





Abstract
Focal bronchial dilatations develop after bronchial thermoplasty (BT) in 58% of patients with severe asthma. This suggests a need for systematic evaluation by CT scan after BT, with specific focus on bronchial dilatation development. https://bit.ly/2AYuhMj
To the Editor:
Bronchial thermoplasty (BT) is a non-pharmacological alternative treatment for severe asthma [1, 2]. BT consists of applying radiofrequency energy to the airways that are distal to the lobar bronchi and >3 mm, to reduce airway smooth muscle mass and bronchial hyperreactivity. However, concerns have been raised about long-term safety, especially risk of bronchial stenosis or bronchiectasis. Indeed, morphological changes in bronchial tubes, such as bronchiectasis or widening of the airways, have been occasionally described during follow-up [3–7]. However, bronchial changes have not been systematically assessed by computed tomography (CT), especially in large prospective cohorts [2, 3, 8, 9].
In this retrospective observational study, we included patients with severe asthma who underwent BT (three procedures, every 3 weeks) in our centre between January 2013 and December 2017 and who had at least one chest CT scan before BT and, at the earliest, 4 months after the last procedure. Pre-BT CT scan, the first post-BT CT scan taken at least 4 months after the procedure and the last available CT scan were visually analysed and compared by three operators, including a specialised radiologist, who were blinded to the clinical response. Analysis focused on the first appearance of new bronchial dilatations after BT, and their location, shape and evolution on successive CT scans.
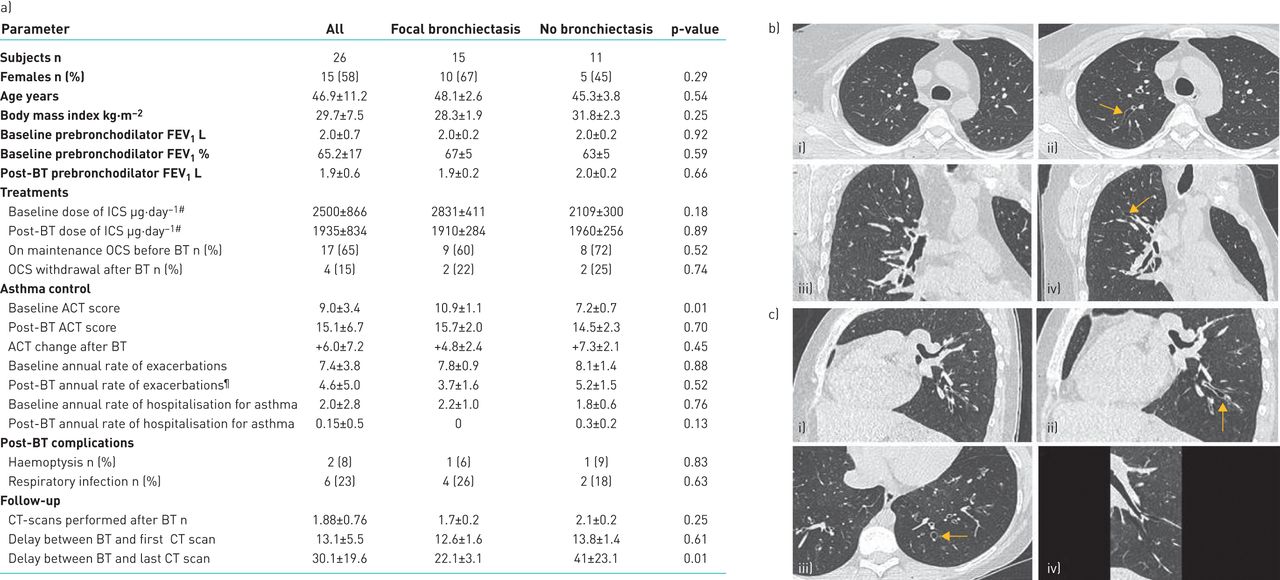
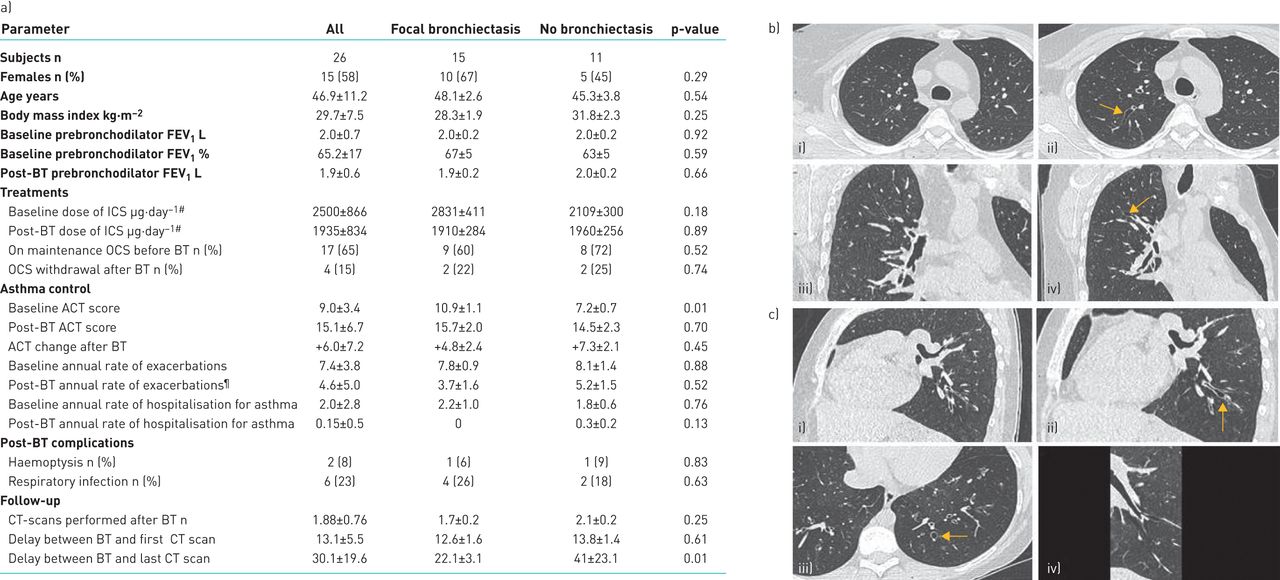
We identified 26 asthmatic patients who fulfilled the inclusion criteria. Clinical characteristics are summarised in figure 1a. Mean±sd age was 47±11 years. 15 (58%) patients were female and 12 (46%) were ex- or current smokers. Mean±sd FEV1 before BT was 65%±17%. Mean±sd follow-up after BT was 30.1±19.6 months (range 6–72 months).
{kind=link}
a) Patient characteristics. Comparison of baseline and 12-month post-bronchial thermoplasty (BT) parameters between patients with or without the appearance of new bronchial dilatations (bronchiectasis). Data are presented as mean±sd, unless otherwise stated. FEV1: forced expiratory volume in 1 s; ICS: inhaled corticosteroids; OCS: oral corticosteroids; ACT: asthma control test; CT: computed tomography. #: beclomethasone equivalents; ¶: during the first year after BT. b) i) and iii) Axial and coronal planes of CT before BT. ii) and iv) Axial and coronal planes of CT of the same patient 2 years after BT, showing a fusiform bronchial dilatation (arrows). c) i) Coronal plane of CT before BT. ii) and iii) Coronal and axial planes of CT of the same patient 3 years after BT, showing a sacciform bronchial dilatation (arrow). iv) CT reconstruction showing the focal bronchial dilatation.
Before BT, four (15%) patients had mild diffuse bronchiectasis, four (15%) had cylindrical bronchiectasis only located in the middle lobe, and diffuse bronchial thickening was observed in 16 (61%). After BT, one or more new focal bronchial dilatations was detected on CT in 15 (58%) patients, with a mean±sd number of 4.0±2.7 dilatations per patient. Most dilatations were tubular, with an unusual fusiform shape, and 1–2 cm in length (figure 1b), a few were shorter with a round shape (figure 1c). Bronchial dilatations were detected on the first post-BT CT scan (performed at a mean±sd of 16±9 months post-BT (range 4–41 months)) in 13 out of 15 patients and on the second CT scan in the remaining two patients. 17 patients (65%) had more than one CT scan after BT during their follow-up; nine had new focal bronchial dilatations diagnosed. In this sub-group, neither the number nor the size (diameter and length) of focal abnormalities changed over a mean±sd follow-up of 41±21 months (range 15–69 months). For patients without new focal bronchial dilatations, the mean CT scan follow-up was 41±23 months (range 11–72 months).
Bronchial dilatations were located in fourth- to fifth-order bronchi, in the left lower lobe in 40% of cases, right upper lobe in 30% and right lower lobe in 25%. The mean diameter was 4.5± 0.9 mm. The 15 patients with new dilatations after BT did not differ from their counterparts in terms of baseline characteristics (figure 1a). The oral cortico-sparing effect, reduction in exacerbations and hospitalisations and increase in Asthma Control Test scores at 12 months after BT were similar between the two groups (figure 1a). The number of activations during the procedure was equivalent. We did not find any correlation between the number of activations in a lobe and number of focal bronchial dilatations.
Bronchial changes after BT have been poorly explored. In the AIR2 trial [5], only 93 of the 190 patients had a CT scan after the procedure. Bronchial dilatations were observed in 3% [5]. Other smaller studies reported bronchial dilatations in 8% [7] and 15% [4] of patients, which is much lower than that observed in the present study (58%). The focal bronchial dilatations such as we describe, some being subtle, may have been missed without careful examination in previous studies.
Mild diffuse bronchiectasis is observed in 25% to 67.5% of patients with severe asthma [10]. These cases differ from the focal fusiform dilatations we observed, whose aspect has never been described in asthma. These changes can be detected as soon as 4 months after the last procedure and were never observed in the untreated middle lobe and always occurred in fourth- to fifth-order bronchi. No bronchial stenosis was observed, although it was not quantitatively assessed [6]. These observations suggest a limited, local, thermal energy-induced tissular damage, such as that discussed with the development of early peribronchial consolidations [4], rather than a fibrotic wound healing. BT-induced structural changes, such as focal destruction of airway smooth muscle, replaced by loose connective tissue, or bronchial nerve ending damage, as previously described [9], may contribute to reduced bronchial tone and global increase in airway diameter.
Focal dilatations occurred in more than half of our patients after BT but did not modify the clinical response, which is comparable to previously reported series. They were not associated with an increased rate of side-effects, such as infections or haemoptysis, over a 12-month clinical follow-up, or with poorer lung function. Two cases (7%) of haemoptysis were reported after BT, one in each group (new dilatations and no new dilatations) occurring in the early post-procedure phase, and were not related to bronchial dilatations.
This study has some limitations due to its retrospective design, the relatively small number of patients and different follow-up among patients, which does allow for proper evaluation of BT safety. We are confident that these focal dilatations are related to the procedure and not to the natural history of airway changes in severe asthma. Indeed, some other investigators in France have also observed such changes at the same delay after the procedure (N. Guibert and L. Guilleminault, CHU de Toulouse, and C. Fournier, CHRU de Lille; personal communication). A control group of patients without BT would have not been matched in terms of airway inflammatory pattern, a strong determinant for airway remodelling, because BT was mostly performed in our centre in patients not eligible for biological agents during the study period. Given the observations reported here, this indication is still current in our hospital, in accordance with recommendations from French health authorities. Special attention is given to diffuse bronchiectasis, which when diffuse and even mild contraindicates the procedure.
Although we did not find any correlation between airway changes and number of activations, our findings argue for BT protocol optimisation, as was already suggested to improve treatment efficiency [11]. Whether limiting the number of treated lobes may reduce the incidence of bronchial dilatations while maintaining equivalent efficacy, although hypothetical, could be investigated. Indeed, although we did not identify clinical complications related to bronchial dilatations, we cannot exclude the possibility of longer-term complications or a significant rate of complications in a larger effective sample. We suggest that systematic evaluation by CT scan should be performed after BT, with specific focus on the development of bronchial dilatations.
Acknowledgements
We thank Clément Fournier (CHRU de Lille, Lille, France), Laurent Guilleminault and Nicolas Guibert (CHU de Toulouse, Toulouse, France) for helpful discussions and sharing experience, and Laura Smales (BioMedEditing, Toronto, Canada) for help with English editing.
Footnotes
Conflict of interest: C. Thibaut de Ménonville has nothing to disclose.
Conflict of interest: M-P. Debray reports personal fees from PneumRx (Boston scientific), personal fees and nonfinancial support from Boehringer Ingelheim, and nonfinancial support from Roche, outside the submitted work.
Conflict of interest: L. Alavoine has nothing to disclose.
Conflict of interest: M-C. Dombret has nothing to disclose.
Conflict of interest: A. Khalil has nothing to disclose.
Conflict of interest: P-Y. Brillet has nothing to disclose.
Conflict of interest: M. Aubier reports grants from GSK, AstraZeneca and Boston Scientific, and grants and personal fees from Chiesi, outside the submitted work.
Conflict of interest: C. Taillé reports personal fees from and that she was a study investigator for AstraZeneca; personal fees from and that she was a study investigator for Boehringer; personal fees from Chiesi; grants and personal fees from, and that she was a study investigator for GSK; personal fees from and that she was a study investigator for Novartis; personal fees from Teva; and that she was a study investigator for Sanofi, all outside the submitted work.
- Received March 4, 2020.
- Accepted July 7, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










