





Figures
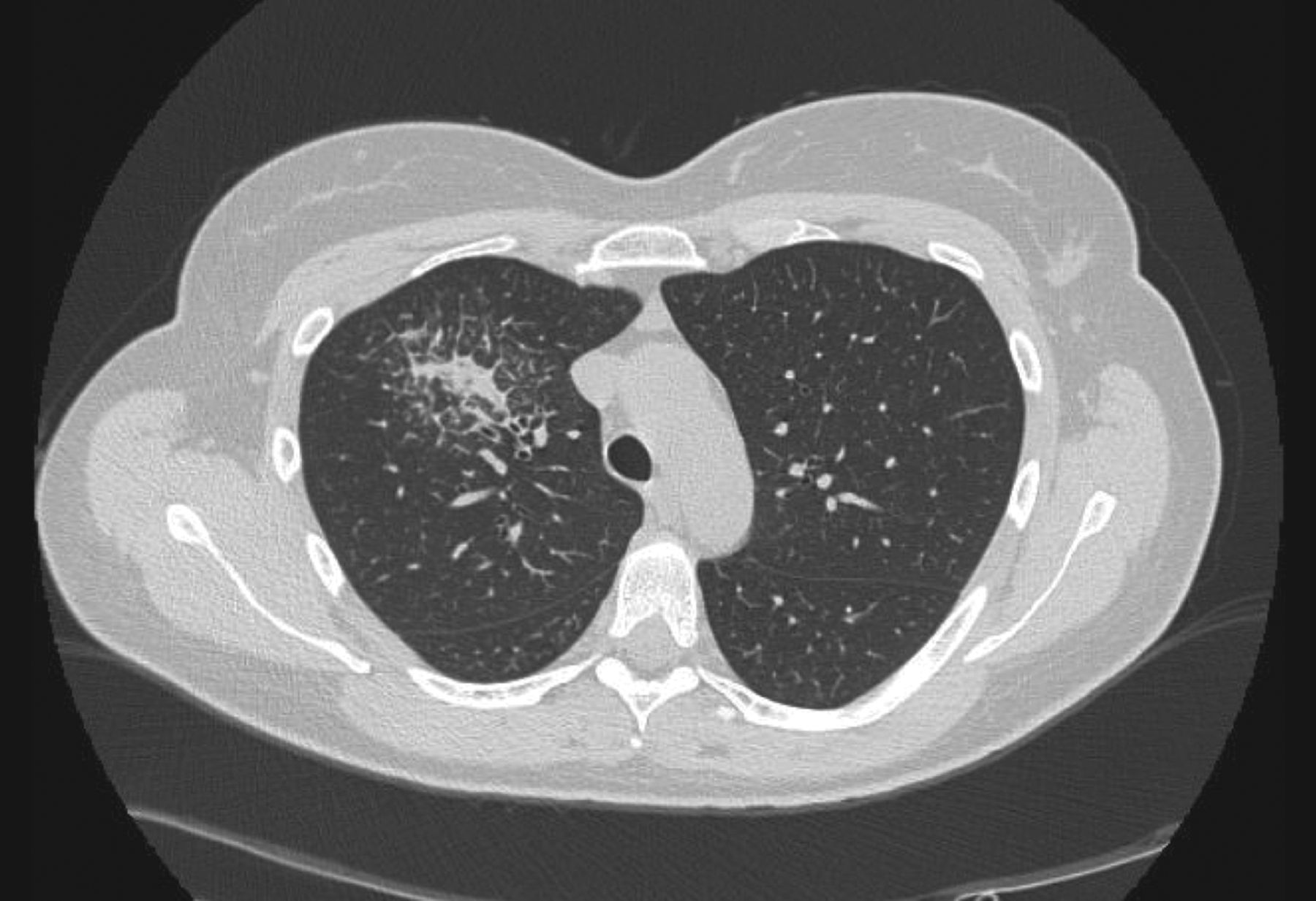
- FIGURE 1
Computed tomography scan of case no. 1: consolidation area in the upper right lobe, with a partial component of ground glass and surrounding thickening of intra and interlobular septa.
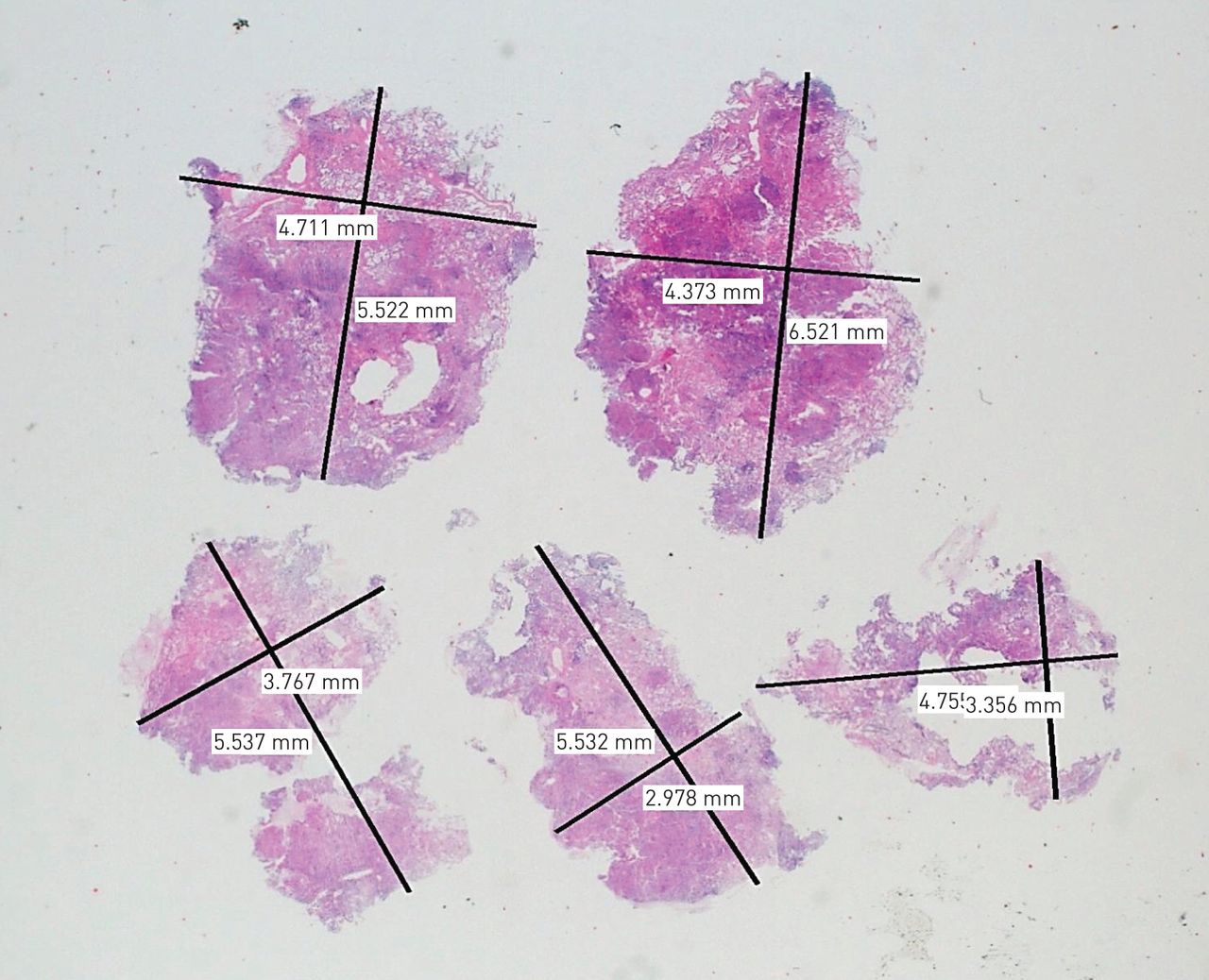
- FIGURE 2
Haematoxylin & eosin ×20: low magnification of case no. 2, showing the number of samples and their size.
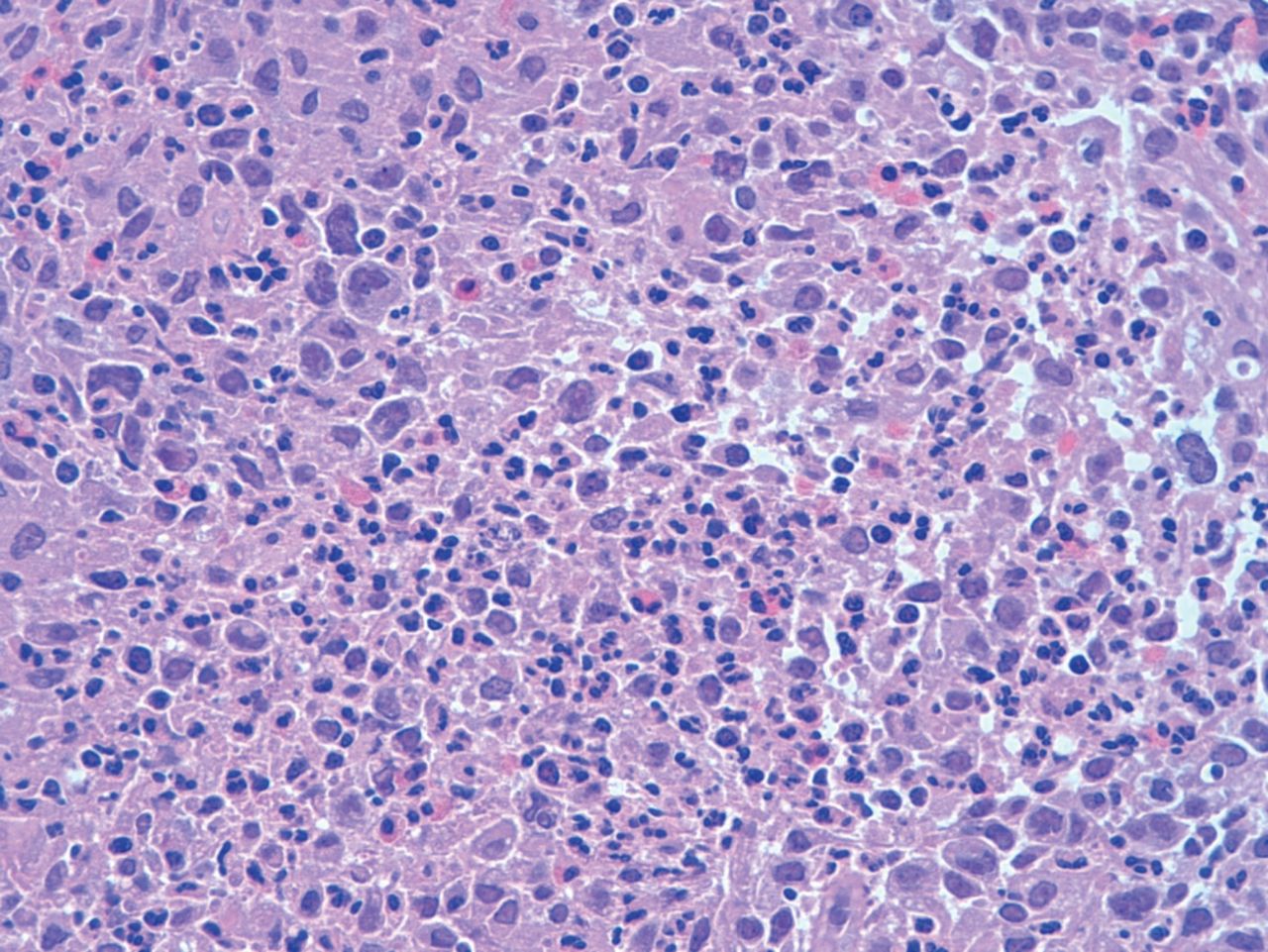
- FIGURE 3
Haematoxylin & eosin ×100: case no. 7. A diffuse and mixed infiltration is present, with eosinophils, lymphocytes and large blastic elements, consistent with Hodgkin cells.
- FIGURE 4
Immunohistochemical stain for CD30 (left) and CD15 (right), ×200: case no. 7. The large elements are strongly positive both for CD30 and CD15, confirming the diagnosis of classic Hodgkin lymphoma.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Clinical and radiological findings
Case no.,
sex, age yrsRecent symptoms and suspected diagnosis Laboratory findings and functional pulmonary data BAL HRCT 1, female, 38 Former smoker. Dry cough and light fever. No relevant auscultatory sounds.
Suspect for lymphoproliferative disorder.SaO2 99%.
FVC 102%
FEV1 99%
DLCO 49%Total cellularity: 630×106·L−1, N 0%, E 3.0%, L 77.0%, M 20.0% Nodular opacities at superior lobe of right lung; multiple bilateral perilymphatic nodules, with ground-glass areas and thickening of septa. 2, female, 41 Nonsmoker; housewife; multiple sclerosis.
Precedent diagnosis of T lymphoma-EBV-related, treated with a complete response.
Light fever and dyspnoea. Presence of nodular skin lesions in lower limbs.Lymphopenia (total lymphocytes: 0.42 109).
FVC 100%
FEV1 100%
DLCO 52%Total cellularity: 270×106·L−1, N 4.0%, E 0.0%, L 26.0%, M 70.0% Bilateral lung opacities, predominantly perivascular, mostly at inferior lobes, with areas of consolidation. 3, male, 68 Respiratory insufficiency and pulmonary hypertension. Atrial fibrillation; dyslipidaemic; demyelinating polyneuropathy.
Light fever, asthenia, confused state.
Intravascular lymphoma? DAD? OP? other?CRP 169; LDH 975.
Monoclonal IgG λ component on protein electrophoresis.
FVC 89%
FEV1 91%
DLCO 53% (mild restrictive deficit)Total cellularity: 40×106·L−1, N 6.0%, E 0.0%, L 8.0%, M 86.0% Diffuse density increasing and minimal consolidations in dorsal regions, mostly at inferior lobes. Suspect for DAD or OP. 4, male, 57 Nonsmoker; teacher; hypertension; MGUS since 2002, restricted for IgM κ.
Tiredness, dyspnoea and light fever for 1 month. Splenomegaly.
Suspect for intravascular lymphoma? HP? Other?Pancytopenia; LDH 3194. Monoclonal IgG κ component on protein electrophoresis.
Pulmonary hypertension: PAP 40 mmHg. Negative hypersensitivity specific antigens.
FVC 107%
FEV1 109%
DLCO 42%Total cellularity: 210×106·L−1, N 2.0%, E 0.0%, L 8.0%, M 90.0% Ground glass with expiratory air trapping and mediastinal adenopathy.
Suspect for intrinsic allergic alveolitis.5, female, 70 Hashimoto thyroiditis and Sjögren syndrome. Light fever.
MALT lymphoma? other?No significant alterations.
FVC 81%
FEV1 81%
DLCO 59%Total cellularity: 210×106·L−1, N
3.0%, E 0.0%, L 30.0%, M 67.0%Parenchymal bilateral consolidations, with thickening of interstitial septa (those nodules were also PET-positive). 6, female, 63 Former smoker; housewife; hypertension; MGUS.
Fever, cough, arthralgias, light myopathy, Raynaud.
Suspect for anti-synthetase syndrome. OP? NSIP? other?Specific antibodies for polymyositis: ku ++, Ro-52 +++; high CPK and myoglobin.
PaO2: 82.9 mmHg, PaCO2: 42.5 mmHg, pH: 7.39 U.
Mild lymphopenia. Two monoclonal IgG components (one κ and one λ) on protein electrophoresis.
FVC 105%
FEV1 93%
DLCO 55%Total cellularity: 200×106·L−1,
N 18%, E 1%, L 22%, M 5%Interlobular reticular septal thickening and ground glass, honeycombing: suspect of fibrotic evolution of former interstitial pathologies. 7, female, 31 Nonsmoker; office worker. Former mononucleosis; asthma. Light fever, sweating, dry cough and pain at right shoulder. CRP 60.9 mg·
L−1; LDH 290.
FVC 101%
FEV1 91%
DLCO 78%Not available Opacity at superior right lobe on CT scans and diffuse bone, lung, splenic and lymph nodes uptakes on PET. 8, female, 74 Nonsmoker; hypertension. Productive cough and light fever. Monoclonal expression of IgG κ light chains on BAL.
FVC 100%
FEV1 85%
DLCO 88%Total cellularity: 510×106·L−1,
N 33.0%, E 2.0%, L 55.0%, M 10.0%Bilateral lung nodules, persistent after antibiotics therapy (with ground-glass areas and interstitial thickening). 9, female, 78 Previous diagnosis of diffuse large B-cell lymphoma and breast carcinoma.
Lung nodules and mediastinal adenopathy.Mild lymphopenia. LDH 316; CRP 67.3.
Monoclonal IgG κ component on protein electrophoresis.
FVC 101%
FEV1 102%
DLCO 76%Total cellularity: 90×106·L−1,
N 60.0%, E 0.0%, L 10.0%, M 30.0%Lung opacities and mediastinal, abdominal and groin lymphadenopathy on CT-PET. 10, male, 35 Back pain some months earlier; worsening after antibiotics.
Suspect for sarcoid versus MALT lymphoma.Anaemia.
LDH 112; CRP 73.4.
FVC 100%
FEV1 101%
DLCO 73%Total cellularity: 3720×106·L−1,
N 6.0%, E 0.0%, L 94.0%Hilar and para-hilar parenchymal opacities with mediastinal adenopathy. 11, male, 40 Nonsmoker; HIV+; positivity for Cryptococcus.
Thoracic pain, cough and fever; enlargement of axillary lymph nodes.
Suspect for lymphoma or cryptococcosis.Anaemia.
Peripheral blood: total CD3+ lymphocytes: 77%, with a CD4/CD8 ratio of 0.18.
Functional pulmonary data not availableTotal cellularity: 680×106·L−1,
N 25.0%, E 0.0%, L 50.0%, M 25.0%Multiple solid lung nodules, bilateral but predominant on the right. 12, male, 60 Former smoker; recent finding of lymphoplasmocytic lymphoma/Walderström on bone marrow biopsy. Weight loss and anaemia.
Suspect for lymphomatous lesion versus fungi versus lung cancer.Anaemia.
FVC 103%
FEV1 105%
DLCO 88%Total cellularity: 80×106·L−1,
N 3.0%, E 0.0%, L 17.0%, M 80.0%Bi-basal nodular areas, ground-glass areas, micronodular perilymphatic aspect, minimum pleuropericardic effusion. Splenomegaly. 13, female, 45 Nonsmoker. Went to ER for dry cough and thoracic pain; dyspnoea without fever.
Suspect for lymphoma.Anaemia.
RCP 15.
FVC 88%
FEV1 95%
DLCO 60%Total cellularity: 330×106·L−1,
N 3.0%, E 0.0%, L 35.0%, M 60.0%Opacities with ground-glass halo, mediastinal and subdiaphragmatic adenopathy, splenomegaly with multiple hypodense lesions. Lung function values are presented as % predicted. HRCT: high-resolution computed tomography; SaO2: oxygen saturation of arterial blood; FVC: forced vital capacity; FEV1: forced expiratory volume in 1 s; DLCO: diffusing capacity of the lung for carbon monoxide; N: neutrophils; E: eosinophils; L: lymphocytes; M: macrophages; EBV: Epstein–Barr virus; CRP: C-reactive protein; LDH: lactate dehydrogenase; MGUS: monoclonal gammopathy of unknown significance; HP: hypersensitivity pneumonia; PAP: pulmonary arterial pressure; MALT: mucosa-associated lymphoid tissue; DAD: diffuse alveolar damage; OP: organising pneumonia; NSIP: nonspecific interstitial pneumonia; CPK: creatine phosphokinase; PaO2: partial pressure of oxygen in arterial blood; PaCO2: partial pressure of carbon dioxide in arterial blood; CT: computed tomography; PET: positron emission tomography; BAL: bronchoalveolar lavage; ER: emergency room.
- TABLE 2
Histological features
Case no. No. specimens Not adequate Total size Distribution Histological diagnosis 1 5 – 40.60 mm2 Small lymphoid cells around blood vessels MALT lymphoma 2 5 – 107.82 mm2 Small lymphoid cells, with few blasts, around blood and lymphatic vessels and paraseptal zones PTCL, NOS 3 4 – 76.00 mm2 Large lymphoid elements in capillaries and arterioles intravascular NHL 4 2 – 98.92 mm2 Large lymphoid elements in capillaries intravascular NHL 5 2 – 47.56 mm2 Small lymphoid cells, with scattered large cells, around blood vessels. Colliquative necrosis. EBV+ LYG, type 2 6 4 – 81.01 mm2 Small lymphoid cells and plasma cells around blood vessel and along lymphatic routes (paraseptal and subpleural) MALT lymphoma 7 7 1: bronchial wall 73.20 mm2 Hodgkin cells and lymphoid infiltrate around bronchiolar walls and vessels HL 8 2 – 98.55 mm2 Small lymphoid cells around blood and lymphatic vessels (also paraseptal) MALT lymphoma 9 5 – 103.82 mm2 Large atypical lymphoid cells around bronchovascular bundles MALT lymphoma 10 4 – 78.92 mm2 Hodgkin cells and lymphoid infiltrate HL 11 13 – 417.70 mm2 Large atypical lymphoid cells around blood vessels. Coagulative necrosis Diffuse large B-cell lymphoma 12 9 2: fibrin 51.55 mm2 Small lymphoid cells around bronchovascular bundles and blood vessels Lymphoplasmocytic lymphoma 13 4 2: pleura and muscle 235.11 mm2 Dense infiltration of small lymphoid cells in subpleural area, resulted a mixture of B and T-lymphoid cells Cryo-TBB and VATS: atypical lymphoproliferative process MALT: mucosa-associated lymphoid tissue; PTCL, NOS: peripheral T-cell lymphoma, not otherwise specified; NHL: non-Hodgkin lymphoma; LYG: lymphomatoid granulomatosis; EBV: Epstein–Barr virus; HL: Hodgkin lymphoma; cryo-TBB: transbronchial cryobiopsy; VATS: video-assisted thoracoscopic surgery.










