





Abstract
The Greek experience reveals that harmonised collaboration among primary care, secondary facilities, designated hospitals and official authorities results in prompt and accurate management of the pandemic-related crisis of COVID-19 https://bit.ly/3eSHVhG
To the Editor:
The novel human coronavirus that is now named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the cause of coronavirus disease 2019 (COVID-19). The disease is mild in most people (∼80%). During the COVID-19 pandemic, in many countries the crisis has quickly overwhelmed the capacities of healthcare systems, leading to major challenges in their ability to respond [1, 2]. In Greece, we managed to control the pandemic by eliminating the number of cases and by keeping mortality rates within acceptable limits. As of 4 July 2020, the National Public Health Organisation reported 3511 cases (55% male) with 192 deaths; 517 patients were hospitalised. 811 (23%) of the total cases were linked to travelling abroad, while 1933 (55.1%) were linked to exposure to a confirmed case. Following extended discussions with primary care physicians and after fully considering our experiences during hospital emergencies, these findings suggest that primary care in Greece may have played a key role in the management of suspected cases of SARS-CoV-2, perhaps relieving the referral hospitals from suspect and mild cases, and critically contributing to our success story during the pandemic.
Primary care played a key role in the management of suspected cases of SARS-CoV-2, and reduced patients' access to referral hospitals. Advice, telephone risk assessment and a well-described testing pathway for patients from the authorities limited the stream of cases presenting at hospital. Indeed, primary care played a significant role in categorising and differentiating suspected patients based on case severity and risk factors, guiding treatment and management accordingly. It is important to emphasise that the primary care system in Greece is mainly based on specialists and not general practitioners. This particular characteristic is quite important, as it means experienced and focused clinicians are managing conditions that require specialty assessment.
As ∼80% of people with COVID-19 have uncomplicated or mild illness [3, 4], early recognition and isolation of suspected cases has been extremely important to contain virus transmission. Mild illness may include uncomplicated upper respiratory tract viral infection symptoms, such as fever, fatigue, cough, anosmia, anorexia, malaise, muscle pain, sore throat, nasal congestion, headache and gastrointestinal symptoms such as diarrhoea, absence of dyspnoea and absence of clinical signs compatible with increased respiratory rate [5, 6]. We strongly believe that, additionally, a near-normal or normal oxygen saturation measure by pulse oximetry (SpO2) (usually >94%) is an important parameter for characterising these patients as mild. Another critical parameter relating to more severe COVID-19 disease is the presence of comorbidities in combination with older age. The recognition of patients who are more vulnerable to infection with SARS-CoV-2 is of utmost importance because it may orientate the clinicians towards the patients who are most likely to deteriorate. Given the results of other studies, it was evident that age and comorbidities were the most important determinants of a poor prognosis of COVID-19 [7].
Our approach to risk stratification is summarised in table 1. We believe that this stratification, used in primary care in Greece, positively affected the healthcare system and diminished the number of cases for hospital assessment. In our opinion, there are three crucial parameters in such stratification: experienced evaluation by specialists, widespread use of pulse oximeters as part of home care and grading of dyspnoea. These three parameters allowed us to clearly stratify patients and follow them properly. Furthermore, it allowed the healthcare system to evaluate and carefully monitor the more severe cases. A clear action plan was provided, counselling patients about the signs and symptoms of complicated disease and when exactly they should seek urgent care through designated COVID-19 hospitals in case of worsening of symptoms. Finally, the general public were informed about the importance of general standard precautions and personal hygiene, including hand hygiene and social distancing [8].
Categorisation of suspected patients based on case severity and risk factors for severe coronavirus disease 2019
With regard to risk stratification, we characterised the following as mild and home care patients: no comorbidities, <65 years old, symptoms for <7 days that did not involve dyspnoea and SpO2 of >94%. We used the cut-off point of 7 days as we strongly believe that prolonged symptoms, even in the absence of dyspnoea, are compatible with the presence of COVID-19-related pneumonia [9]. For dyspnoea assessment, we avoided simple questions with possible yes or no answers, and used specific features that characterise dyspnoea only on exertion or even at rest. The latter allowed our patients to overcome the dichotomous process and to express their dyspnoea in a more realistic way. The other two stratification risks are more complicated since the presence of one characteristic may overcome the absence of others.
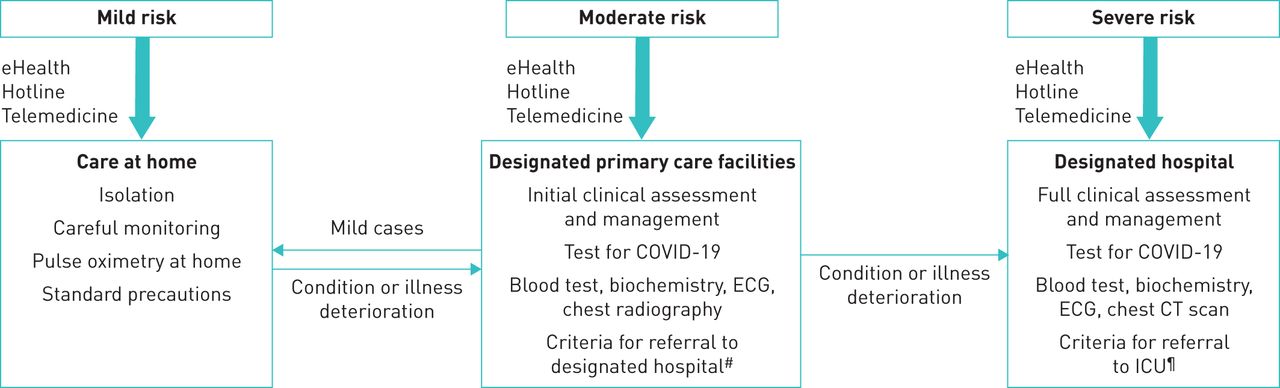
Our suggested algorithm after risk stratification is provided in figure 1. The mild-risk patients need careful monitoring, proper use of an oximeter at home, standard precautions and eHealth facilities, which allow them to discuss any changes in disease status. A PCR-based test at home is not obligatory for these patients. Any clinical deterioration moved them a step forward in risk and to a different clinical assessment.
{kind=link}
Suggested algorithm for the management of different risks based on initial stratification. #: signs and symptoms of severe illness, such as altered mental status, dyspnoea, oxygen saturation measured by pulse oximetry <94% at room air, respiratory rate >30·min−1, systolic blood pressure <90 mmHg, shock. ¶: impending respiratory failure, acute respiratory distress syndrome, septic shock, life-threatening organ dysfunction.
In general, patients with moderate or severe risk were referred to designated COVID-19 hospitals for clinical assessment. Even those with moderate risk were assessed at hospital or at primary care-designated level. These patients had fever for <7 days and SpO2 of >94% at room air, mild dyspnoea and laboratory test results such as lymphocytes >800/μL, C-reactive protein levels <1.5 mg·dL−1 (upper normal limit 0.5 mg·dL−1) and ferritin <500 μg·L−1, without any infiltrates on chest radiograph. These patients were advised to self-isolate at home and followed the mild risk assessment.
Finally, critical patients presenting with severe symptoms, including altered mental state, shortness of breath, tachypnoea with an increased respiratory rate of >30/min, an SpO2 of <94% at room air, hypotension with systolic blood pressure <90 mmHg or other signs of shock, were urgently admitted at referral to COVID-19 hospitals or intensive care units (ICUs). Early identification of those with severe illness and rapid admission to designated hospitals or ICU ensures optimised supportive care treatment and survival. Regarding severe risk, the absence of fever is compatible with disease deterioration leading to shock [5].
In our algorithm in Greece, primary care services and dedicated community health workers played a major role, contributing significantly to the successful management of the COVID-19 pandemic seen in Greece. The development of eHealth facilities, including a COVID-19 telephone hotline, telemedicine, online platforms and smart phone facilities, contributed significantly to appropriate assessment and successfully directing suspected patients towards designated healthcare facilities for COVID-19. Installing such programs allows minimal contact between healthcare workers and patients, and lightens the workload in healthcare facilities. The Greek experience revealed that harmonised collaboration among primary care, secondary facilities, designated hospitals and official authorities may result in the prompt and accurate management of such crises.
Footnotes
Conflict of interest: I. Tomos has nothing to disclose.
Conflict of interest: K. Kostikas was an employee of Novartis until October 2018.
Conflict of interest: G. Hillas has nothing to disclose.
Conflict of interest: P. Bakakos has nothing to disclose.
Conflict of interest: S. Loukides has nothing to disclose.
- Received July 5, 2020.
- Accepted July 9, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










