





Abstract
Pulmonary rehabilitation, whether performed at home or in a specialised centre, is effective in the management of COPD. As gender-related differences in COPD were previously reported, we aimed to evaluate the impact of gender on pulmonary rehabilitation outcomes in the short, medium and long term.
In this retrospective observational study of 170 women and 310 men with COPD, we compared the outcomes of an 8-week home-based pulmonary rehabilitation programme including an individualised plan of retraining exercises, physical activities, therapeutic education, and psychosocial and self-management support. Exercise tolerance, anxiety, depression, and quality of life (QOL) were assessed using the 6-min stepper test (6MST), Hospital Anxiety and Depression Scale (HADS) and Visual Simplified Respiratory Questionnaire (VSRQ), respectively. Assessments were carried out before, immediately after the pulmonary rehabilitation programme (T2) and at 8 (T8) and 14 months (T14).
At baseline, women were younger (mean 62.1 versus 65.3 years), more often nonsmokers (24.7% versus 7.7%) and had a higher body mass index (28 versus 26.4 kg·m−2). They more often lived alone (50.6% versus 24.5%) and experienced social deprivation (66.7% versus 56.4%). They had significantly lower exercise tolerance (−34 strokes, 6MST) and higher anxiety and depression (+3.2 HADS total score), but there were no between gender differences in QOL (VSRQ). Both groups showed similar improvements in all outcome measures at T2, T8 and T14 with a tendency for men to lose QOL profits over time.
Despite some differences in baseline characteristics, women and men with COPD had similar short-, medium- and long-term benefits of a home-based pulmonary rehabilitation programme.
Abstract
Despite some differences in baseline characteristics, women and men with COPD had similar short-, medium- and long-term benefits of a home-based pulmonary rehabilitation programme https://bit.ly/2XfFakK
Introduction
The prevalence of chronic obstructive pulmonary disease (COPD) among women is steadily increasing due in large part to more frequent occupational exposure to noxious particles and increased smoking among women since the 1960s [1]. Habits have changed, and women also find it more difficult than men to quit smoking and to remain nonsmokers [1, 2]. Despite the increasing prevalence, the diagnosis of COPD is often delayed in women, who report higher difficulties in meeting a specialist and feel the time of consultation to be insufficient compared with male patients [3]. With similar smoking habits, women with COPD generally have a more severe disease, experience worse dyspnoea and quality of life (QOL) and have a higher risk of hospitalisation [2]. Taken together, COPD-related factors could hamper the attendance to pulmonary rehabilitation and its benefits. As a result, whereas mortality from COPD has declined among men since the early 2000s, it has remained stable among women [4]. Hence, there is an urgent need to improve screening and treatment strategies for women with COPD.
Pulmonary rehabilitation is a comprehensive patient-focused treatment that combines retraining exercises, physical activities, therapeutic education and self-management support [5]. In COPD, it has demonstrated effectiveness in improving exercise tolerance, dyspnoea, QOL, anxiety and depression, and in reducing exacerbation frequency, the duration of hospitalisations and COPD-related health costs [5, 6]. We and others have shown that home-based pulmonary rehabilitation programmes are effective in improving exercise tolerance, dyspnoea and QOL in patients with COPD [7, 8].
Gender, as opposed to the term sex, commonly used to refer to the biological characteristics that define men and women, refers to the socially and culturally constructed roles, behaviours and attributes that a given society considers appropriate for men and women. Although gender is considered as a determinant of health in the same way as age, socioeconomic level, culture and ethnicity [9], only a few studies have investigated the impact of being a woman defined by the term gender in pulmonary rehabilitation outcomes. A systematic review on this subject concluded that studies showed insufficient evidence and conflicting results across studies [10]. Recently, Spielmanns et al. [11] found no difference between genders in exercise tolerance improvement after pulmonary rehabilitation. Nguyen et al. [12] confirmed the previous short-term results but mentioned that QOL was improved only in women. To our knowledge, no study has evaluated the impact of gender on long-term outcomes in a home-based setting.
The aim of our study was to determine whether gender influenced the outcomes of a home-based pulmonary rehabilitation programme in COPD patients over the short-, medium- and long-term.
Methods
Patients
In a retrospective study, we analysed data from all consecutive COPD patients undergoing a home-based pulmonary rehabilitation programme between January 2010 and July 2017 provided by FormAction Santé, Northern France. The study population included 480 patients (figure 1) referred by their pulmonologist for a home-based pulmonary rehabilitation programme because of disabling dyspnoea despite optimal treatment. Patients decided to participate in a centre- or home-based pulmonary rehabilitation programme according to personal preference and/or unavailability of a pulmonary rehabilitation centre close to the patient's home. Exclusion criteria included the occurrence of exacerbation in the preceding 4 weeks, lung cancer, dementia, uncontrolled psychiatric illness or any serious condition (cardiovascular, neurological, osteoarticular, etc.) that could prevent physical activity or be exacerbated by exercise. The prescribing physician was responsible for the diagnosis and assessment of COPD and comorbidities, treatments (other than pulmonary rehabilitation), validation of the absence of contraindications to exercise and determination of the retraining target heart rate. Social deprivation was assessed using the Evaluation of Deprivation and Inequalities in Health Centres (EPICES) multidimensional questionnaire [13], which evaluates social deprivation on a quantitative and continuous scale ranging from 0 (no deprivation) to 100 (maximum deprivation). Forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV1) were measured at baseline by spirometry.

Flow chart.
This study was conducted in accordance with the principles described in the amended Declaration of Helsinki and approved by the Committee for the Evaluation of Observational Research Protocols of the French Language Pulmonary Society (CEPRO 2017-007). All patients provided written informed consent for the use of the data.
Pulmonary rehabilitation programme
The home-based pulmonary rehabilitation programme has been described previously in detail [8, 14]. Briefly, it consisted of a 1.5-hour in-home session per week, supervised by a member of the pulmonary rehabilitation team, for 8 weeks, with unsupervised exercises during the other days of the week, and one visit 6 and 12 months after the end of pulmonary rehabilitation. The pulmonary rehabilitation programme started with an evaluation of the patient's needs and expectations leading to the formulation of a personalised plan. Educational, motivational and self-management plans were designed and implemented through a collaborative process between the pulmonary rehabilitation team, the patient and his/her caregiver [15]. Follow-up visits were restricted to the planned assessments; otherwise, patients were followed by health professionals according to their usual schedule of care.
Endurance exercises were performed on a cycle ergometer or a stepper at the target heart rate, with the goal of working up to 30 to 45 min daily [8]. For very severe COPD patients, exercise training was started with a duration of a few minutes repeated several times a day, with the goal of reaching 10 min at a time and 30 to 45 min per day. If necessary, an oxygen supply was delivered. Patients managed their exercise intensity based on dyspnoea (target of 3–4 on a Borg 1–10 scale) or perception of effort (target of 11–13 on a Borg 6–20 scale). Strengthening exercises with dumbbells and/or elastibands were offered, to be performed in 10-min sessions for 5 days a week, depending on the patient's abilities and motivations, as well as balance exercises.
The programme was focused on the resumption of daily activities (e.g., walking, cleaning, gardening and shopping) according to the patient's wishes and environment, with the goal of facilitating long-term integration of the programme into the patient's lifestyle and circumstances.
Assessments
Assessments were performed at home at baseline, at the end of the 8-week pulmonary rehabilitation programme (T2), and at 8 (T8) and 14 months (T14) after baseline. Exercise tolerance was assessed by the 6-min stepper test (6MST) [16], anxiety and depression by the Hospital Anxiety and Depression Scale (HADS) [17] and QOL by the Visual Simplified Respiratory Questionnaire (VSRQ) [18]. The minimally clinically important differences (MCIDs) were 40 strokes for the 6MST [19], 1.5 points for HADS-Anxiety, 1.5 points for HADS-Depression [17] and 3.4 points for VSRQ [18]. Patients were considered “responders” if their test scores improved by at least the MCID between T0 and T2, T8, or T14.
Statistical analysis
Patients were classified according to their biological sex. Quantitative variables are presented as mean and sd or median and interquartile range according to the normality of distribution, as determined graphically and by the Shapiro–Wilk test. Qualitative variables are presented as frequencies and percentages. Categorical variables were compared using Chi-squared tests. Quantitative variables were compared using Student's parametric tests when normally distributed, otherwise using nonparametric Wilcoxon tests. Baseline variables (6MST, VSRQ HADS-Anxiety and HADS-Depression) and all changes from baseline (T0) to T2, T8 or T14 were compared between men and women using covariance analysis (ANCOVA).
Global progressions of parameters were compared between the two patient groups (women versus men) using linear mixed models by adjusting the value to baseline. Quality of the linear models was verified by analysis of residuals. In the case of non-normality of residuals, the data were log-transformed. All analyses (ANOVA and linear mixed models) were adjusted for confounding factors (age, body mass index (BMI), living arrangement, smoking status, FEV1 percentage of predicted, EPICES and coronary artery disease or peripheral vascular disease). The significance threshold was set at 0.05. All analyses were performed using SAS software version 9.4 (SAS Institute, Cary, NC, USA).
Results
The study population was composed of 480 patients (mean age 64.2 years) with severe COPD (mean FEV1 36% pred), including 170 women (35.4%) (table 1). Compared with men, women were significantly younger and had significantly higher BMI and FVC, whereas FEV1 and Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages distribution were similar between genders. Women more often lived alone, were non-smokers and presented with social deprivation. Women were also less likely to have coronary artery or peripheral vascular diseases, or sleep apnoea syndrome than men (15.9% versus 32.3%, p<0.001; 14.1% versus 22.2%, p=0.03, respectively). While diagnosed anxiety, depression, dysthyroidism and osteoporosis were significantly more common in women (40.2% versus 29.8%, p<0.001; 30.5% versus 19.4%, p<0.01; 19.4% versus 3.5%, p<0.001; 12.3% versus 4.5%, p=0.002; respectively), asthma and chronic heart failure prevalence were not different between genders.
Baseline characteristics
The percentage of men and women evaluated at the different steps of the study did not differ significantly (89.4% versus 91.9% at T2, 80% versus 79.7% at T8 and 71.8% versus 69.7% at T14) neither did the withdrawal reasons or number of deaths (p=0.12) (figure 1). No incidents or accidents related to the pulmonary rehabilitation programme were reported. Compared with patients who completed the study, those who dropped out during the 14-month study for any reason (n=140, 29.2%) including death, presented with a more severe disease at baseline (FEV1 33.5% versus 41%, p<0.001), more often received long-term oxygen therapy (LTOT) (80% versus 60.9%, p<0.001) and/or noninvasive ventilation (41.4% versus 30.9%, p=0.027), and were more often affected by coronary artery or peripheral vascular diseases (36.4% versus 22.4%, p<0.001). Death occurred in 42 patients (8.7%) who were older (69.1 versus 63.7 years, p<0.001), had lower exercise tolerance (6MST 230.8 versus 315.2 strokes, p<0.001), received LTOT more frequently (85.7% versus 64.6%, p=0.006), and more often suffered from heart failure (26.2% versus 10%, p=0.004) and rhythm disorders (31% versus 16.4%, p=0.019) compared with the survivors.
At baseline, women had significantly higher total HADS and HADS-Anxiety scores as well as HADS-Depression scores after adjustment for confounding factors and completed significantly fewer strokes in the 6MST compared with men (table 2). VSRQ score was not statistically different between groups.
Assessments at baseline
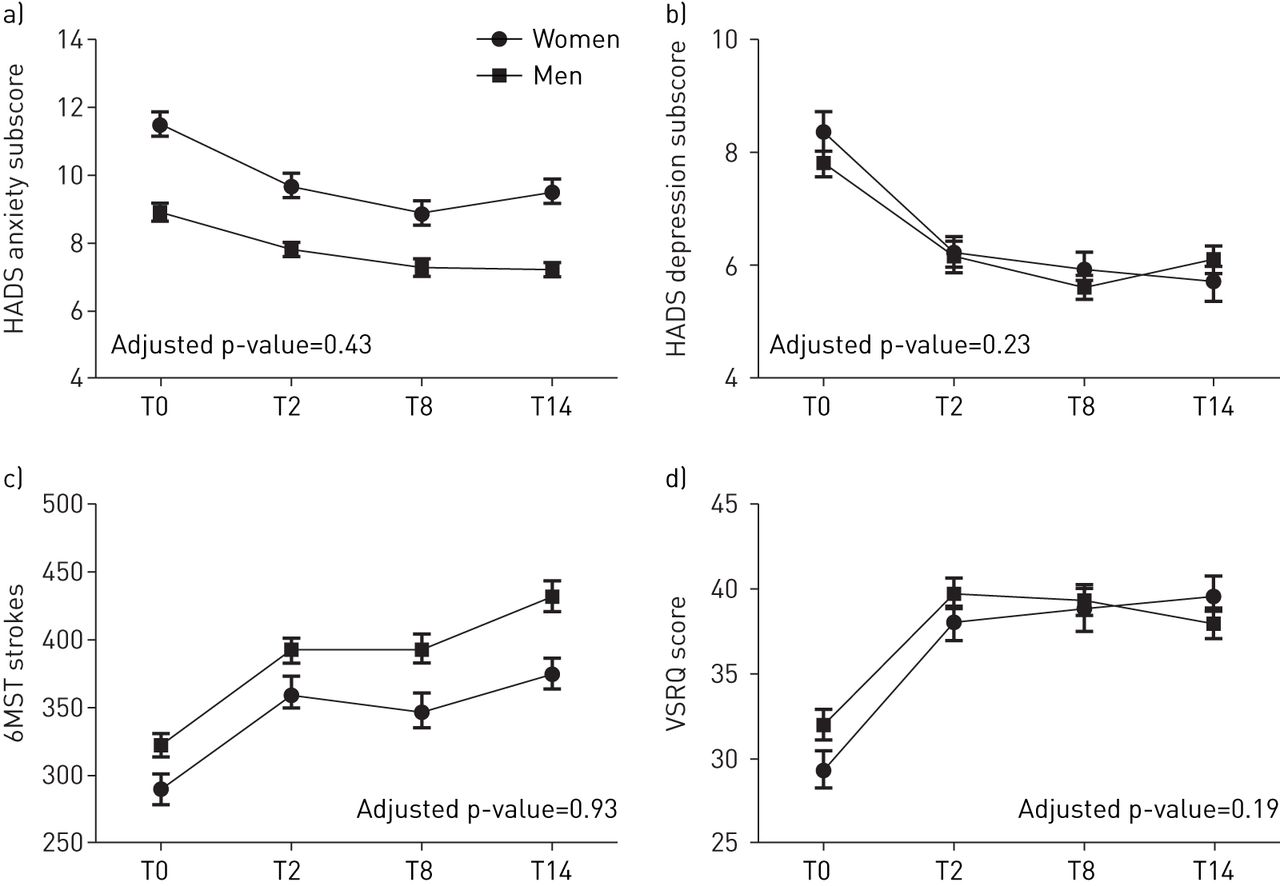
Men and women showed similar improvements in outcomes measured at 2, 8 and 14 months after the start of the pulmonary rehabilitation programme (figure 2 and table 3). After adjustment to confounders, there was no impact of gender on the magnitude of improvement in 6MST strokes and HADS scores (total, anxiety and depression). The improvement in the VSRQ score was significantly higher in women than men between T0 and T2 only after adjustment and this difference was also found at T14 with or without adjustment. The percentage of men and women who met the definition of a pulmonary rehabilitation responder (≥MCID change from baseline in at least one of the four outcome measures) tended to decrease over time but was not significantly different between men and women at T2, T8 or T14 (table 4). With respect to individual outcomes, the percentage of patients with ≥MCID change in HADS-Anxiety subscore differed significantly only at T8 (37% women versus 50% men, p=0.02) (figure 3). In contrast, a greater proportion of women showed ≥MCID improvement in the VSRQ score at T14 (64.6% versus 52.1%, p=0.04).

Changes in exercise tolerance, quality of life, anxiety and depression in COPD patients according to gender. (a–d) Changes in parameters from T0 (baseline) to T2, T8 and T14 (2, 8 and 14 months after T0) for (a) Hospital Anxiety and Depression Scale (HADS) anxiety subscore, (b) HADS-depression subscore, (c) 6-min stepper test (6MST) stroke number and (d) Visual Simplified Respiratory Questionnaire (VSRQ) score. Data are presented as the mean±sem at each time for the whole population. p-values are adjusted for baseline value of age, body mass index, living arrangement, smoking status, forced expiratory volume in 1 s (FEV1) (% pred), EPICES (Evaluation of Deprivation and Inequalities in Health Centres) score, and coronary artery disease or peripheral vascular disease. p-value is the Pinteraction for the interaction between time and group (i.e. <0.05 indicates a significant difference in the change in variable with time compared between the two patient groups). All analyses were adjusted to the baseline value. Minimum–maximum scores: HADS total, 0–42; HADS subscores, 0–21 (low to high anxiety/depression); VSRQ, 0–80 (low to high quality of life).
Changes in outcome measures in women and men with chronic obstructive pulmonary disease (COPD) at 2, 8 and 14 months after initiation of pulmonary rehabilitation
Percentage of pulmonary rehabilitation responders according to gender

{kind=link}
{kind=link}
{kind=link}
Percentage of patients who responded to pulmonary rehabilitation according to gender. Data are presented as the percentage of patients who responded to pulmonary rehabilitation, with response defined as a change of ≥MCID for the indicated assessments at 2 (T2), 8 (T8) and 14 (T14) months compared with the start of the pulmonary rehabilitation programme. 6MST: number of strokes in the 6-min stepper test; MCID: minimum clinically important difference; VSRQ: Visual Simplified Respiratory Questionnaire. *: p<0.05.
Discussion
The results of this retrospective observational study identified no gender-based differences in the outcomes of a home-based pulmonary rehabilitation programme in COPD patients. In our study, women entering a home-based pulmonary rehabilitation programme in comparison with men were younger, had a higher BMI, and were less likely to be smokers or to present with coronary artery or peripheral vascular diseases. They more often lived alone, had a higher level of social deprivation, and had greater levels of anxiety, depression and exercise intolerance. Nevertheless, women and men showed similar beneficial effects of pulmonary rehabilitation on depression, anxiety, QOL and exercise tolerance, and they were similarly able to sustain these benefits for up to 1 year thereafter with a tendency for men to lose QOL profits over time.
Epidemiological characteristics of our study population are consistent with previous studies of COPD patients, in that the women were younger and less often smokers than men with the same degree of airflow limitation [2]. An audit of several outpatient pulmonary rehabilitation programmes in the UK found that COPD patients with lower socioeconomic status were less likely to adhere to the programme, but those who did complete the programme had similar outcomes to patients with higher socioeconomic status [20]. In our study, although the women were more socially deprived than the men, they showed similar attendance to the home-based pulmonary rehabilitation programme, suggesting that this modality could better meet their needs and overcome their socioeconomic limitations compared with outpatient or inpatient pulmonary rehabilitation programmes. This is an important finding because non-attendance and premature cessation are common during pulmonary rehabilitation programmes. Identified predictors of pulmonary rehabilitation non-attendance are socioeconomic disadvantage, advanced age, active smoking, severe obstruction, LTOT use, low QOL and distance from a pulmonary rehabilitation site [21]. Our results suggest that gender does not affect the long-term attendance to home-based pulmonary rehabilitation. Home-based programmes have considerable advantages for patients who are otherwise unable to visit a pulmonary rehabilitation centre by allowing them to benefit from a personalised pulmonary rehabilitation programme that takes into account constraints in their daily activities and living environment.
In the present study, women with COPD had higher baseline anxiety and depression scores than men, which is consistent with a report that anxio-depressive disorders were twice as common in women than men with COPD (56% versus 35% with anxiety symptoms, 38% versus 13% with depression symptoms), despite there being no difference in COPD severity [22]. Anxiety disorders are known to alter therapeutic observance [23] and attendance to pulmonary rehabilitation programmes[24], making it reasonable to assume that they may also impact pulmonary rehabilitation outcomes. There is a paucity of data on how gender affects the benefits of pulmonary rehabilitation on psychological outcomes. Haave et al. [25] reported that men and women with COPD showed similar improvements in the trait portion of the Spielberger State–Trait Anxiety Inventory after pulmonary rehabilitation, whereas Nguyen et al. [12] found that women had more marked improvements than men in depression based on the Patient Health Questionnaire-9, and neither group showed improvement in anxiety based on the Generalised Anxiety Disorder-7 score. In contrast, in the present study, we found significant and comparable improvements in HADS-Anxiety and HADS-Depression scores in both men and women in the short, medium and long term after pulmonary rehabilitation, suggesting that the choice of evaluation tools may be responsible for discrepancies between studies.
Consistent with some previous reports, we found that QOL at baseline was not significantly different between women and men with COPD [26, 27]. However, other studies have reported lower global QOL scores in women with COPD [28, 29] or found significant gender differences in specific components of QOL evaluation [30, 31]. The discrepancies between these studies may reflect the difficulty of examining gender differences with such a broad outcome measure as QOL, which may be affected by numerous other factors, such as deterioration of exercise tolerance, changes in stress and comorbidities. In our study, QOL improvement at the end of pulmonary rehabilitation was statistically but not clinically higher in women after adjustment for confounders. Our results are in accordance with most studies in this area, which have found no effect of gender on improvement in QOL after pulmonary rehabilitation, independently of the evaluation tool used [11, 25, 32–36]. Only two studies to date have reported a gender difference in QOL in COPD patients; one found that women benefited more from pulmonary rehabilitation than men [12, 37] and the second found the reverse [38]. In our population, a higher percentage of women showed a clinically significant improvement in the long term. This is mainly due to the gradual decline in the percentage of male responders while the proportion of female responders remained stable. This finding suggests that there may be a gender difference in COPD patient ability to maintain the beneficial effects of pulmonary rehabilitation on QOL over the long term. This is an important observation because, to our knowledge, only two other studies of COPD patients [26, 27] have compared gender differences in QOL at 6 months after pulmonary rehabilitation, and no studies have investigated such differences at 12 months after pulmonary rehabilitation.
In our study population, women with COPD had lower exercise tolerance than men with the same degree of airflow limitation as reported by other groups [11, 32, 39]. No gender differences have been reported in the short-term benefits of pulmonary rehabilitation on exercise tolerance in COPD patients [11, 12, 25, 33, 35–37, 40], with the exception of Skumlien et al. [38] who reported greater improvement in men. Our study additionally found no gender-based differences in exercise tolerance over the medium and long term after pulmonary rehabilitation. This durability of improvement may be due, at least in part, to the integration of patient-selected physical activities of daily living from the start of the pulmonary rehabilitation programme.
Our study is limited by its retrospective and observational design. A recruitment bias was possible, because selection of home-based pulmonary rehabilitation was based on patient's personal choice and/or geographical distance from a rehabilitation centre and some patients were lost to follow-up before the long-term reassessment. However, this possible recruitment bias should be the same between men and women. We can even suggest that because of specific social roles attributed to women by the society, a home-based programme could facilitate the attendance and adherence in women, compared to traditional settings. Moreover, as previously reported, this modality of pulmonary rehabilitation is as effective as programmes taking place in rehabilitation facilities with good attendance rates and provides an innovative solution to better meet the patient's needs. Finally, our classification criterion being biological sex, patients who identify themselves as belonging to a gender different to their biological sex could have been misclassified. As sex is a main determinant of gender and identity construction, this should only concern a few patients. Furthermore, gender seems more appropriate to describe our groups as pulmonary rehabilitation responses seem more determined by the individual as a whole and not only dictated by sex-related biological characteristics.
In conclusion, this study shows that despite being younger, more socially deprived, more anxious and having a reduced exercise tolerance compared with men, women with COPD showed similar benefits from home-based pulmonary rehabilitation on exercise tolerance, anxiety and depression on a short-, medium- and long-term basis. QOL is more improved in women with a tendency for men to lose profits over time.
Acknowledgements
We thank members of the rehabilitation team at FormAction Santé: Sophie Duriez, Mathieu Grosbois, Marjorie Lambinet, Valentine Opsomer, Gaelle Tywoniuk, Florence Urbain and Virginie Wauquier. The authors also wish to thank Anne M. O'Rourke for editing a version of the manuscript.
Footnotes
Author contributions: J-M. Grosbois, B. Wallaert, F. Machuron and A.S. Diot had full access to all data, and take responsibility for the integrity of the data and the accuracy of data analysis, including and especially any adverse effects. J-M. Grosbois, O. Le Rouzic, C. Chenivesse, B. Wallaert, S. Gephine, M. Kyheng and G. Terce contributed substantially to the study design, data analysis and interpretation, and writing of the manuscript.
Conflict of interest: J-M. Grosbois reports FormAction Santé (J-M. Grosbois) received financial support from Adair, Aeris Santé, Bastide, France Oxygène, Homeperf, LVL Medical, Medopale, NorOx, Santélys, Santeo, SOS Oxygène, Sysmed, VitalAire and the ARS Hauts de France for the home-based pulmonary rehabilitation programme; personal fees and nonfinancial support from AstraZeneca and Boehringer Ingelheim, personal fees from Chiesi, nonfinancial support from GlaxoSmithKline and Novartis, and personal fees from Vitalaire and Roche, during the conduct of the study.
Conflict of interest: S. Gephine has nothing to disclose.
Conflict of interest: A.S. Diot has nothing to disclose.
Conflict of interest: M. Kyheng has nothing to disclose.
Conflict of interest: F. Machuron has nothing to disclose.
Conflict of interest: G. Terce has nothing to disclose.
Conflict of interest: B. Wallaert reports personal fees and nonfinancial support from Roche and Boehringer Ingelheim, and nonfinancial support from Vitalaire, outside the submitted work.
Conflict of interest: C. Chenivesse reports grants from AstraZeneca and Santélys, personal fees from ALK-Abello, AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, Roche, Sanofi and TEVA, and nonfinancial support from ALK-Abello, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, MEDA Pharma, Medexact, Novartis, Pierre Fabre and Pfizer, outside the submitted work.
Conflict of interest: O. Le Rouzic reports personal fees and nonfinancial support from AstraZeneca, Boehringer Ingelheim, Chiesi, Lilly and Novartis, and nonfinancial support from GlaxoSmithKline, MundiPharma, Pfizer, Teva, Santelys Association, Vertex and Vitalaire, outside the submitted work.
- Received January 21, 2020.
- Accepted July 25, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










