (figure 2). After excluding the IIP patients in the ILD group, the 90-day mortality was also significantly higher in the ILD group than in the non-ILD group (53.3% versus 19.0%, p=0.014) (figure S1). In the ILD group, no significant differences in 90-day mortality were observed between patients with IIPs and non-IIPs (70.6% versus 53.3%) (figure S2a) or UIP pattern and non-UIP pattern (72.7% versus 57.1%) (figure S2b).

Kaplan–Meier comparison of survival curves between the interstitial lung disease (ILD) and non-ILD groups. The 90-day mortality was significantly higher in the ILD group than in the non-ILD group (62.5% versus 19.0%). PCP: Pneumocystis pneumonia.
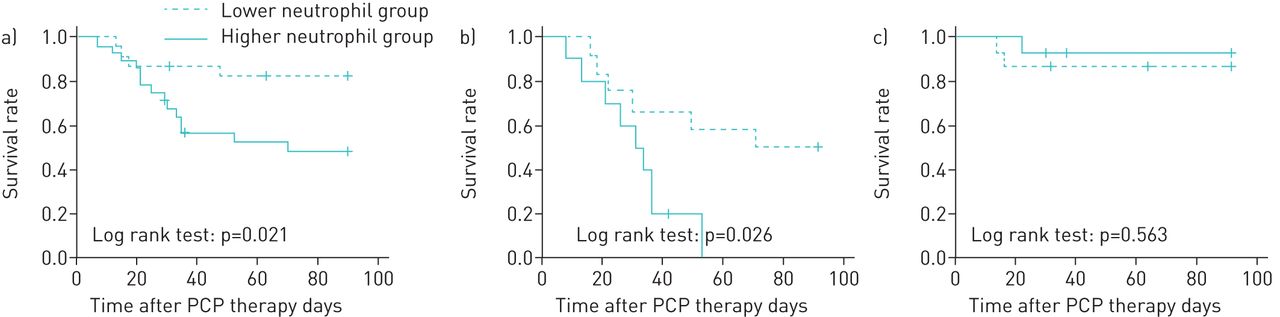
BALF neutrophilia in PCP patients was significantly related to survival rate. The subjects were categorised as a “higher” or “lower” group according to the median value of the percentage of BALF neutrophils. The median percentage of BALF neutrophils was 12.6% across all subjects (ILD group: 22.6%; non-ILD group: 6.6%). BALF neutrophilia was significantly associated with the 90-day mortality rate when taking all subjects into account (higher group: 50.0%; lower group: 17.4%) (p=0.021) (figure 3a) and in the ILD group (higher group: 90.0%; lower group: 50.0%) (p=0.026) (figure 3b). No significant association was found for the non-ILD group (figure 3c).

Kaplan–Meier comparison of survival curves between lower and higher percentage of bronchoalveolar lavage fluid (BALF) neutrophil groups. The patients were categorised into the “higher” or “lower” group according to the median percentage of BALF neutrophils. a) With regards to all subjects as a whole, the 90-day survival was significantly worse in the higher group (n=28) than in the lower group (n=23) (90-day mortality rate in the higher group: 50.0%; lower group: 17.4%). b) In the interstitial lung disease (ILD) group, the 90-day survival was significantly worse in the higher group (n=12) than in the lower group (n=10) (higher group: 90.0%; lower group: 50.0%). c) In the non-ILD group, the 90-day survival was not different between the higher group (n=14) and the lower group (n=15) (higher group: 13.3%; lower group: 7.1%).
We used a Cox hazards model for univariate and multivariate analyses to determine the significant predictors of 90-day mortality. In the univariate analysis, serum albumin, LDH, KL-6, PaO2/FIO2 ratio, C-reactive protein, steroid pulse therapy and pre-existing ILD were covariates with a p-value <0.1 (table 3). In the multivariate analysis, pre-existing ILD (hazard ratio (HR) 5.952, 95% CI 1.900–18.649; p=0.002) and the serum level of albumin (HR 0.312, 95% CI 0.131–0.743; p=0.009) were independent risk factors for 90-day mortality.
Univariate and multivariate analyses of predictors of 90-day mortality
Changes in β-d-glucan and KL-6 after PCP treatment
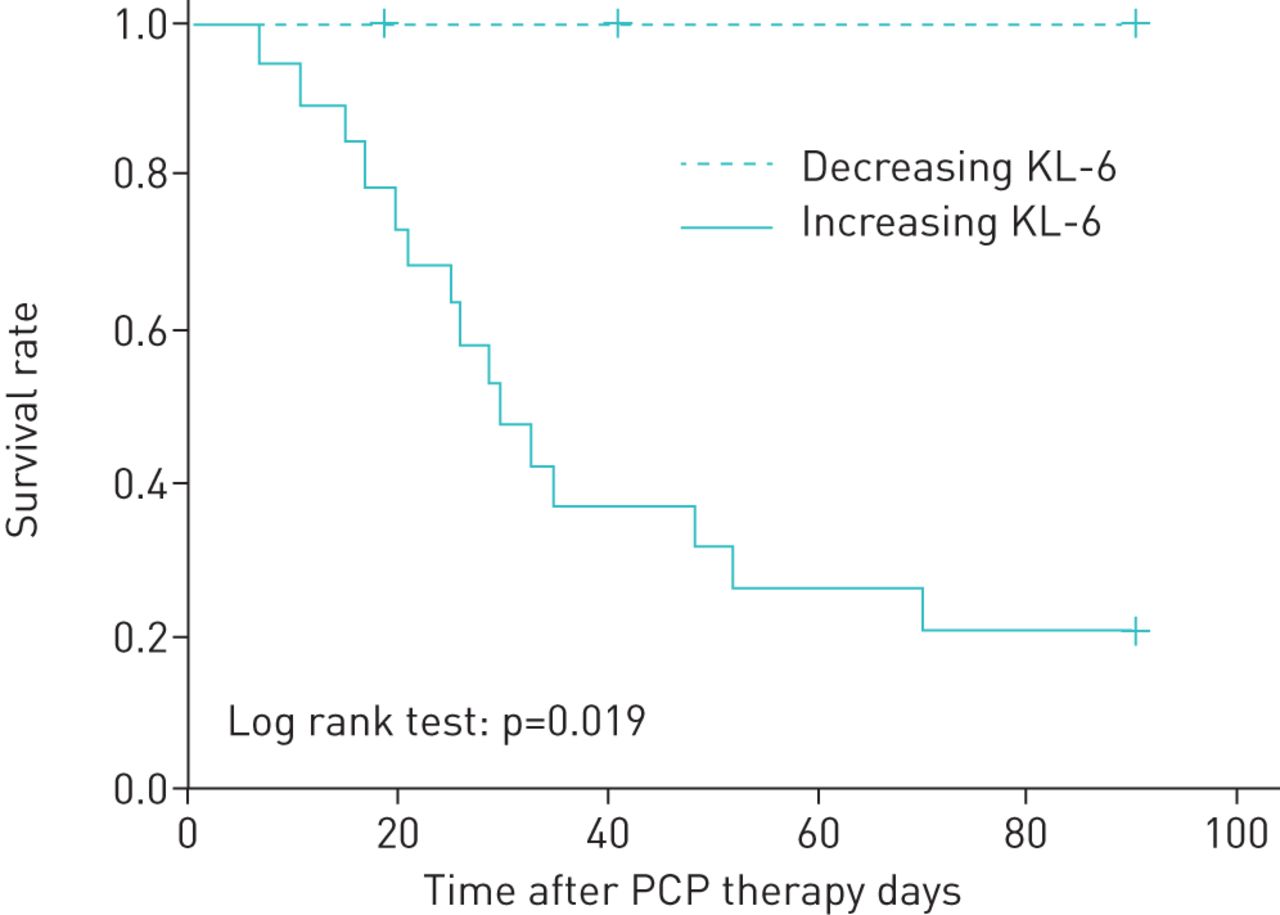
We examined the changes in serum markers associated with PCP and ILD. The levels of β-d-glucan significantly decreased after the treatment of PCP in both the ILD group (p=0.006) (figure 4a) and non-ILD group (p=0.001) (figure 4b). The serum levels of KL-6 significantly increased in the ILD group (p=0.001) (figure 4c) and did not change in the non-ILD group (p=0.249) (figure 4d). In the ILD group, the 90-day mortality of 19 patients with increasing KL-6 after the treatment was significantly higher than that of five patients with decreasing KL-6 (78.9% versus 0%, p=0.019) (figure 5).

Comparisons of serum levels of β-d-glucan and Krebs von den Lungen-6 (KL-6) before and after Pneumocystis pneumonia treatment. The levels of β-d-glucan significantly decreased in both groups: a) median value of the interstitial lung disease (ILD) group from 78.5 to 38.5 pg·mL−1, p=0.006; b) non-ILD group from 95.0 to 27.0 pg·mL−1, p=0.001). c) The level of KL-6 significantly increased in the ILD group (median value from 1505.0 to 2730.0 U·mL−1, p=0.001) and d) did not change significantly in the non-ILD group (median value from 659.5 to 550.0 U·mL−1, p=0.249).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier comparison of survival curves in the interstitial lung disease patients divided by increasing or decreasing Krebs von den Lungen-6 (KL-6) levels after Pneumocystis pneumonia (PCP) treatment. The 90-day mortality of the patients with increasing KL-6 after the treatment was significantly higher than those with decreasing KL-6 (increasing KL-6, n=19: 78.9%; decreasing KL-6, n=5: 0%).
Discussion
We examined the impact of pre-existing ILD on the outcomes of non-HIV PCP. The mortality was significantly higher in the ILD group than in the non-ILD group. Multivariate analysis demonstrated that pre-existing ILD and serum levels of albumin were independent risk factors of 90-day mortality. Furthermore, this is the first study that has reported a significant increase in serum KL-6 levels after treatment of non-HIV PCP in patients with pre-existing ILD and a concurrent decrease in serum β-d-glucan levels.
Several risk factors, such as low serum albumin, high LDH and severe respiratory failure, have been shown to be associated with poorer prognosis in non-HIV patients with PCP [5–8]. In a recent review examining underlying diseases as risk factors for mortality, Liu et al. [6] reported a significant association for the presence of solid tumours. While coexisting pulmonary diseases have been reported as risk factors for developing PCP [23], the impact of pre-existing ILD on outcomes of PCP was unknown. A small study examining 20 non-HIV patients with PCP, including four patients with pre-existing ILD, reported a significant association between ILD and a high 90-day mortality [24]. Aoki et al. [25] investigated prognostic indicators in 25 PCP patients with CTD and concluded that pre-existing CTD-ILD was one of the prognostic factors leading to death. Nevertheless, there has been a lack of studies that have mainly focused on pre-existing ILD in non-HIV PCP. In our study, all patients with pre-existing ILD, which was regarded as an underlying disease of PCP or comorbid condition, were assigned to the ILD group. Consequently, a greater number of patients with pre-existing ILD were included in the present study than in previous studies, and we showed that pre-existing ILD was an important predictor for a poorer prognosis.
Severe PCP is characterised by intense neutrophilic pulmonary inflammation associated with diffuse alveolar damage (DAD), which is also observed as the typical pathological finding of ARDS and acute exacerbation (AE) of ILD, including AE-IPF [26–29]. According to our analysis of BALF cellular profiles, the percentage of BALF neutrophils was significantly higher in the ILD group than in the non-ILD group and this factor was significantly associated with a poorer prognosis. These results suggest that in patients with PCP, pre-existing ILD may increase susceptibility to the development of DAD, namely AE-ILD, leading to refractory respiratory failure. However, in the non-ILD group, the degree of BALF neutrophilia was not associated with the survival rate. This contrasts with several studies that have reported that BALF neutrophilia may be a significant prognostic factor associated with fatality in patients with non-HIV PCP in the absence of pre-existing ILD [30, 31]. While the reasons for this discrepancy are unclear, previous studies have reported that the extent of lung damage in neutrophil-impaired knockout mice with PCP were unexpectedly the same as in wild-type mice, and CD8+ T-cell-mediated responses might be more directly responsible for lung injury than neutrophil-mediated inflammation [32, 33]. As only limited previous data on the prognostic utility of BALF cellular analysis in non-HIV PCP are available, further research is required to elucidate the exact role of neutrophils in the pathogenesis of PCP.
The serum level of KL-6 is known to be useful for not only detecting the presence of ILD and evaluating disease activity, but also for the diagnosis of PCP [34, 35]. In the present study, serum levels of KL-6 were elevated at the time of PCP diagnosis, regardless of the presence or absence of pre-existing ILD, and the elevation of KL-6 was higher in the ILD group than in the non-ILD group. While KL-6 levels were significantly increased in the ILD group and did not change in the non-ILD group after PCP treatment, levels of β-d-glucan were significantly reduced in both groups. These paradoxical changes in KL-6 and β-d-glucan levels in the ILD group might be attributed to the progressive and refractory characteristics of pre-existing ILD after treatment for PCP. Furthermore, in the ILD group, the mortality of patients with increasing KL-6 was significantly higher compared to patients with decreasing KL-6. Yokoyama et al. [36] also reported that an increase in KL-6 after treatment predicted poorer outcomes in cases of rapidly progressive IPF, including AE-IPF, suggesting that the monitoring of KL-6 may be useful for the management of active IPF. The utility of KL-6 measurement in PCP patients, with or without ILD, needs to be addressed in future studies.
In our study, the prognosis of the ILD group was very poor despite sufficient treatment. Notably, no patients in the ILD group had received prophylaxis for PCP with TMP/SMX. In a meta-analysis investigating the efficacy of prophylaxis for non-HIV immunocompromised patients, the incidence of developing PCP was 6.2% in the control group versus 0.9% in the prophylaxis group [37]. Although some attending physicians in our study did not perform or discontinued prophylaxis due to renal or hepatic disorders and side-effects such as skin rash and leukopenia (data not shown), we suggest that it is prudent to provide prophylaxis for PCP whenever possible in patients with pre-existing ILD under immunosuppression.
This study has several limitations. First, this was a retrospective study employing a small sample, and did not randomise patients to treatment and control groups. Second, the underlying comorbid conditions were heterogeneous and could have affected the outcomes of PCP treatment. Third, there was insufficient previous laboratory data regarding KL-6 and β-d-glucan measurements before the onset of PCP, and newly developed GGO could be observed in both PCP and AE-ILD. Furthermore, the diagnosis of PCP was based on PCR results in three-quarters of all patients, and false positive results may have occurred due to colonisation by P. jirovecii as opposed to true infection. Therefore, we could not completely distinguish PCP from AE of pre-existing ILD. Nevertheless, the levels of β-d-glucan were significantly elevated at diagnosis in all patients and reduced after PCP therapy in most patients, suggesting a more accurate diagnosis of PCP than in prior studies [38].
In conclusion, our study indicates that pre-existing ILD is associated with a poorer prognosis in patients with non-HIV PCP. Therefore, prophylaxis for PCP should be considered, especially in patients with pre-existing ILD under immunosuppression.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Table S1 00306-2019.SUPPLEMENT
Figure S1 00306-2019.figureS1
Figure S2 00306-2019.figureS2
Acknowledgements
We would like to acknowledge all the participants. The authors would like to thank Editage (https://www.editage.jp) for the professional English language review.
Footnotes
This article has supplementary material available from openres.ersjournals.com
Conflict of interest: S. Hamada has nothing to disclose.
Conflict of interest: H. Ichiyasu has nothing to disclose.
Conflict of interest: M. Inaba has nothing to disclose.
Conflict of interest: H. Takahashi has nothing to disclose.
Conflict of interest: T. Sadamatsu has nothing to disclose.
Conflict of interest: K. Akaike has nothing to disclose.
Conflict of interest: A. Masunaga has nothing to disclose.
Conflict of interest: Y. Tashiro has nothing to disclose.
Conflict of interest: N. Hirata has nothing to disclose.
Conflict of interest: T. Yoshinaga has nothing to disclose.
Conflict of interest: T. Sakagami has nothing to disclose.
- Received November 6, 2019.
- Accepted February 11, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










