





Abstract
Asthma is a chronic inflammatory airway disease. Increase in airway inflammation is hypothesised to contribute to worsening of asthma symptoms and deterioration in lung function, resulting in the use of reliever medication. Short-acting β2-agonists only treat the symptoms, whereas an anti-inflammatory reliever is believed to treat both symptoms and the underlying inflammation, thereby arresting the progression to an exacerbation. As-needed budesonide/formoterol as an anti-inflammatory reliever reduces the risk of severe exacerbations. However, supporting mechanistic evidence has not yet been described, specifically the temporal dynamics of parameters including airway inflammation, over time and during asthma worsening.
The STIFLE study aims to characterise daily variability in airway inflammation, symptoms, lung function and reliever use in people with asthma. This phase IV, open-label, parallel-group, multicentre, exploratory study will enrol 60–80 adult patients with asthma receiving low- or medium-dose inhaled corticosteroids/long-acting β2-agonists (EudraCT identifier number 2018-003467-64). Participants will be randomised 1:1 to either as-needed budesonide/formoterol dry-powder inhaler or salbutamol reliever for 24 weeks, in addition to their maintenance therapy. Daily data will be captured for fractional exhaled nitric oxide, spirometry, asthma symptoms and medication use using devices connected to a smartphone via the STIFLE application. STIFLE will thereby enable not only characterisation of the variability of airway inflammation and clinical outcomes in relation to asthma worsening, but also elucidate the effect of as-needed budesonide/formoterol on airway inflammation against a background of daily maintenance therapy.
Abstract
Using novel, home-based tools to generate new insights into the link between inflammation and asthma attacks, the STIFLE study aims to increase understanding of the mechanisms behind the benefits of budesonide/formoterol anti-inflammatory reliever therapy https://bit.ly/33X1wJU
Introduction and study rationale
Asthma is a chronic inflammatory disease of the airways [1]. The inflammation is variable in terms of intensity and is heterogeneous, with well-characterised subtypes that have different responses to therapy [1, 2]. In parallel, variability in lung function, asthma symptoms and reliever medication use are commonly observed over days and weeks [3–5]. Often, these periods, beyond baseline day-to-day or week-to-week variability, are interspersed with significant exacerbations of symptoms [6], necessitating increased reliever use and, potentially, the use of oral corticosteroids [7].
Treatment with inhaled corticosteroids (ICS) is the cornerstone of asthma management [7] and treatment strategies targeted at inflammation (via maintenance of a normal airway eosinophil count) have been shown to reduce the risk of severe exacerbations compared with strategies based on assessment of symptoms, lung function and use of rescue treatment [8]. However, many patients, regardless of the underlying disease severity, are not adherent with such treatment and rely on short-acting β2-agonists (SABAs) for rapid relief of asthma symptoms [9]. Such over-reliance on SABAs is a concern since their excessive use may worsen asthma control and increase the risk of fatal or near-fatal asthma [10, 11]. A SABA does not address the underlying inflammation and increases the risk of exacerbations [12]. In addition, even in patients whose disease is apparently controlled and who are adherent to maintenance medication, exacerbations may still occur [9]. This suggests that, in such a variable condition, patients' requirement for anti-inflammatory therapy varies and, in turn, represents an argument in favour of providing increased doses of ICS when symptoms worsen. To this end, a combination of budesonide/formoterol (ICS/fast-onset but long-acting β2-agonist (LABA)) as maintenance and reliever therapy has been studied in several randomised controlled trials in patients with moderate-to-severe asthma [5, 13–16]. Results from these trials have demonstrated that as-needed use of budesonide/formoterol as an anti-inflammatory reliever in addition to daily maintenance therapy is highly effective in reducing the risk of severe exacerbations, with up to a 47% reduction versus comparator regimens that utilise a SABA as a reliever [5, 13, 16]. In addition, as-needed budesonide/formoterol has been evaluated as a treatment option for patients with mild asthma, as assessed in the SYGMA (Symbicort Given as Needed in Mild Asthma) programme [17, 18], the PRACTICAL (Personalised Asthma Combination Therapy: with Inhaled Corticosteroid and Fast Onset Long-Acting Beta Agonist) study [19] and the Novel START (Novel Symbicort Turbuhaler Asthma Reliever Therapy) study [20]. In the latter study, the risk of severe exacerbations was lower in the as-needed budesonide/formoterol group compared with as-needed SABA, a finding that was paralleled by a reduction in exhaled nitric oxide fraction (FENO), consistent with an effect of as-needed budesonide/formoterol on airway inflammation [20].
Hypothesis of the STIFLE study: use of anti-inflammatory reliever therapy in the “window of opportunity”
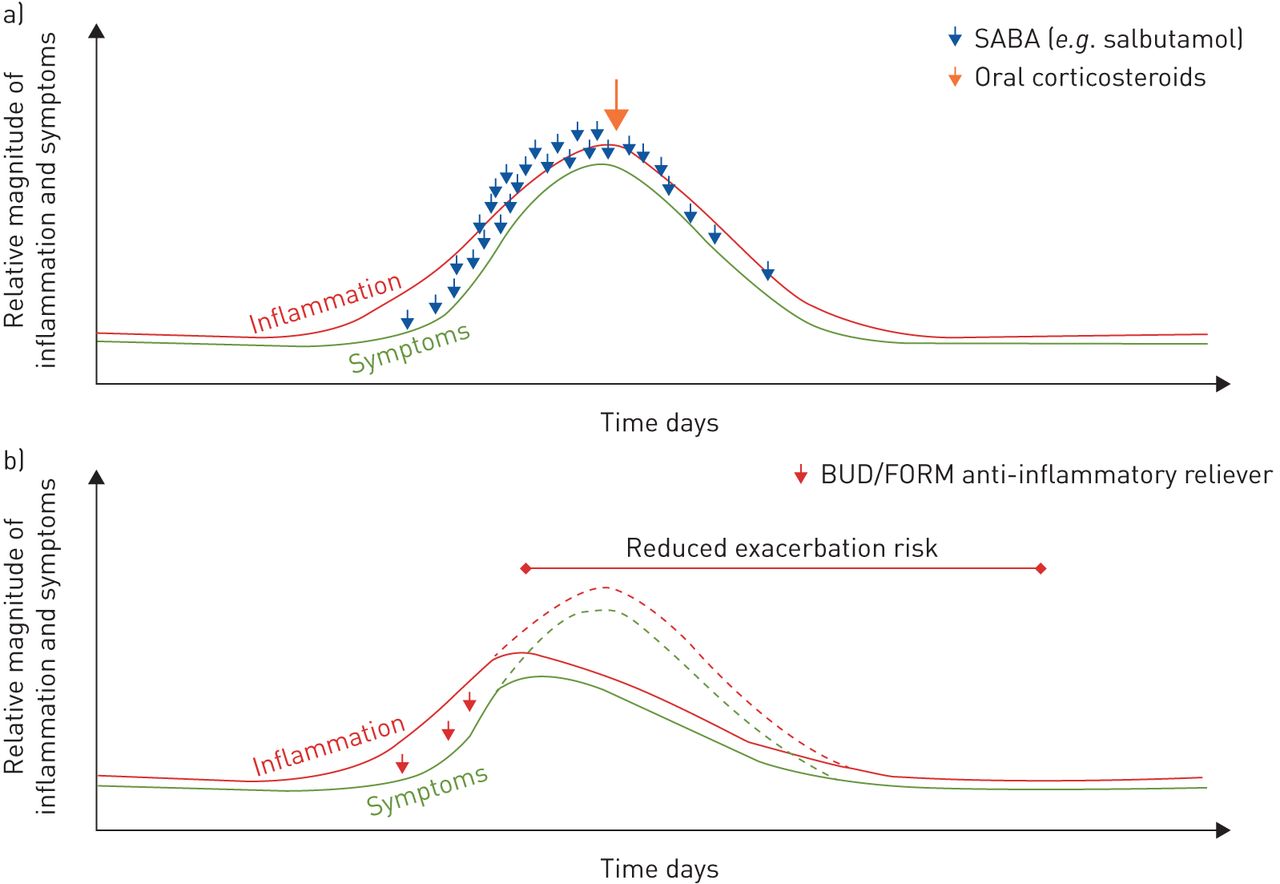
The benefits of anti-inflammatory reliever therapy in reducing the risk of exacerbations are hypothesised to be due to additional anti-inflammatory ICS therapy received at pivotal times [21], specifically during the “window of opportunity” when inflammation-driven symptoms start to worsen (figure 1 and supplementary video) [22, 23]. This is based on the work of Tattersfield et al. [23], who evaluated all severe exacerbations that occurred in the FACET (Formoterol and Corticosteroids Establishing Therapy) study. Exacerbations were characterised by a gradual fall in peak expiratory flow (PEF) over 5–7 days, followed by a more rapid fall over 2–3 days prior to an exacerbation. Furthermore, the change in PEF occurred in parallel with an increase in symptoms and the use of SABA reliever, suggesting that a 2–3-day window of opportunity exists when patients experience deteriorating symptoms and lung function but have not yet deteriorated to the stage of requiring oral corticosteroids. Indeed, a post hoc analysis of FENO data from the CHARISM (Childhood Asthma Respiratory Inflammatory Status Monitoring) study showed an increase in FENO ∼10 days before a moderate exacerbation, with a significant increase 3 days beforehand [24]. Together, these findings highlight an early opportunity to adjust treatment with an increase in ICS to target the underlying flare-up of airway inflammation, thereby arresting progression to exacerbation. In addition, against a background of budesonide/formoterol maintenance therapy, as-needed formoterol demonstrated better exacerbation control than a SABA [14], likely due to a stabilising effect on airway smooth muscle. Furthermore, LABAs may be particularly active against noneosinophilic exacerbations [25].
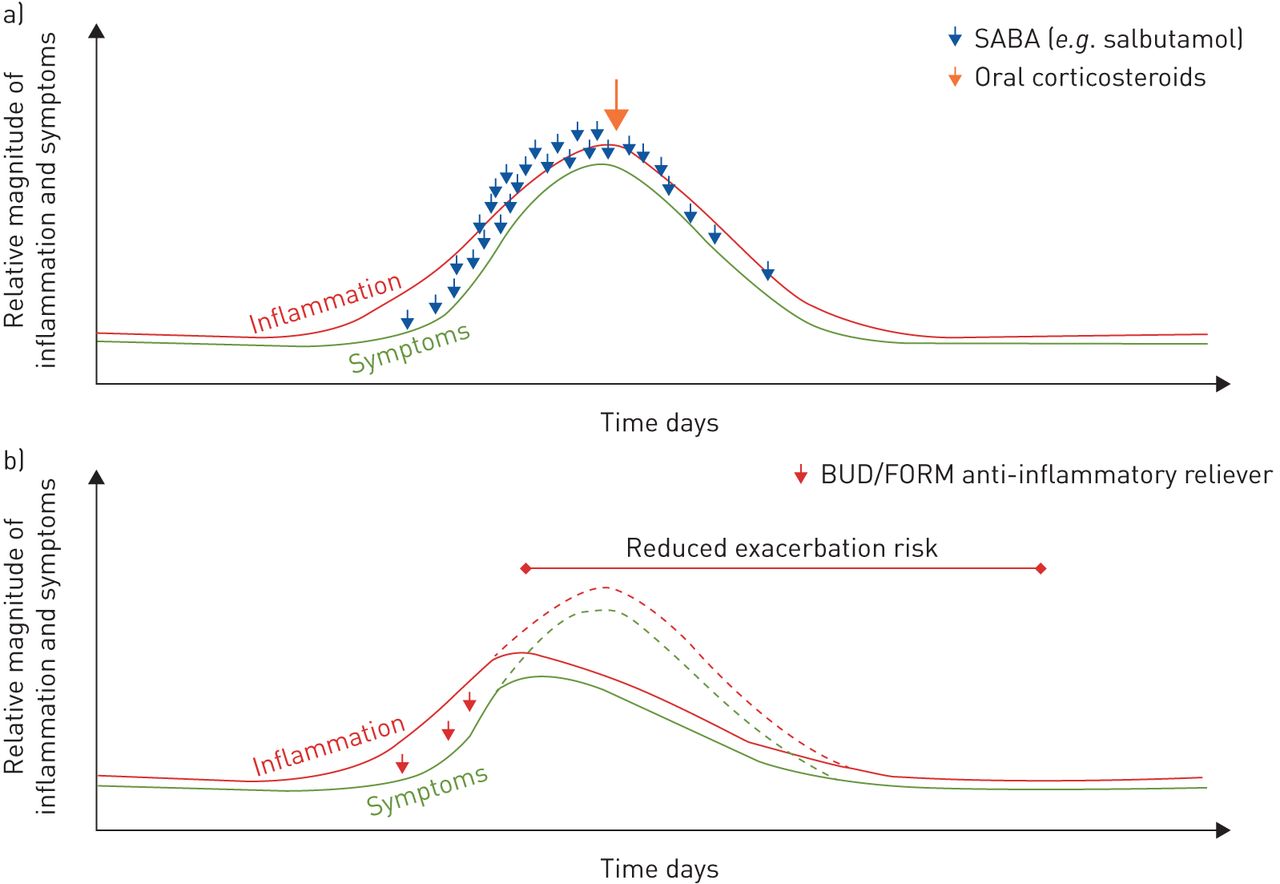
Proposed hypothesis of the mechanism of a) short-acting β2-agonist (SABA) reliever and b) as-needed budesonide (BUD)/formoterol (FORM) as anti-inflammatory reliever therapy during worsening of asthma symptoms that precedes an exacerbation. The effects of FORM are likely to be more complex and are not presented in the graphs. SABA treats only symptoms and not the underlying inflammation. Anti-inflammatory reliever therapy treats both symptoms and the underlying inflammation. Dashed lines indicate asthma worsening in patients with SABA reliever use.
However, supporting mechanistic evidence has not yet been described for as-needed budesonide/formoterol, specifically the nature of the variations and temporal dynamics (patterns or trends with respect to time) of airway inflammation, symptoms, lung function and reliever use, both over time and during periods of symptom worsening. Consequently, the STIFLE study (EudraCT identifier number 2018-003467-64) has been designed to characterise the day-to-day relationship between such parameters, and specifically in relation to worsening of symptoms in patients with asthma receiving as-needed budesonide/formoterol anti-inflammatory reliever or a SABA, against a background of budesonide/formoterol maintenance therapy.
Design of the STIFLE study
STIFLE is a phase IV, randomised, active-comparator, open-label, parallel-group, multicentre, exploratory, 24-week study in adult asthma patients (≥18 years of age) receiving Global Initiative for Asthma 2018 [26] step 3 or step 4 treatment (low- or medium-dose ICS/LABA only). The study aims to characterise variability in inflammation (FENO), symptoms, lung function and reliever use, on a daily basis, over time (primary objective) and in the period surrounding an event (secondary objective). Events include severe exacerbation, Composite Endpoint for Exacerbations (CompEx) [27], a single day with six or more occasions of reliever medication use and FENO >50 ppb (table 1). Key inclusion and exclusion criteria are shown in table 2. This study will consist of a screening visit (visit 1), a 2-week run-in period, a baseline visit (visit 2) and a 24-week treatment period (visits 3 and 4) (figure 2). During the run-in period, patients will receive maintenance budesonide/formoterol 100/6 µg or 200/6 µg dry-powder inhaler, two inhalations twice daily (based on ongoing low- or medium-dose ICS/LABA, respectively, at study entry) and SABA reliever (salbutamol 100 µg) as needed. At visit 2 (baseline visit, week 1), eligible patients will be randomised 1:1 (stratified by ongoing low- or medium-dose of ICS/LABA at study entry) to receive maintenance budesonide/formoterol (100/6 µg or 200/6 µg, two inhalations twice daily) with either as-needed budesonide/formoterol (same dose as maintenance) or salbutamol (100 µg) as reliever for 24 weeks. Additional visits will be scheduled if a patient meets any of the criteria for an event during the treatment period, including the first occurrence of a severe exacerbation, symptom worsening (decrease in PEF, increase in reliever use or asthma symptoms) or a single day with six or more occasions of reliever medication use. Informed consent will be obtained from all patients prior to initiation of study-related procedures, sampling and analysis.
STIFLE study objectives and endpoints
Key inclusion and exclusion criteria

Study design. BMI: body mass index. #: patients on low-dose inhaled corticosteroid (ICS)/long-acting β2-agonist (LABA) at study entry will receive budesonide (BUD)/formoterol (FORM) 100/6 µg and those on medium-dose ICS/LABA at study entry will receive BUD/FORM 200/6 µg. ¶: randomisation criteria are adherence (completed ≥80% of asthma assessments (exhaled nitric oxide fraction (FENO) and spirometry measurements, and completing the asthma symptom diary) at home during the run-in period) and reliever medication use (used reliever medication for 2–8 days out of the last 10 days of the run-in period). +: event visit assessments are prior and concomitant medication (days 1 and 12), serious adverse events (AEs) and AEs leading to treatment discontinuation, clinical chemistry, urinalysis, haematology (including eosinophils), spontaneous sputum for inflammatory biomarkers, nasal absorption samples for inflammatory biomarkers, blood sample (eosinophil-derived neurotoxin and C-reactive protein), plasma and serum samples for exploratory biomarkers. §: daily assessments at home are FENO, peak expiratory flow (PEF) and forced expiratory volume in 1 s (FEV1), and completing the asthma symptom diary before taking the study medication in the morning; and PEF and FEV1, and completing the asthma symptom diary before taking the study medication in the evening.
All patients will be provided with a kit containing a smartphone and four devices (a FENO monitoring device (Vivatmo Me; Bosch, Waiblingen, Germany), a spirometer (Spirobank Smart; MIR, Rome, Italy) and two inhaler sensors (SmartTurbo and SmartTouch; Adherium, Auckland, New Zealand)) connected to the smartphone via the STIFLE application (AstraZeneca, Cambridge, UK) and will receive training on its use. Daily, at home, patients will perform FENO measurements (morning) and spirometry assessments (PEF and forced expiratory volume in 1 s (FEV1), morning and evening) and complete an asthma symptom diary that includes reliever medication use (morning and evening). Data from these four devices and an embedded asthma symptom diary will be recorded in the STIFLE application through an integrated approach (figure 3). ∼30 patients who agree to participate in a nasal biomarker substudy of STIFLE will be shown how to collect a nasal absorption sample (synthetic absorptive matrix (SAM) [28]), and will be provided with a kit and instructions for collecting the samples at home. These patients will collect daily morning nasal samples for the first 30 days of randomised treatment for the evaluation of inflammatory biomarkers.
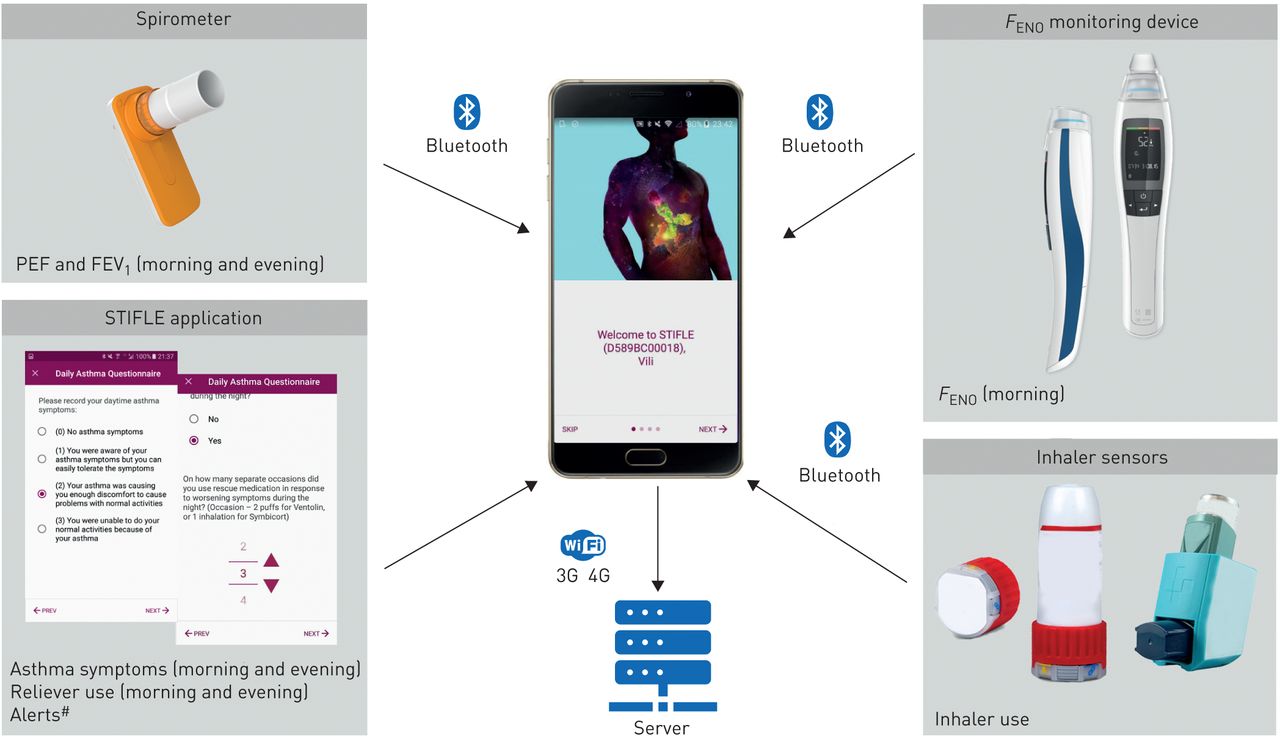
Integrated approach to data collection. PEF: peak expiratory flow; FEV1: forced expiratory volume in 1s; FENO: exhaled nitric oxide fraction. #: the patient and the investigator will receive alerts from the STIFLE system regarding event visits (in relation to the exploratory objective event) due to symptom worsening (based on peak expiratory flow (PEF), reliever use and symptom score criteria) or due to a single day with six or more occasions of reliever medication use. Patients will also be instructed to contact the study site to arrange an event visit if they experience a severe exacerbation. Patients and investigators will be blinded to all data collected from these devices. Asthma symptoms during the night and day will be recorded by the patient twice daily in the asthma symptom diary, according to the following scoring system: 0, no asthma symptoms; 1, “you are aware of your asthma symptoms, but you can easily tolerate the symptoms”; 2, “your asthma is causing you enough discomfort to cause problems with normal activities (or with sleep)”; 3, “you are unable to do your normal activities (or to sleep) because of your asthma”.
At all clinic visits, FEV1 will be assessed (by clinic spirometry equipment), safety (adverse events) will be evaluated, and blood samples will be collected for haematology (including eosinophils), clinical chemistry and C-reactive protein analyses. 60–80 patients will be randomised from three sites in the UK to achieve ≥50 patients who will complete the 24-week study. It is anticipated that half of these patients will meet the criteria for an event.
A short review: FENO
Daily measurement of FENO is an important methodological component of the STIFLE study. FENO is a simple, noninvasive, quantitative, highly sensitive and safe measure of airway inflammation [29]. FENO is a surrogate marker for eosinophilic airway inflammation and is used to determine the potential need for and likelihood of response to ICS, to optimise the doses of anti-inflammatory medications, and to unmask poor adherence to ICS [29]. A strength of the STIFLE study is that we will measure FENO concentrations daily, against a background of maintenance ICS therapy, to determine if variability in FENO around the time of an exacerbation can be detected and, therefore, whether it is a useful biomarker of type 2 inflammation in a cohort of treated patients with moderate asthma.
How will the STIFLE study help understand the day-to-day relationship between airway inflammation, symptoms and lung function in patients with asthma?
To our knowledge, STIFLE will be the first study specifically designed to investigate daily airway inflammatory patterns and associated variability in symptoms, lung function and reliever medication use in patients with asthma. An increase in airway inflammation is thought to contribute to worsening of asthma symptoms and deterioration in lung function, requiring the use of reliever medication. However, the time perspective of various parameters before and after asthma worsening is largely unknown, including the order of appearance, magnitude and timeframe in relation to worsening. Therefore, the STIFLE study will help clarify these differences and provide an understanding of the temporal dynamics of these parameters, and specifically in relation to asthma worsening.
High “as-needed” reliever use is a robust measure of asthma instability [22]. Results from an exploratory analysis of two randomised controlled trials reported that budesonide/formoterol maintenance and anti-inflammatory reliever therapy reduced the incidence of high reliever use episodes (more than six inhalations a day) and exacerbation burden immediately following these high-use episodes compared with ICS/LABA maintenance plus SABA reliever therapy [22]. Consequently, STIFLE will also help establish whether the hypothesised mechanistic benefit of as-needed budesonide/formoterol as anti-inflammatory reliever relates to the timely and rapid suppression of airway inflammation (and related symptoms) by ICS during the window of opportunity [21, 22], as compared with only symptom relief provided by a SABA (figure 1). The concentration of ICS in lung tissue has been shown to decline over time (between maintenance doses) [30], with concentrations being ∼10% of peak values within 6 h of inhalation; thus, as-needed ICS may help restore concentrations when the levels of ICS are suboptimal between scheduled maintenance doses [14]. The importance of increasing ICS dosing frequency is supported by the results of a crossover study in 34 adult asthma outpatients where greater efficacy was consistently observed with budesonide four times daily dosing compared with two times daily dosing, while providing the same total daily dose [31]. In addition to the timely increase in ICS dose, the rapid onset of action of ICS is of particular importance, with a wealth of evidence supporting the rapid anti-inflammatory effect of inhaled budesonide (with or without formoterol) [32–35]. Indeed, results from a randomised controlled trial in 41 patients with stable asthma reported a significant reduction in sputum eosinophils and an improvement in airway responsiveness within 6 h of budesonide inhalation [32]. Furthermore, a systemic anti-inflammatory effect on circulating lymphocytes within 30 min of inhalation with budesonide/formoterol has been demonstrated [34]. Additionally, budesonide/formoterol has been reported to prevent asthma deterioration and significantly improve baseline FEV1 at 30 min following a low-dose allergen exposure in patients with intermittent allergic asthma [35].
Notably, the STIFLE study will incorporate several important methodological components. The main outcomes will be based on daily measurements, including local airway inflammation as measured by FENO concentrations taken at home. To date, very few studies have evaluated FENO in the setting of acute exacerbations and those that have report varying results [36–38]. Results from a cross-sectional study in a paediatric emergency department reported that FENO concentrations during an exacerbation did not correlate with asthma severity and had limited utility in the management of acute asthma [36]. In contrast, in adult patients with moderate-to-severe asthma, a significant increase in FENO concentrations during exacerbations compared with baseline in certain patients was reported [37]. In a sample of emergency department patients with acute exacerbations of asthma, FENO measurements were poorly reproducible and did not correlate with asthma severity [38]. However, a significant increase in FENO was reported during 3 days before until 4 days after moderate exacerbations in children with asthma [24]. The results from STIFLE are therefore expected to contribute to this knowledge base. Although FENO measurements have been implemented in many asthma trials, including studies utilising daily, domiciliary methods for capturing FENO [39, 40], a novel aspect of this study is that daily home assessments of FENO will be used to determine variability and to compare with other parameters (lung function, reliever use and symptoms) in a real-time environment to assess maintenance plus SABA versus maintenance plus anti-inflammatory reliever therapy over 6 months.
A potential limitation of using FENO measurements is that rhinitis and allergic comorbidities in patients with asthma may also lead to changes in FENO levels [41]. However, in addition to FENO, other biomarkers of inflammation, such as sputum and blood eosinophils, eosinophil-derived neurotoxin, and nasal absorption biomarkers, will also be measured to explore patterns of inflammation. As patients will be performing FENO and spirometry assessments at home, it is necessary that they use these devices correctly. Spirometers can be difficult to use in the community and challenging to interpret. However, all patients are trained on device use. Moreover, there is a precedence for the use of the spirometer in the home environment [42, 43].
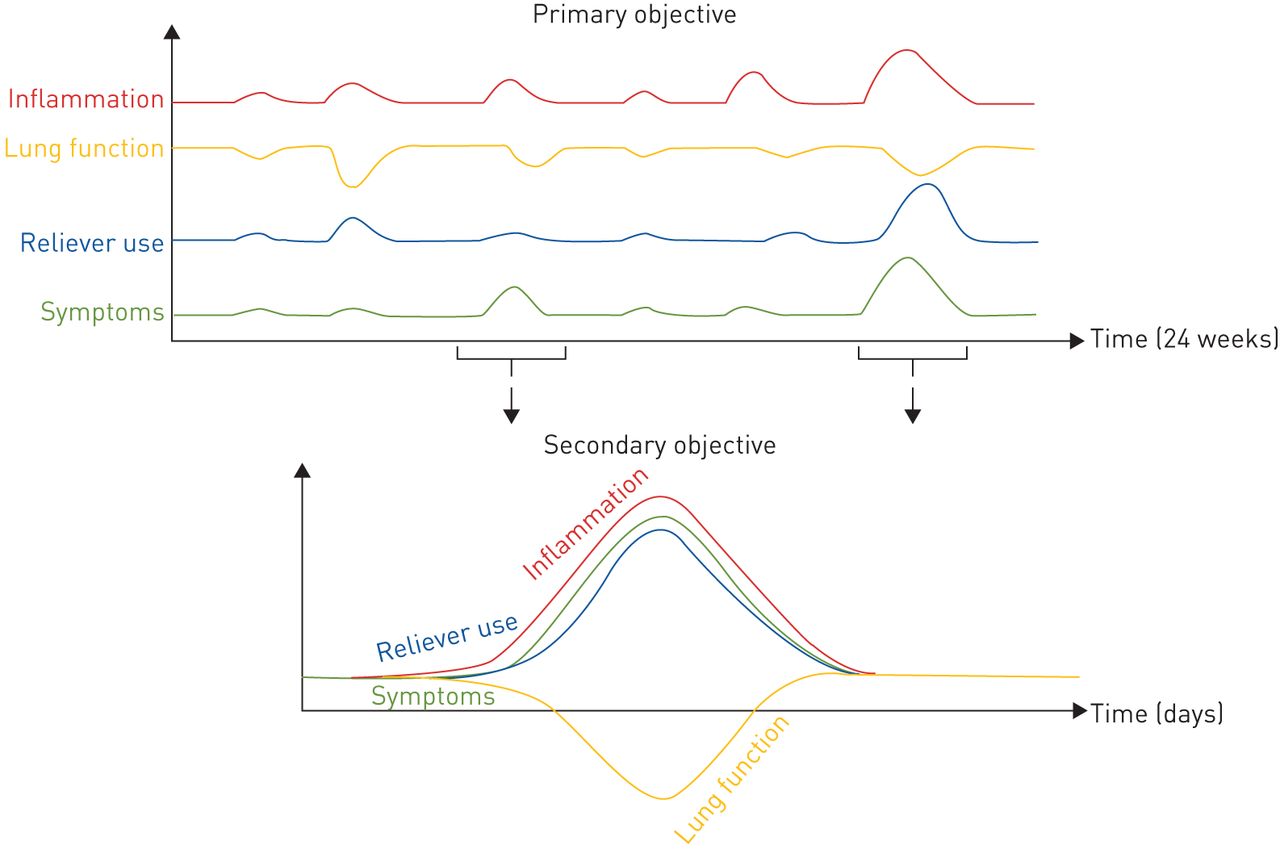
Another important feature of the study design of STIFLE is the examination of the temporal dynamics of clinical parameters and local inflammation in relation to an event (figure 4), which may provide insights into the inflammatory mechanism of worsening symptoms and lung function and highlight the benefits of an anti-inflammatory reliever compared with a SABA reliever. Notably, STIFLE will include patients on a background of ICS/LABA maintenance since variability in lung function, asthma symptoms and reliever medication use are also observed in patients receiving such therapy [5, 9], many of whom continue to be at risk of exacerbations even when adherent to therapy [44].
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Examination of endpoints over 24 weeks and specifically in relation to an event. The graphs are for representation only. The variables may or may not show parallel changes at a specific time point. Results from the STIFLE study would potentially provide an understanding of the temporal dynamics of these parameters.
STIFLE will also be among one of the first prospective studies to use CompEx, an extended definition of asthma exacerbations that combines diary-based events (clinically relevant asthma deteriorations) with the traditional definition of severe exacerbations [27]. Since severe exacerbations are rare events, clinical trials using such events as the primary outcome measure require large sample sizes and a long study duration to evaluate treatment effects. Thus, CompEx, which mirrors results observed with the severe exacerbation-validated outcome [27], was incorporated into the STIFLE study because it allows for the evaluation of clinically relevant worsening in this clinical trial of short duration and with relatively few patients.
Conclusion
In summary, the temporal dynamics of clinical parameters and airway inflammation are largely unknown in patients with asthma, and the mechanistic evidence for the anti-inflammatory effect of as-needed budesonide/formoterol has not been described. STIFLE is expected to provide insights into the real-time day-to-day relationship between airway inflammation, lung function, asthma symptoms and reliever use in such patients, including the temporal dynamics of various parameters surrounding events. Results will further elucidate the anti-inflammatory effect of budesonide/formoterol as an anti-inflammatory reliever against a background of regular maintenance therapy.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00333-2019.SUPPLEMENT
Acknowledgements
Medical writing support was provided by Sudha Korwar of Cactus Communications (Mumbai, India), which was funded by AstraZeneca in accordance with Good Publication Practice guidelines (www.ismpp.org/gpp3).
Footnotes
This study is registered at https://eudract.ema.europa.eu/ with identifier number 2018-003467-64.
This article has supplementary material available from openres.ersjournals.com. Qualified researchers can request access to anonymized individual patient-level data from AstraZeneca group of companies sponsored clinical trials via the request portal. All request will be evaluated as per the AZ disclosure commitment: https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.
Conflict of interest: T. Harrison reports non-financial support from AstraZeneca for assistance with manuscript writing during the conduct of the study; grants, personal fees for advisory boards and speaker meetings, and support to attend conferences from AstraZeneca, fees for advisory boards and speaker meetings from GSK, and personal fees from Vectura, outside the submitted work.
Conflict of interest: I.D. Pavord reports speaker fees, advisory board honoraria, sponsorship to attend scientific meetings and payments for organising educational events from AstraZeneca; speaker fees, advisory board honoraria and sponsorship to attend scientific meetings from Boehringer Ingelheim; a speaker fee from Aerocrine; speaker fees and advisory board honoraria from Almirall and Novartis; speaker fees, advisory board honoraria and sponsorship to attend scientific meetings from GlaxoSmithKline; advisory board honoraria from Genentech and Regeneron; speaker honoraria, payments for organising educational events and sponsorship to attend scientific meetings from Teva; speaker honoraria from Chiesi; advisory board honoraria from Sanofi, Circassia and Knopp; and funding from NIHR as a Senior Investigator, all outside the submitted work.
Conflict of interest: J.D. Chalmers reports grants and personal fees from AstraZeneca during the conduct of the study; and grants and personal fees from GlaxoSmithKline, Boehringer Ingelheim, Zambon, Insmed, Grifols and Novartis, grants from Gilead, and personal fees from Napp, all outside the submitted work.
Conflict of interest: G. Whelan is an employee of AstraZeneca.
Conflict of interest: M. Fagerås is an employee of AstraZeneca.
Conflict of interest: A. Rutgersson is an employee of AstraZeneca.
Conflict of interest: L. Belton reports other from AstraZeneca, during the conduct of the study; other from AstraZeneca, outside the submitted work.
Conflict of interest: S. Siddiqui has nothing to disclose.
Conflict of interest: P. Gustafson is an AstraZeneca employee and shareholder.
Support statement: The STIFLE study is funded by AstraZeneca. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received November 28, 2019.
- Accepted March 24, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References











Jump To
- Article
- Abstract
- Abstract
- Introduction and study rationale
- Hypothesis of the STIFLE study: use of anti-inflammatory reliever therapy in the “window of opportunity”
- Design of the STIFLE study
- A short review: FENO
- How will the STIFLE study help understand the day-to-day relationship between airway inflammation, symptoms and lung function in patients with asthma?
- Conclusion
- Supplementary material
- Acknowledgements
- Footnotes
- References
- Figures & Data
- Info & Metrics