





Abstract
Aims Brain magnetic resonance imaging (MRI) is recommended during the initial work-up for nonsmall cell lung cancer (NSCLC). Although small enhancing brain nodules not radiologically confirmed as metastatic lesions have often been detected, their clinical course has not been well studied.
Methods This nested case–control study included NSCLC patients who had small enhancing brain nodules detected by serial brain MRIs from January 2014 through December 2018 at a tertiary university hospital. Small enhancing brain nodules were defined as round enhancing nodules of ≤10 mm diameter without oedema in thin-section (1 mm) contrast MRIs. The incidence, natural course and risk factors of growing nodules were evaluated.
Results A total of 171 small enhancing brain nodules in 123 patients were observed over an average of 22.1 months. The incidence of nodule growth was 49.1% with mean growth rate of 11 mm·year−1. We found that 25.0% of the growing nodules contributed to clinical upstaging compared to the initial stage. Cerebral events were more common in growing nodules; therefore, local therapy was performed more often. However, there was no difference in the cerebral event-related mortality. Nodule growth was more frequent in younger individuals, multiple nodules, advanced disease, poorly differentiated carcinoma, rim enhancement and larger initial size. In multivariable analysis, predictors of growth were N stage ≥1, existence of epidermal growth factor receptor mutation and larger initial size.
Conclusion Considering the clinical course of small enhancing brain nodules, more intensive evaluation is required for early detection and pre-emptive intervention when accompanied by risk factors.
Abstract
Small enhancing brain nodules are found in 4.1% of NSCLC. Growth is found in the 49.1% with a rate of 11.0 mm per year. Lymph node metastasis, EGFR mutation and larger diameter are risk factors for growth. https://bit.ly/2ALqhhM
Introduction
Metastatic lesions are found at the time of diagnosis in about 30–40% of patients with nonsmall cell lung cancer (NSCLC) [1, 2]. About 10–20% of NSCLC patients have at least one brain metastasis at the time of diagnosis [3–5]. Metastatic brain lesion significantly increases morbidity and mortality in NSCLC [6, 7]. NSCLC patients in whom brain metastasis was detected at the time of initial diagnosis had worse survival rates than those in whom it developed later [8]. Therefore, brain magnetic resonance imaging (MRI) has been an important tool for initial diagnosis of brain metastasis in NSCLC patients [9–11].
The indication of brain MRI has been extended from patients with advanced stage or neurological symptoms to the early stage (IB) or asymptomatic patients. Silent brain metastasis has been identified in a large proportion of patients with NSCLC [12, 13]. Brain metastasis constitutes the majority of asymptomatic metastasis cases in stage I NSCLC [14]. Early detection of asymptomatic brain metastasis was related with reduced incidences of morbidity and mortality [15]. In general, the presence of neurological symptoms no longer determines the need for a brain MRI, except for stage IA NSCLC.
The increasing use of brain MRI scan for brain metastasis work-up has increased the detection of asymptomatic enhancing brain nodules. The radiological features of brain metastasis in MRIs have been well identified [16]. However, when the diameter of the enhancing brain nodule is too small, it is often difficult to radiologically distinguish malignant lesions from benign ones. In practice, instead of a brain biopsy, short-term follow-up with brain MRI is usually conducted for the undetermined brain nodules. Once a growth of the brain nodule is detected or a neurological symptom appears during the follow-up, radiation therapy or surgical intervention needs to be considered. Therefore, it is important to delineate the natural course of small enhancing brain nodules and identify risk factors for the growing nodules.
Methods
For structured and standardised reporting, we followed the statements from strengthening the reporting of observational studies in epidemiology guidelines [17].
Study design and eligibility criteria
We conducted a nested case–control study by reviewing the electronic medical records of pathologically diagnosed NSCLC patients from January 2014 through December 2018 at a tertiary teaching hospital in Korea. The inclusion criteria for the present study were as follows: 1) ≥18 years old; 2) absence of neurological symptoms; 3) small enhancing brain nodules detected in the initial thin-section (1 mm) brain MRI with contrast; and 4) implementation of serial brain MRIs to follow-up the small enhancing brain nodules for at least 3 months. We excluded patients who started any treatment likely to affect the size of the small enhancing brain nodules at initial presentation (i.e. a definite local therapy (surgical or radiation therapy) or a tyrosine kinase inhibitor therapy with the potential to penetrate the blood–brain barrier, such as afatinib, alectinib, brigatinib, crizotinib, dacomitinib, erlotinib, gefitinib, lorlatinib and osimertinib). If a patient had newly started one of those therapies in the middle of follow-up, we finished observation at the start of treatment and excluded the impact of the therapy on the growth rate of the initially observed nodule. Additionally, patients diagnosed with a primary brain tumour were excluded.
Clinical and radiological assessments
We evaluated clinical characteristics, including age, sex, history of smoking cigarettes (in pack-years), use of systemic chemotherapy, interval and frequency of brain MRIs during the observed period, total observed duration, and tumour–node–metastasis (TNM) stage. We assessed the histological features, including pathological diagnosis, epidermal growth factor receptor (EGFR) mutation, anaplastic lymphoma kinase (ALK) rearrangement and programmed death-ligand 1 (PD-L1) expression.
We analysed the radiological features, including the location, number of concurrent brain nodules, rim enhancement, initial size and interval size change. The interval of follow-up brain MRI was determined by each clinician. The small enhancing brain nodule was defined as an enhancing round nodule ≤10 mm diameter without oedema or haemorrhage. Brain nodules were primarily identified in formal brain MRI scan reports, and each MRI image was reviewed to identify small enhancing brain nodules. Also, the follow-up brain MRI images were reviewed to trace radiological changes in small enhancing brain nodules. These radiological features and interval size changes were determined after discussing with an experienced brain radiologist (IH). Based on the follow-up MRI results, the brain nodules were classified into those with growth and without growth. Growth was defined as a radiological evidence of increased diameter of the brain nodules in follow-up brain MRI. No growth was defined as no radiological evidence of increased diameter of the brain nodules in follow-up brain MRI at 6 months or more. Baseline characteristics and clinical and radiological features were compared between brain nodules with growth and without growth to find risk factors that were significantly related with growth of the brain nodule.
Our primary end-point was to analyse the incidence rate of growing nodules among the small enhancing brain nodules. The small enhancing brain nodules were observed until death or initiation of any treatment affecting the growth rate. To reveal the natural course of growing nodules, we evaluated interval change of the diameter (mm, mm·year−1), the event of newly developed neurological symptom or sign, the event of definite local therapy (surgical resection, stereotactic radiosurgery or whole-brain radiotherapy) for the newly developed neurological symptom or sign, and the event of central nervous system (CNS)-related death or all-cause death. We estimated the actual impact of growing brain nodules on clinical decisions by identifying events of clinical upstaging or treatment plan change, such as local to systemic therapy or curative to palliative therapy, via review of medical records. Subgroup analysis was performed to know how growth rate or growth risk was different according to significant radiological features.
Brain MRI protocol
Brain MRI scans were performed using a 3T magnetic resonance scanner (Ingenia, Philips Healthcare, Best, the Netherlands) with a 32-channel head coil. In addition to routine pre-contrast brain magnetic resonance sequences, thin-section post-contrast images were obtained after intravenously administering gadobutrol (Gadovist; Bayer Schering Pharma, Berlin, Germany) at a dose of 0.1 mmol·kg−1 of body weight. The post-contrast study included sagittal T1-weighted three-dimensional gradient-echo sequence (repetition time (TR) of 8.5 ms; echo time (TE) of 4.6 ms; flip angle (FA) of 8°; field of view (FOV) of 240×240 mm; matrix of 240×240; one excitation; and slice thickness of 1 mm). In addition, sagittal T1-weighted three-dimensional turbo spin-echo sequence with motion-sensitised driven-equilibrium preparation (TR of 500 ms; TE of 28.9 ms; FA of 90°; FOV of 240×240 mm; matrix of 240×240; one excitation; and slice thickness of 1 mm) was obtained for better detection of tiny enhancing nodules by selective suppression of blood vessel signals [18].
Statistical analyses
Comparative analyses of categorical variables were performed using Pearson's Chi-squared test or Fisher's exact test. Continuous variables were analysed using the t-test and median and interquartile range (IQR) or mean and sd were calculated. The time to growth of the small enhancing brain nodule was analysed using Cox proportional hazard regression model. After examining multicollinearity, multivariable analyses were performed using variables related to the growth of small enhancing brain nodules. Missing data on molecular testing were handled by excluding the patients in our analysis and addressed in the footnotes of each table. All statistical analyses were done using R statistical software, version 3.5.1 (R Core Team, 2018, Vienna, Austria).
Ethics
The Institutional Review Board Committee of Seoul National University Hospital approved the study protocol and waived the need for obtaining informed consents to access the electronic medical records (no. H-1901-154-1006).
Results
Among a total of 2998 patients with NSCLC who were evaluated using brain MRI, 540 patients were followed-up for brain lesions using serial brain MRIs starting from the time of initial diagnosis of NSCLC. There were 123 patients with 171 small enhancing brain nodules that met our eligibility criteria. Mean follow-up duration for the small enhancing brain nodules was 22.1±17.5) months. During the follow-up period, the estimated incidence rate of the growing small enhancing brain nodule was 84 out of 171 (49.1%) (figure 1).
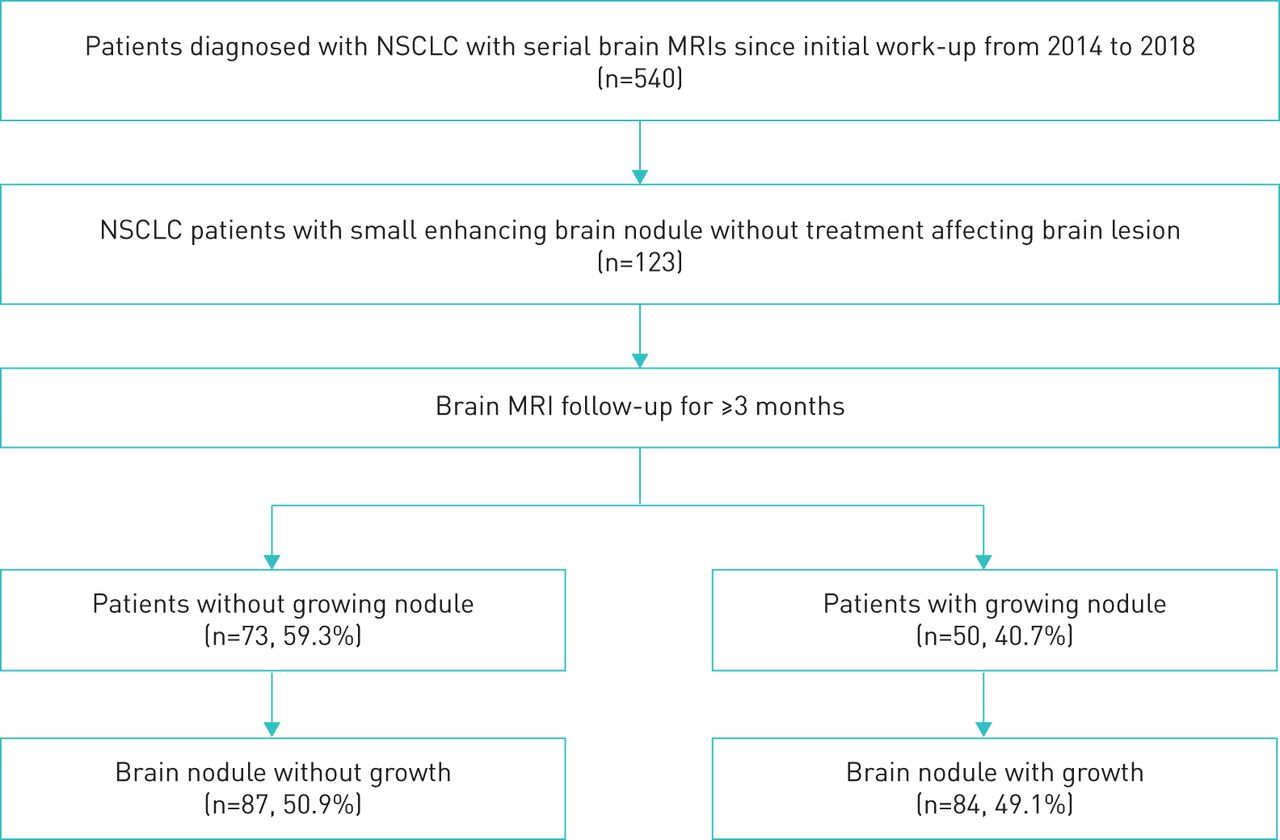
Flow chart of inclusion criteria for eligible small enhancing brain nodules. NSCLC: nonsmall cell lung cancer; MRI: magnetic resonance imaging.
Baseline characteristics of small enhancing brain nodules
The baseline characteristics of the study population are summarised in table 1. The mean patient age was 62.7±11.1) years and 114 out of 171 (66.67%) small enhancing brain nodules were detected in males. During regular follow-up brain MRI scans, the small enhancing brain nodule was found growing in 50 out of 123 (40.7%) patients. Among patients with and without evidence of a growing brain nodule, the former were more likely to be younger and to have received more systemic chemotherapy whereas a solitary lesion was more likely to be found in the latter group of patients. There were no significant differences in sex, smoking history or total observed duration between these two groups. Also, multiple lesions (≥3) were significantly related with brain nodule growth.
Baseline characteristics of NSCLC patients with small enhancing brain nodules
Clinical and radiological manifestations of small enhancing brain nodules
We examined the difference in TNM staging between patients with and without growing small enhancing brain nodules (table 1). The T stage was not related with the growth of brain nodules, nor did the N stage affect their growth. Lymph node involvement was significantly associated with a higher detection rate of brain nodule growth. The small enhancing brain nodules were more likely to be stable in case of extracranial TNM stage I and II, but grew in extracranial metastatic lesions (TNM stage IV). Also, we evaluated whether the histological features of NSCLC were related to the growth of small enhancing brain nodules (table 2). Adenocarcinoma was the most common histological type (62.6%) among the various pathologic features of NSCLC. There was no difference in the proportion of adenocarcinoma, squamous carcinoma and large-cell carcinoma between small enhancing brain nodules with and without growth. EGFR mutation, ALK rearrangement and PD-L1 expression were not significantly associated with brain nodule growth detection.
Comparison of histological features between the small enhancing brain nodules with and without growth
Radiological features of small enhancing brain nodules are described in table 3. There was no differences in geographical distribution throughout the brain according to the growth of the brain nodules. Growing brain nodules had a greater diameter at initial presentation (4.0 mm versus 2.5 mm, p<0.001) and the nodules with rim enhancement were more likely to be growing (p<0.001). Although the MRI interval was similar, MRI scans were conducted less often in patients with a brain nodule with growth.
Comparison of radiological features between the small enhancing brain nodules with and without growth
Natural history of small enhancing brain nodules with growth
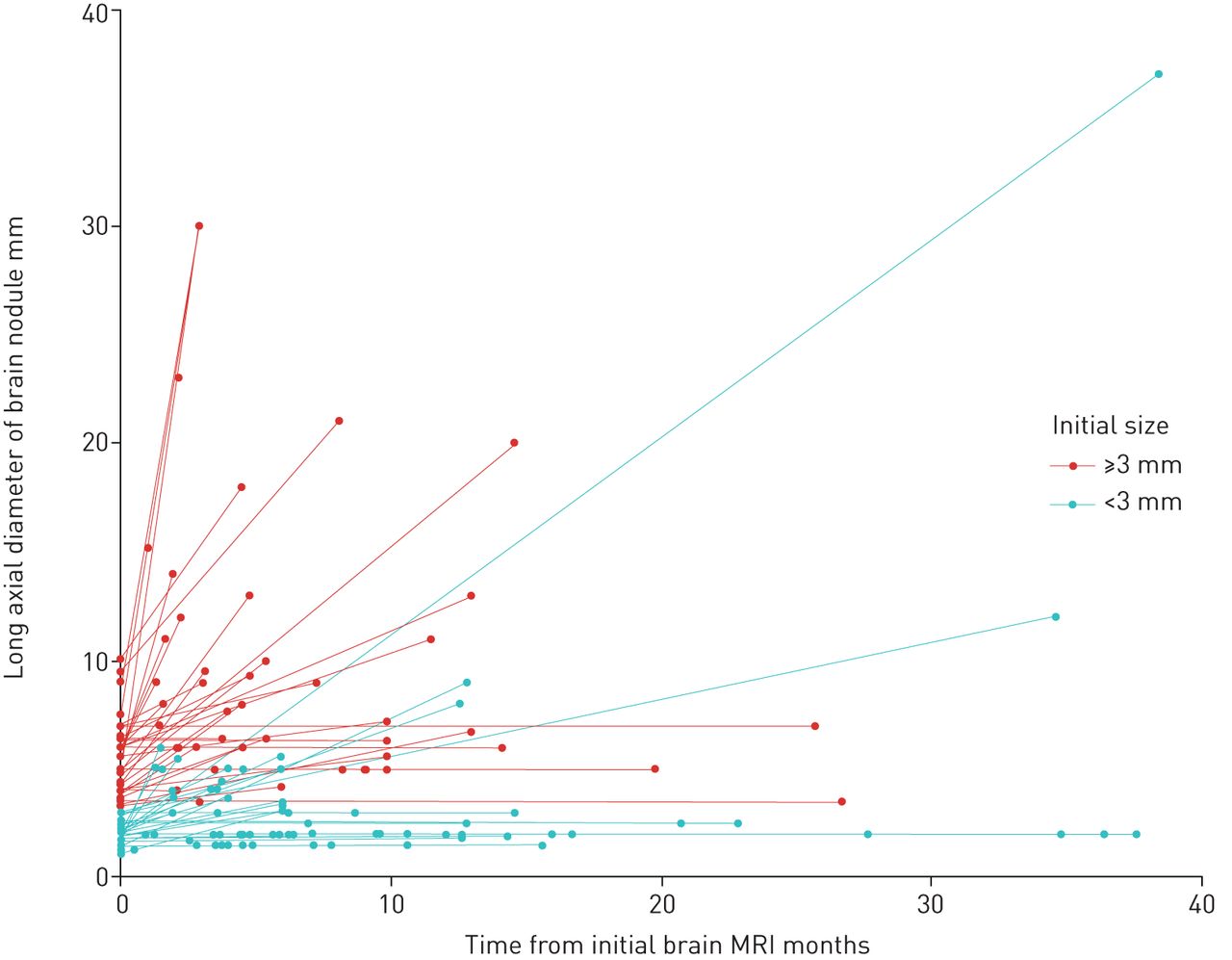
In growing small enhancing brain nodules (n=84), median change of diameter was 3.2 mm (IQR, 2.0–7.8) and annual median growth rate was 11.0 mm·year−1 (IQR, 4.9–20.7; table 4 and figure 2). We found that 25% of the growing brain nodules contributed to clinical upstaging of NSCLC. In about 35% of the growing brain nodules, the chemotherapy regimen was changed immediately after the detection of brain nodule growth. More CNS-related events and definite local therapy were observed in small enhancing brain nodules with growth (p=0.001 and p=0.003, respectively). For the patients with definite local therapy, the protocolised radiation doses of 20 Gy in 5 fractions or 30 Gy in 10 fractions were applied for whole-brain radiotherapy and the median peripheral dose of 22 Gy (range, 15–25 Gy) was prescribed at the median 50% isodose line for Gamma Knife radiosurgery (Leksell Gamma Knife® Icon™). Brain nodules with growth were significantly associated with a higher overall mortality rate when compared with those without growth (p=0.001). However, the relationship between growth of small enhancing brain nodules and CNS-related mortality was not significant (p=0.638).
Natural course of the small enhancing brain nodule over the period of follow-up

{kind=link}
{kind=link}
Natural course of small enhancing brain nodules. Green line indicates the small enhancing brain nodules with initial diameter of <3 mm and red line indicates the small enhancing brain nodules with initial diameter of ≥3 mm. GGN: ground-glass nodule.
In subgroup analyses, the small enhancing brain nodules with rim enhancement showed a higher growth rate (17.7 mm·year−1 versus 5.6 mm·year−1, p<0.001) (supplementary information 1). In addition, we found a higher risk of growth in brain nodules with a diameter ≥3 mm, especially when observed for 6 months or longer (supplementary information 2 and 3).
Analysis of risk factors related to the growth of small enhancing brain nodule
In univariable analysis using Cox regression hazard model, we found that N stage ≥1, extracranial metastasis, EGFR mutation, PD-L1 expression >10%, number of brain nodules, rim enhancement and initial size were significantly related with growth of small enhancing brain nodules upon observed time (table 5). In multivariable analysis, N stage ≥1, existence of EGFR mutation and a larger initial size were significantly associated with a higher risk of growth of small enhancing brain nodules upon observed time.
Evaluation of risk factors for the growth of the small enhancing brain nodules using Cox regression hazard model
Discussion
This is a large cohort of very small brain nodules not deemed to be metastases at baseline work-up of newly diagnosed lung cancer. Predictors we found in patients with nodules showing growth during follow-up were also features of a more aggressive phenotype such as younger age, a histology of poorly differentiated carcinoma, higher extracranial TNM stage, multiple brain nodules and more systemic chemotherapy. Regular brain MRIs with at least 6-month intervals were considered adequate in that the cumulative growth rate of the growing small enhancing brain nodules was 11.0 mm·year−1 in diameter. The growth has a clinical significance because about 25% of these nodules contributed to clinical upstaging and about 35% of them contributed to change of chemotherapy regimen in our study. Closer follow-up with frequent brain MRI scans or pre-emptive therapy might be needed in NSCLC patients with any lymph node metastasis, EGFR mutation or a larger diameter (≥3 mm) of the brain nodule, given the increased hazard ratio of growth upon observed time among the small enhancing brain nodules in these patients.
Brain MRI scan has played an important role in the initial work-up for staging of NSCLC. A previous study reported that 22.4% of brain metastases were present in the initial brain MRI [19]. Initial brain MRIs detected metastatic lesions in about 5% of the patients with squamous cell carcinoma and in about 16% of those with adenocarcinoma [20, 21]. An important point in our study is that in about 4% of the NSCLC patients, additional small enhancing nodules were detected that were insufficient to make a definite diagnosis of a metastatic lesion. About half of the small enhancing brain nodules were eventually found growing during the 22-month follow-up period. When brain MRI was repeated every 5.5 months, about 94% of the growth of brain nodule could be detected within 12 months. Our study provides a perspective for future studies regarding follow-up strategies in NSCLC patients when a small enhancing brain nodule is found.
Another important finding of our study was that the growing small enhancing brain nodules derived more CNS-related events but did not increase CNS-related mortality. This finding may be explained by a higher rate of definite local therapy in this group which prevents the progression of the metastatic lesion. In fact, a higher overall mortality rate in patients with growing small enhancing brain nodules was likely not caused by the brain lesion itself, but may be attributable to their advanced TNM stage. In current practices with short-term brain MRI follow-up and definite local therapy for a growing brain nodule, detection of small enhancing brain nodules seems to have limited impact on patient's prognosis. However, a shorter follow-up interval can be beneficial because an earlier intervention in high-risk patients may be likely to reduce CNS-related symptoms [22].
We found that the growth rate of small enhancing brain nodules was significantly associated with their initial size and rim enhancement. The initial diameter of the nodules not only predicted the growth, but also the magnitude of growth (i.e. a larger diameter was associated with a greater growth rate, whereas rim enhancement did not show significant power in the multivariable analysis to predict the growth of small enhancing brain nodules). In fact, brain metastasis accounts for only 30% of the radiologically rim-enhancing lesions [23]. Furthermore, our study showed that the growth rate is greater with rim enhancement in growing small enhancing brain nodules. Therefore, it would be more reasonable to differentiate the brain MRI follow-up interval for small enhancing brain nodules according to the diameter and rim enhancement in the initial brain MRI.
Our study has several limitations. First, we excluded enhancing brain lesions that were diagnosed and treated as definite brain metastases at the initial work-up for NSCLC staging. The natural course of the growing small enhancing brain nodules included in our study cannot be applied to all the metastatic brain lesions in NSCLC, because it would be less aggressive. Second, brain biopsy was not conducted for any patient to diagnose brain metastasis at initial work-up. Growth is not synonymous with metastasis. It is possible to incidentally find growing enhancing brain nodules in primary brain tumours or infections [24]. However, given the clinical context that brain MRI was performed for staging work-up of NSCLC, most growths were likely to suggest metastasis. For small enhancing brain nodules that did not grow, it is difficult to make the final diagnosis as one disease entity. Vascular enhancement and capillary telangiectasia are commonly considered as a radiological diagnosis in these cases. Stable or slowly growing metastatic lesions may also be included in no growth group without detectable growth during our study period. However, stable or slowly growing metastasis is considered as a very rare case and does not demonstrate clinical significance. A long-term follow-up for slowly growing metastasis may be needed, as the life expectancy of NSCLC patients has improved. Third, the frequency of follow-up brain MRI was lower in small enhancing brain nodules with growth during the observed period. When the growth of brain nodule was identified, the observed duration was censored because the treatment for the brain lesion was initiated immediately. In fact, the growing brain nodule had a shorter observation period of about 3.4 months. However, there was no difference in brain MRI intervals between patients having brain nodules with and without growth groups. The physician's practice appears similar among the patients with small enhancing brain nodules.
Conclusions
A closer observation is required to detect small enhancing brain nodule during initial work-up for NSCLC staging in cases with advanced stage tumour, EGFR mutation, and initial nodule size ≥3 mm. This may lead to earlier detection of brain metastasis and pre-emptive intervention. Further research is needed to reach a consensus on the interval and duration of performing brain MRIs in NSCLC patients with small enhancing brain nodules.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Growth rates of small enhancing brain nodules according to initial diameter and rim enhancement 00109-2020.Figure_Scatter_Rim_enhancement
Forest plot of hazard ratios for the growth of brain nodules according to the initial diameter 00109.2020.Figure_ForestPlot
Detection rates of growing small enhancing brain nodules with the initial diameter of less than 3 mm and greater than or equal to 3 m 00109-2020.Table_Incidence_growth
Footnotes
This article has supplementary material available from openres.ersjournals.com
Conflict of interest: H.W. Lee has nothing to disclose.
Conflict of interest: J. Cho has nothing to disclose.
Conflict of interest: N. Kwak has nothing to disclose.
Conflict of interest: I. Hwang has nothing to disclose.
Conflict of interest: Y.S. Park has nothing to disclose.
Conflict of interest: C-H. Lee has nothing to disclose.
Conflict of interest: S-M. Lee has nothing to disclose.
Conflict of interest: C-G. Yoo has nothing to disclose.
Conflict of interest: Y.W. Kim has nothing to disclose.
Conflict of interest: S.M. Choi has nothing to disclose.
- Received February 29, 2020.
- Accepted June 4, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










