





Abstract
Aim A subgroup of children with obstructive sleep apnoea (OSA) requires treatment with continuous positive airway pressure (CPAP). This study's aims were: 1) to determine if the optimal CPAP for the treatment of OSA in children correlates with body mass index (BMI); 2) to determine the correlation between polysomnographic variables and optimal CPAP in children with OSA; and 3) to develop a CPAP predictive equation for children with OSA.
Methods This was a retrospective study of children with OSA who underwent CPAP titration studies. Patients with craniofacial abnormalities (except Down syndrome) and neuromuscular diseases were excluded. Polysomnograms were done using Sandman Elite. Correlations between optimal CPAP, clinical and polysomnographic variables were analysed. A multivariable linear regression model for optimal CPAP was developed.
Results 198 children (mean±sd age 13.1±3.6 years) were studied. Optimal CPAP had a significant positive correlation with age (rho=0.216, p=0.002), obstructive apnoea-hypopnoea index (rho=0.421, p<0.001), 3% oxygen desaturation index (rho=0.417, p<0.001), rapid eye movement respiratory disturbance index (rho=0.378, p<0.001) and BMI z-score (rho=0.160, p=0.024); and a significant negative correlation with arterial oxygen saturation measured by pulse oximetry nadir (rho= −0.333, p<0.001). The predictive equation derived was:
Optimal CPAP (cmH2O)=6.486+0.273·age (years)−0.664·adenotonsillectomy
(no=1, yes=0)+2.120·Down syndrome (yes=1, no=0)+0.280·BMI z-score.
Conclusion The equation developed may help to predict optimal CPAP in children with OSA. Further studies are required to validate this equation and to determine its applicability in different populations.
Abstract
A predictive equation may help derive the optimal CPAP for the treatment of obstructive sleep apnoea in children http://bit.ly/2wTf6Bw
Introduction
Obstructive sleep apnoea (OSA) is characterised by habitual snoring and repeated episodes of partial or complete upper airway obstruction that compromises normal gas exchange and sleep architecture [1]. Globally, habitual snoring occurs in approximately 7% of school-aged children and 2–4% of children who snore suffer from OSA [2]. Other common symptoms of OSA in children include restless sleep, mouth breathing, bed wetting and witnessed apnoeas [3]. Derangements in gas exchange during sleep result in repeated arousals, hypoxia and hypercapnia [4]. If left untreated, this may lead to: 1) neurocognitive deficits, including impaired executive function and learning, behavioural problems, poor attention and hyperactivity, 2) cardiovascular sequelae including systemic hypertension, and 3) metabolic derangements, including insulin resistance and dyslipidaemia [5–7].
Treatment of OSA comprises medical and surgical therapy. Medical therapy includes weight management and treatment of allergic rhinitis [8]. Given that adenotonsillar hypertrophy is the most common cause of OSA in children, adenotonsillectomy (AT) is the primary surgical treatment for most children with OSA [9]. However, a considerable proportion of children suffer from residual OSA after AT, ranging from 13 to 29% in those without comorbidities, and up to 73% in those with comorbidities such as obesity [9].
For patients with residual OSA after AT or contraindications to surgery, continuous positive airway pressure (CPAP) is often recommended [9]. CPAP acts as a pneumatic splint for the nasopharyngeal airway to prevent its collapse during sleep [10]. Currently, overnight manual titration with polysomnography (PSG) is considered as the gold standard for determining the optimal CPAP level required to treat OSA [11]. However, this is costly, time consuming, resource intense and is not easily available in many settings. This has prompted exploration of methods to expedite the process through split-night CPAP titration studies, auto-CPAP titration and the use of CPAP predictive equations [12, 13]. CPAP predictive equations for adults have been reported by several authors; however, given the differences in the clinical phenotype of paediatric OSA compared to adult OSA [14–16], equations derived based on adult data may not be appropriate for children.
Body mass index (BMI), a variable frequently examined in CPAP predictive equations [13], is of particular interest, given the rising global trend in childhood obesity. For children aged 2–19 years, overweight and obesity are defined as BMI between the 85th and 94th percentiles and >95th percentile respectively, for age and sex [17]. Obesity affects 10–15% of children in Singapore [18]. The relationship between OSA and obesity in children is well recognised [9]; the incidence of OSA in obese children is much higher, ranging from 13 to 66% [18]. Obesity also plays an important role in the higher prevalence (30–50%) of OSA in children with Down syndrome (DS) [19]. However, current literature acknowledges the insufficient evidence for choosing a higher CPAP level a priori, when initiating CPAP based on clinical grounds and during CPAP titration studies, for children with higher BMI [11]. Although adult studies have suggested a correlation between BMI and optimal CPAP levels, no such data exist for children. If such a correlation is evident in children, this may aid in initiating CPAP and planning CPAP titration studies in children with OSA.
The objectives of this study were: 1) to determine whether optimal CPAP for the treatment of OSA in children correlates with BMI; 2) to determine the correlation between PSG variables and optimal CPAP in children with OSA; and 3) to develop a CPAP predictive equation for children with OSA.
Materials and methods
In this retrospective study, we reviewed the clinical, anthropometric and PSG data of children aged 2–18 years who underwent either CPAP titration or split-night CPAP titration studies for the treatment of OSA at KK Women's and Children's Hospital, Singapore, between January 2009 and June 2018. All children were diagnosed with OSA on a preceding diagnostic overnight PSG. Children with known syndromes (except DS), craniofacial abnormalities, neuromuscular diseases, and skeletal deformities were excluded. This study was approved by the SingHealth Centralised Institutional Review Board.
Baseline PSGs and CPAP/split-night CPAP titration studies were conducted using a Sandman Elite sleep diagnostic system (Natus Neurology Inc., Embla Systems, Ontario, Canada). The American Academy of Sleep Medicine (AASM) guideline for manual titration of CPAP was used for titration studies [11]. The sleep studies were scored and reported by qualified paediatric sleep physicians as per the AASM guideline [20]. Data were collected from electronic records. Anthropometric and clinical variables included age, sex, race, height, weight, BMI, history of AT (performed after baseline PSG) and OSA severity. BMI z-scores are measures of relative weight adjusted for the child's age and sex. BMI z-scores at the time of CPAP/split-night CPAP titration studies were calculated using the World Health Organization AnthroPlus software version 1.0.4 [21] for children without DS, and the Canadian Paediatric Endocrine Group calculator [22] for children with DS. OSA severity was defined as mild, moderate or severe, according to the obstructive apnoea-hypopnoea index (OAHI) (see Appendix A). PSG variables collected from baseline diagnostic PSGs included OAHI, rapid eye movement respiratory disturbance index (REM RDI), arterial oxygen saturation measured by pulse oximetry nadir (SpO2 nadir), 3% oxygen desaturation index (ODI3) and optimal CPAP (see Appendix B for definitions). The optimal CPAP was defined as the CPAP level that best controlled respiratory events in the patient during the titration study. The grading of CPAP titration studies was assigned as per the AASM guideline [11] (see Appendix C).
Statistical analysis
Categorical variables were reported as frequencies with proportions, whereas continuous variables were expressed as mean±sd. Normality assumption was checked using a Shapiro–Wilk test. One-way ANOVA (or Kruskal–Wallis test) was used to compare mean optimal CPAP and OSA severity. Fisher's exact test was used to compare the grading of CPAP titration studies and split-night CPAP titration studies between the non-DS and DS subgroups. Spearman's rank correlation was calculated between optimal CPAP and baseline clinical, anthropometric and PSG variables, including age. Univariable and multivariable linear regression models were fitted to examine the relationship between optimal CPAP and baseline variables. The full model was adjusted for the baseline variables presented in the model. In order to ensure validity of the results, we checked multicollinearity (where variance inflation factor >10) between variables, heteroscedasticity assumption and distribution of residuals for goodness-of-fit. To handle missing data in the regression analysis, we used fully conditional multiple imputation with 25 imputations and 1000 iterations using Markov chain Monte Carlo method [23]. Model summary estimates were calculated based on Rubin's rule [24]. Results from the multiple imputation regression models were presented as main results and the complete case analysis results are available in the supplementary material (see Appendix D). The overall statistical significance level was set at 5% probability with a two-tailed hypothesis test for all analyses. All statistical analyses were performed using Stata version 15.1 (StataCorp, College Station, TX, USA) and SPSS Statistics version 25 (IBM, Chicago, IL, USA).
Results
198 children (mean±sd age 13.1±3.6 years, 142 (71.7%) males) underwent CPAP titration or split-night CPAP titration studies during the study period. The demographic, clinical and PSG data from the baseline diagnostic PSG are summarised in table 1. Additionally, two subgroups (non-DS (n=175) and DS (n=23)) were identified. Of note, there were only 10 (5%) children aged ≤6 years in the study group.
Demographic, clinical and polysomnography (PSG) data
Correlations between optimal CPAP and baseline PSG variables are given in table 2 and the supplementary material (see Appendix E). Overall, there was a significant positive correlation between optimal CPAP and age (rho=0.216, p=0.002), OAHI (rho=0.421, p<0.001), ODI3 (rho=0.417, p<0.001), REM RDI (rho=0.378, p<0.001) and BMI z-score (rho=0.160, p=0.024); and a significant negative correlation between optimal CPAP and SpO2 nadir (rho= −0.333, p<0.001). Subgroup analyses showed a significant positive correlation between BMI z-score and optimal CPAP in the non-DS subgroup (rho=0.263, p<0.001) but not the DS subgroup (rho=0.251, p=0.249). Optimal CPAP correlated positively with age and ODI3 in both subgroups, and with OAHI and REM RDI in the non-DS subgroup only. The significant negative correlation between optimal CPAP and SpO2 nadir was observed only in the non-DS subgroup.
Correlation between optimal continuous positive airway pressure and baseline variables
Of the clinical and PSG variables, univariable regression identified age, diagnosis of DS, OAHI, ODI3, REM RDI, SpO2 nadir and BMI z-score as potential predictive variables associated with optimal CPAP. Using a multivariable linear regression analysis, a predictive equation for optimal CPAP was derived with age, AT history, diagnosis of DS and BMI z-score as predictor variables (table 3). This model accounted for 31.4% of the variance in optimal CPAP (adjusted R2=0.314). No significant multicollinearity or heteroscedasticity was observed. The predictive equation (variables with p<0.1) was:
Univariable and multivariable linear regression analysis to determine predictors of optimal continuous positive airway pressure (n=198)
Optimal CPAP (cmH2O)=6.486+0.273·age (years)−0.664· adenotonsillectomy (no=1, yes=0)+2.120·DS (yes=1, no=0)+0.280·BMI z-score.
Data on optimal CPAP in relation to OSA severity are given in table 4. In the non-DS subgroup, optimal CPAP was significantly higher in those with severe OSA compared to mild-to-moderate OSA (p<0.001). However, the distribution of optimal CPAP in the DS subgroup did not vary by OSA severity (p=0.257).
Mean optimal continuous positive airway pressure according to obstructive sleep apnoea (OSA) severity (n=198)
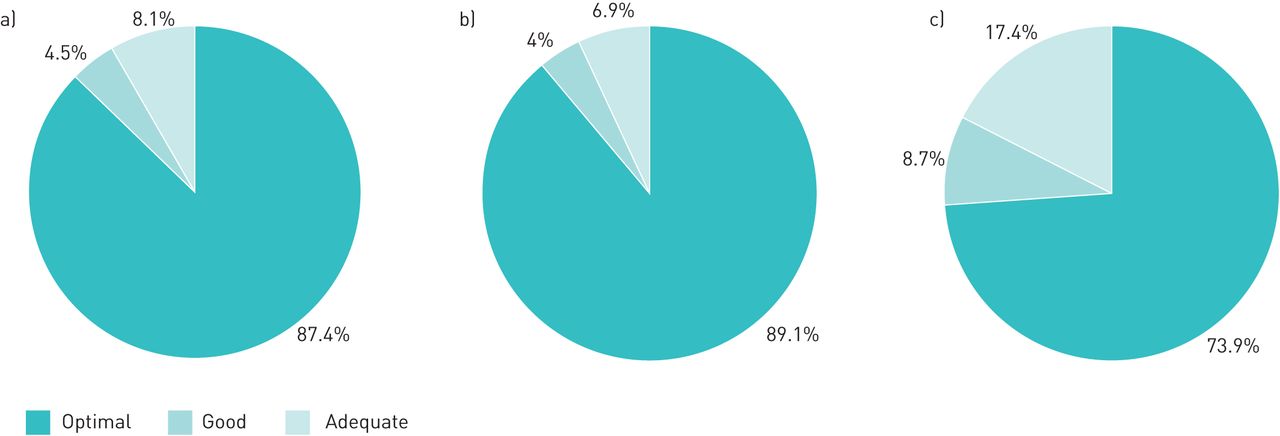
Data on the grading of CPAP titration and split-night CPAP titration studies are presented in figure 1. In the non-DS subgroup, 89.1% had an optimal CPAP titration study, compared to 73.9% in the DS subgroup. Overall, there was no significant difference in the proportion of children with various titration study gradings between the non-DS and DS subgroups (p=0.072).
{kind=link}
Grading of continuous positive airway pressure (CPAP) and split-night CPAP titration studies in a) the whole group (n=198), b) non-Down syndrome subjects (n=175) and c) Down syndrome subjects (n=23).
Discussion
Our data show that BMI z-score has a significant positive correlation with optimal CPAP in non-DS, but not DS children with OSA. We have also shown that optimal CPAP correlates positively with age and ODI3 in both subgroups, and with OAHI and REM RDI in the non-DS subgroup. A significant negative correlation between optimal CPAP and SpO2 nadir was shown in the non-DS subgroup. A predictive equation for optimal CPAP was derived using age, AT history, diagnosis of DS and BMI z-score.
To our knowledge, this is the first study describing the correlation between optimal CPAP and clinical, anthropometric and baseline diagnostic PSG data in a well-characterised cohort of children with OSA. The CPAP predictive equation derived in this study includes variables such as age, AT history and the diagnosis of DS that have never been included in previous CPAP predictive equations for adults with OSA [13]. As children age, they experience maturational changes in their adenotonsillar size and craniofacial morphology [16]. The resultant alterations in upper airway dimensions may necessitate a higher CPAP to maintain airway patency, explaining the significant positive correlation between age and optimal CPAP observed.
Given that the frequency of adenotonsillar hypertrophy in paediatric OSA is higher than in adult OSA [14, 16], the inclusion of AT history in the predictive equation is particularly relevant in children. Intuitively, within subject, one would expect the optimal CPAP after AT to be lower than pre-AT. However, the predictive equation suggests a higher optimal CPAP for children who have undergone AT. This observation may have several explanations. There is a suggestion that after AT, children may maintain the craniofacial morphological changes developed secondary to adenotonsillar hypertrophy [25]. Additionally, weight gain and an increase in BMI percentile after AT is well recognised [26] and this may necessitate a higher optimal CPAP despite previous AT in some children. Furthermore, children with residual OSA after AT may have had more severe OSA to begin with, due to underlying comorbidities (e.g. obesity and allergic rhinitis) that persist after AT, which may explain the need for a higher CPAP [7, 27]. Confirmation of this observation would require further studies that include data from CPAP titration studies before and after AT in cohorts matched for baseline characteristics.
Children with DS were included in this study, given the relatively larger subgroup sample size compared to those with other rarer syndromes involving craniofacial dysmorphism. Additionally, children with DS are known to have a higher risk of residual OSA after AT and hence have a greater need for CPAP compared to the general paediatric population [28]. The higher optimal CPAP in children with DS compared to those without may be explained by differences in craniofacial morphology, such as midface hypoplasia, relative macroglossia, and lingual tonsillar hypertrophy; as well as hypotonia and exaggerated upper airway collapsibility [29].
BMI has been found to be the most common variable in CPAP predictive equations for OSA treatment in non-DS adult populations [13]. However, since BMI percentiles that define overweight and obesity are related to age and sex in children [30, 31], the strength of this study lies in the fact that we used BMI z-scores rather than raw BMI data to better analyse the correlation between BMI and optimal CPAP in children. Obese children have increased subcutaneous fat deposition in the neck and fatty infiltration of the tongue, resulting in increased pharyngeal collapsibility [6, 32]. Additionally, fat deposition around abdominal viscera and thoracic walls may compromise the lung volume [6, 32]. These factors may account for the positive correlation between BMI z-score and optimal CPAP observed in the non-DS subgroup. In children with DS, the relative influence of craniofacial anatomical differences on optimal CPAP may explain why BMI z-score alone had no significant correlation with optimal CPAP.
While previous studies of non-DS adult populations have included sex in their predictive equations [13], sex was not found to be a statistically significant variable to predict optimal CPAP in children. In the prepubertal paediatric population, OSA affects both sexes equally [33]. After puberty, however, OSA incidence is higher in males due to testosterone-mediated muscle mass enlargement in the upper airways [16]. This sex effect was not reflected in our predictive equation as this study included similar proportions of prepubertal and post-pubertal children.
Race was initially evaluated as a predictor due to the importance of race and ethnicity in the pathogenesis of OSA [13]. Differences in optimal CPAP between Asian and white adults have been attributed to racial variations in craniofacial morphology [34]. However, race adjustment was eventually dropped from this study's model. As this study analysed Asian children primarily, the number of white people included may have been insufficient to elucidate the correlation between race and optimal CPAP. The results of this study also suggest that the differences in craniofacial features of Chinese, Malay and Indian children in Singapore do not affect optimal CPAP. Future studies may consider including cephalometric measures in the linear regression analysis to confirm this observation.
This study has few limitations. Due to its retrospective design, data on other anthropometric indices of central adiposity, such as waist and neck circumference, were not available and hence their correlation with optimal CPAP could not be determined. Such indices have been shown to correlate significantly with optimal CPAP [13] and if evaluated together with BMI z-score, may help refine the correlation between central adiposity and optimal CPAP in children with OSA [35]. Formal sample size calculation was not done as the number of patients who underwent CPAP titration and/or split-night CPAP titration studies at KK Women's and Children's Hospital in the given timeframe was limited, hence all eligible children were included in the study. We did not include a separate cohort of children with OSA for validation of the CPAP predictive equation, hence, the clinical applicability of the formula cannot be confirmed at present. Moreover, as CPAP tolerance may be variable across the paediatric age range, when commencing CPAP for the first time, some children may not tolerate the level of CPAP predicted based on the equation and may require a lower starting CPAP level which may then be gradually increased to the predicted optimal CPAP, as tolerated. The DS subgroup sample size in this study was small. Hence, future studies may include a larger sample size to re-examine the relationship between optimal CPAP and BMI z-score in children with DS. In this study, we were not able to assess the within-subject difference in optimal CPAP before and after AT. In routine clinical practice, most children with OSA would undergo medical therapy and AT as the first-line treatment before CPAP is considered as a treatment option and hence determining pre- and post-AT optimal CPAP level is often not possible. Given the diverse racial variation in Singapore, the applicability of this study to other populations with different ethnic origins may be limited.
Despite these limitations, this study, for the first time assessed the correlation between optimal CPAP and baseline variables including clinical, anthropometric and diagnostic PSG data in a well-characterised group of children with OSA and developed a predictive equation for optimal CPAP. Once validated in prospective cohorts, the CPAP predictive equation may be helpful in 1) selecting a starting CPAP level closer to the optimal CPAP a priori during CPAP titration studies, thereby increasing the probability of achieving an optimal CPAP titration in a single night; 2) using clinical bedside titration as a substitute for manual titration in a sleep laboratory in resource-limited settings and when factors such as patient immobility or critical illness preclude formal manual CPAP titration studies; and 3) helping clinicians recommend a CPAP level closer to the optimal CPAP when initiating CPAP in the home setting, improving treatment efficacy and patient adherence [36, 37].
In conclusion, this study showed a significant positive correlation between the optimal CPAP level and BMI in non-DS children with OSA but not in children with DS and OSA, providing evidence for selecting a higher starting CPAP pressure a priori during CPAP titration studies in obese children. The optimal CPAP predictive equation that we developed would need further validation in prospective studies in different paediatric patient populations.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00312-2019.SUPPLEMENT
Footnotes
This article has supplementary material available from openres.ersjournals.com.
Conflict of interest: J. Chong has nothing to disclose.
Conflict of interest: R. Bajpai has nothing to disclose.
Conflict of interest: O.H. Teoh has nothing to disclose.
Conflict of interest: A. Pugalenthi has nothing to disclose.
Conflict of interest: J.C. Allen Jr has nothing to disclose.
Conflict of interest: Z.R. Cheng has nothing to disclose.
Conflict of interest: S.G. Tan has nothing to disclose.
Conflict of interest: M. Lim has nothing to disclose.
Conflict of interest: J. Tan has nothing to disclose.
Conflict of interest: A. Goh has nothing to disclose.
Conflict of interest: Y.H. Tan has nothing to disclose.
Conflict of interest: B. Thomas has nothing to disclose.
- Received November 11, 2019.
- Accepted March 10, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










