





Abstract
Background Noninvasive ventilation (NIV) is considered as the first-line treatment for acute exacerbation of COPD (AECOPD) complicated by respiratory acidosis. Recent studies demonstrate a role of nasal high-flow oxygen (NHF) in AECOPD as an alternative treatment in patients intolerant to NIV or with contraindications to it.
Aim The study aimed to evaluate whether NHF respiratory support is noninferior compared to NIV in respect to treatment failure, defined as need for intubation or change to alternative treatment group, in patients with AECOPD and mild-to-moderate acute or acute-on-chronic hypercapnic respiratory failure.
Methods We designed a multicentre, prospective, randomised trial on patients with AECOPD, who have pH<7.35 but >7.25 and PaCO2 >45 mmHg, in whom NIV is indicated as a first-line treatment. According to power analysis, 498 participants will be required for establishing noninferiority of NHF compared to NIV. Patients will be randomly assigned to receive NIV or NHF. Treatment will be adjusted to maintain SpO2 between 88%–92% for both groups. Arterial blood gases, respiratory variables, comfort, dyspnoea score and any pulmonary or extrapulmonary complications will be assessed at baseline, before treatment initiation, and at 1, 2, 4, 6, 12, 24, 48 h, then once daily from day 3 to patient discharge, intubation or death.
Conclusion Given the increasing number of studies demonstrating the physiological effects of NHF in COPD patients, we hypothesise that NHF respiratory support will be noninferior to NIV in patients with AECOPD and mild-to-moderate acute or acute on chronic hypercapnic respiratory failure.
Abstract
Nasal high-flow oxygen could be an effective alternative to NIV respiratory support for patients with mild-to-moderate #AECOPD, especially for those who do not tolerate or have contraindications for NIV https://bit.ly/3bgxDYx
Introduction
COPD exacerbations are events of great importance in the progression of the disease, imposing considerable burden on quality of life, lung function, morbidity and mortality [1]. They are defined as events of acute worsening of respiratory symptoms that result in additional therapy and are characterised by variable clinical manifestations and causative factors [1, 2].
The underlying pathophysiology of COPD exacerbations include severe expiratory flow limitation which, in combination with the characteristic rapid shallow breathing pattern, cause dynamic hyperinflation and detrimental mechanical effects. The acute decompensation of chronic adaptive mechanisms results in acute respiratory failure which is characterised by hypoxaemia, and, often accompanied by carbon dioxide (CO2) retention and acidaemia [2].
Noninvasive ventilation (NIV) has been considered the first-line treatment for acute exacerbations of COPD (AECOPD) accompanied by respiratory acidosis [3], as it reduces endotracheal intubation rates and overall mortality [4]. However, the failure rate in NIV ranges from 15 to 24% for COPD patients [5] and a great percentage of patients (∼30%) present with contraindications to NIV, are unable to tolerate NIV or have poor mask fit [6].
Over the last decade, nasal high flow (NHF) has emerged as an innovative oxygen delivery device. The operating principle is based on the administration of heated and humidified gas mixture delivered at high flows through large-bore nasal cannula [7], resulting in reduction in work of breathing [8]. The simplistic nature of the device has favourable effects on patients’ cooperation and tolerance of the treatment. The beneficial effects of NHF arise from several mechanisms, which include the high and stable inspiratory oxygen fraction, decrease in anatomical dead space, and positive airway pressure generation [9]. Despite the fact that the role of NHF in the management of hypoxaemic respiratory failure is well established [8, 10], there are no explicit data for its application in COPD patients. One possible explanation of this could be that the studies indicating any beneficial effects of NHF in COPD patients have only just been published [11–14]. They have shown that NHF can reduce arterial CO2 and work of breathing in patients with stable COPD [11, 12] as well as improve modified Medical Research Council dyspnoea scale and quality of life [13, 14]. Additionally, NHF has been used to provide respiratory support in patients with AECOPD who were intolerant of NIV, with successful outcomes [15–17]. However, randomised controlled trials comparing the efficacy of NHF to NIV as first-line treatment in patients with AECOPD have not yet been conducted. It appears that NHF has a role in treating type II respiratory failure and could be used as a rescue therapy when intubation and NIV are contraindicated or NIV is not tolerated, as complementary therapy during breaks off NIV, and even as an alternative to NIV in carefully selected and closely monitored patients.
This manuscript describes a study protocol, which evaluates respiratory support provided by NHF compared to NIV in patients with AECOPD and mild-to-moderate acute or acute on chronic hypercapnic respiratory failure. We hypothesise that NHF will be noninferior to NIV in this patient population.
Methods
Study design
This is a prospective, unblinded, multicentre, noninferiority randomised controlled trial. Block randomisation will be conducted using randomly selected block sizes. Due to the research design, neither the individual collecting data nor the patient can be blinded to treatment allocation.
The study will be conducted in the emergency department and medical ward of four Greek hospitals: General Hospital of Evangelismos, Athens; General Hospital for Thoracic Diseases Sotiria, Athens, University Hospital of Larissa, Thessaly and Venizeleio General Hospital, Heraklion, Crete. The protocol was approved by the relevant Ethics Committee for all the participating centres. The study was prospectively registered in Clinical Trials.gov in July 2018 (NCT03466385). Consent to participate in the trial will be obtained from all patients or next of kin and the study will be conducted according to ICH-GCP and clinical trial regulations. Site investigators or the study coordinator have informed consent delegation. In order to achieve consistency in our study, site investigators, study coordinators and research staff involved in data collection and data recording from different sites are centrally trained in the trial protocol and standard operating procedures. The data manager will receive all case report forms electronically for the statistical analysis. REDCap (research electronic data capture) will be used for data collection and management and it will be managed by the biostatistician. Furthermore, data will be remotely monitored and checked by a clinical research associate and site investigators will be provided with regular data monitoring reports, which will be actioned where appropriate.
Study population
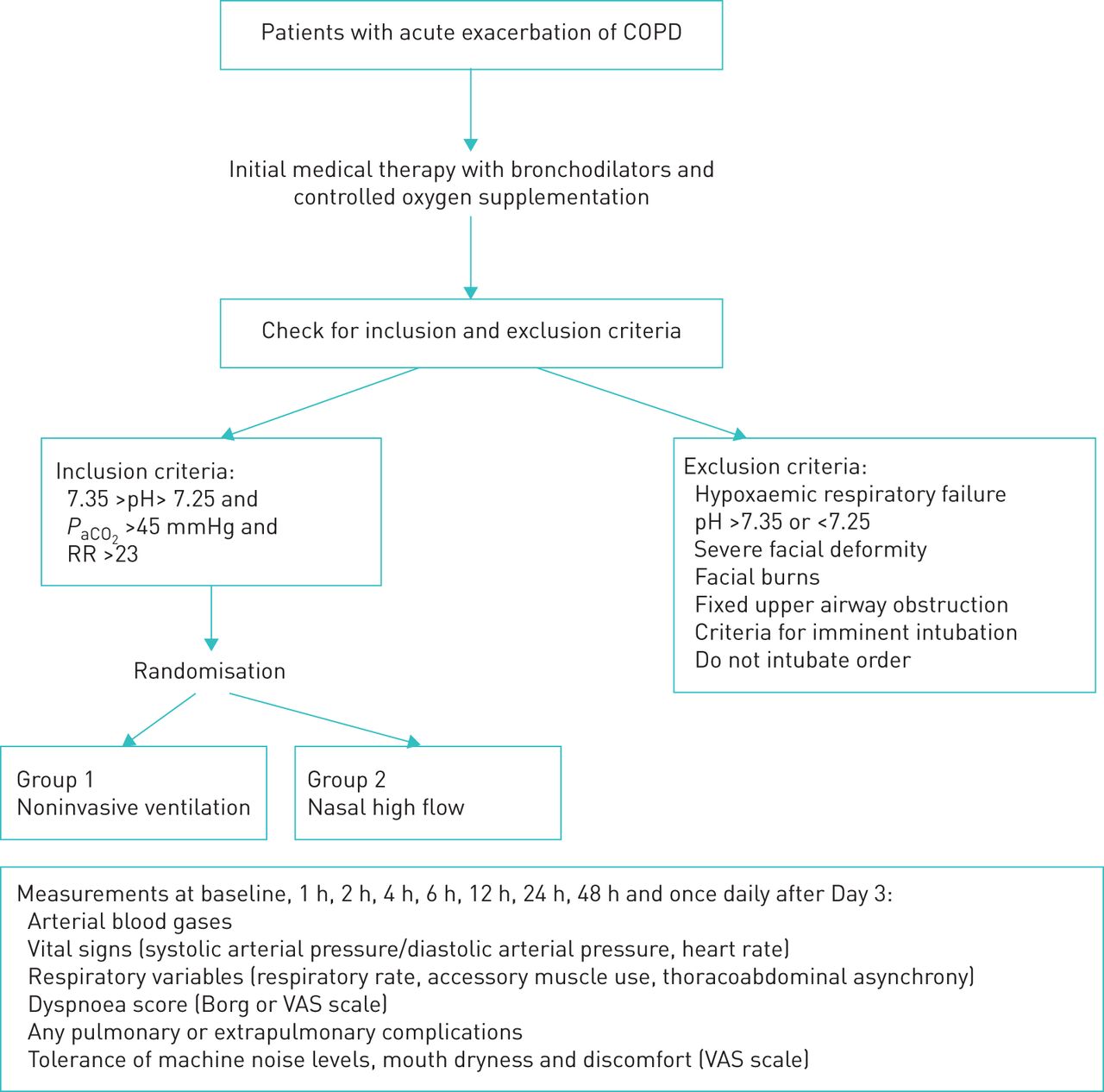
Patients considered eligible for the study will be those admitted to the emergency department or hospitalised in medical ward with AECOPD (defined as any worsening of the patient's respiratory symptoms that is beyond normal day-to-day variations and leads to change in medication) combined with mild-to-moderate acute or acute on chronic hypercapnic respiratory failure (defined as 7.35>pH>7.25 and arterial CO2 tension (PaCO2) >45 mmHg), who have indication for NIV treatment initiation (i.e. pH<7.35, PaCO2>45 mmHg, and respiratory rate >23 breaths·min−1 persisting after initial medical therapy with bronchodilators and controlled oxygen supplementation) [6, 18] (figure 1). Patients will be excluded if they meet one or more of the following criteria: severe facial deformity, facial burns, fixed upper airway obstruction and any of the following criteria for imminent intubation and invasive mechanical ventilation (i.e. respiratory or cardiac arrest, diminished consciousness (Glasgow coma score <8), psychomotor agitation inadequately controlled by sedation, massive aspiration, persistent inability to remove respiratory secretions, severe haemodynamic instability unresponsive to fluids and vasoactive drugs, severe ventricular or supraventricular arrhythmias and life threatening hypoxaemia) [1, 6]. Also, COPD patients who have goals of care that do not include mechanical ventilation are not eligible for our study.

{kind=link}
Flow diagram of study protocol. PaCO2: arterial CO2 tension; RR: respiratory rate; VAS: visual analogue scale.
Study groups
There will be two study groups. Patients randomised to study group 1 will receive NIV with the initial setting: expiratory positive airway pressure of 3 cmH2O, inspiratory positive airway pressure of 15 cmH2O, inspiratory to expiratory ratio of 1:2 to 1:3, inspiratory time of 0.8–1.2 s and inspiratory oxygen fraction (FIO2) adjusted to maintain arterial oxygen saturation measured by pulse oximetry (SpO2) between 88–92%, according to the British Thoracic Society/Intensive Care Society guideline for the ventilatory management of acute hypercapnic respiratory failure in adults [6]. Any further changes of expiratory positive airway pressure and inspiratory positive airway pressure will be made according to patient's vital signs/monitoring data and the attending physician's instruction. Study group 2 will receive NHF therapy with the initial setting of flow at 50–60 L·min−1, temperature at 37°C and FIO2adjusted to maintain SpO2 between 88–92% [19]. The NHF device and consumables will be the same in all centres (AIRVO 2, Fisher & Paykel Healthcare Ltd., Auckland, New Zealand). For NIV devices, each site uses its own local and available NIV devices, so they are familiar with their use; however, the therapy delivered by the different NIV devices is comparable.
Study end-points
The primary end-point of the study is the frequency of treatment failure defined as: need for intubation and invasive mechanical ventilation or change to the alternative treatment group. Secondary end-points include: changes in respiratory variables (respiratory rate, arterial blood gases (ABGs), respiratory accessory muscle use), patient's comfort (level of noise, mouth dryness, general perception of tolerance) and any pulmonary and extrapulmonary complications (e.g. pneumothorax, arrhythmia, cardiac infarction).
Data collection and outcome assessment
A case report form for every patient will be recorded. Demographic data including sex, age, weight, height, spirometric measurements (most recent forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), FEV1/FVC ratio obtained from medical notes), reason for hospital admission and any concomitant health problems will be documented. ABG, vital signs (systolic and diastolic arterial pressure, heart rate), respiratory variables (respiratory rate, accessory muscle use, thoracoabdominal asynchrony), dyspnoea score (with the Borg scale) [20, 21] and any pulmonary or extrapulmonary complications will also be assessed. We will also record patient's comfort by assessing the following: machine noise levels, mouth dryness and general perception of tolerance using a visual analogue scale from 0 (no inconvenience due to noise, no dryness, no discomfort) to 10 (maximum inconvenience due to noise, maximum dryness, maximum discomfort) [21, 22].
All measurements (figure 1) will be performed at baseline, before NIV or NHF initiation, and at 1, 2, 4, 6, 12, 24, 48 h then once daily from day 3 to patient discharge, intubation or death. Treatment settings (NIV or NHF) will be recorded for all time points.
At each study point, if the patient feels discomfort and there is deterioration or even no improvement of the examined physiologic variables, NHF or NIV treatment settings will be reviewed and if settings are already optimal, the patient will be changed to the other group. Optimal setting is defined as the ideal setting regulated by the attending physician for each patient. The cut-off values of the examined physiologic parameters are SpO2<88% not corrected with supplemental oxygen, respiratory rate >35 breaths·min−1, thoraco-abdominal asynchrony and auxiliary respiratory muscle use, worsening of hypercapnia and acidaemia, indicating further respiratory muscle fatigue and sequential organ failure assessment score >4 [19]. Patients presenting with or developing respiratory arrest, gasping respiration, pH<7.15, signs of low cardiac output or presence of exclusion criteria (severe facial deformity, facial burns or fixed upper airway obstruction) will be immediately intubated and ventilated. Intubation will be considered for NIV and NHF failure defined as imminent respiratory arrest, severe respiratory distress, persisting pH<7.25 or deterioration in pH despite optimum settings and, depressed consciousness (Glasgow coma score <8) [6].
In patients whose ABG and other respiratory indices have been improved sufficiently, weaning from treatment will begin. For the NIV group, treatment time will be reduced gradually, with increasingly prolonged periods of self-ventilation during the day, with overnight NIV. After patient's clinical status and ABG stabilisation (pH>7.35 and PaCO2<45 mmHg or >45 mmHg with respiratory rate <25 breaths·min−1), NIV will be discontinued [6]. In the NHF group, supplementary oxygen (if supplemental oxygen was required) should be decreased first to FIO2 values <35%, followed by a stepped decrease in flow rate of 5–10 L.min−1. The intervals of these decrements will be based on the patient's above mentioned clinical and physiological parameters. When the patient is stable for 1–2 h with minimal or no supplemental oxygen while SpO2 remains >88–92% and flow rate <15 L·min−1, NHF will be stopped and a Venturi mask or nasal prongs will be provided, if supplementary oxygen is still needed [9, 19, 23].
During the study period, bronchodilator therapy via a nebuliser will be administered during breaks from NIV or via a nebuliser inserted into the ventilator circuit if the patient is dependent on NIV [6]. In the NHF group, aerosols will be administered without interruption of therapy, by placing the nebuliser above the nasal cannula and reducing the flow to 30 L.min−1 for enhanced lung delivery [24].
Statistical analysis
As our primary outcome is binary (i.e. treatment failure or not for two parallel groups), α will be set at 0.05 and β at 0.20 (80% power) for our sample size. For the purpose of the study we will assume that no patient will be lost to follow-up. A failure rate of 20% for NIV and 20–25% for NHF is expected. Given this, the noninferiority margin δ will be set at 5–12%
Noninferiority for NHF will be established if the upper limit of the one-sided 95% confidence interval for the between-group difference in treatment failure rates is <10% with α set at 0.05. Assuming failure rates of 20% in the NIV group and 21% in the NHF group, with a noninferiority limit of 10% with 80% power, 498 participants (249 per group) will be required.
As study power will be reduced considerably if the primary outcome is achieved less often than expected, an interim analysis will be conducted after 200 patients have been enrolled to re-assess the validity of the sample size estimate. This interim analysis will neither assess the difference between the two treatments nor modify the α risk.
Discussion
Over the past decade, NHF therapy has been increasingly utilised for the management of hypoxaemic respiratory failure. The physiological effects of NHF treatment have also been studied in stable chronic COPD patients with the use of NHF showing a reduction in hypercapnia [12, 25, 26] and respiratory rate [12, 25–27] with concomitant improvement in dyspnoea and patients’ quality of life [13, 14]. In a study by Fraser et al. [12], it was suggested that, compared to long-term oxygen therapy, NHF led to higher tidal volume and end-expiratory lung volumes. It seems that NHF therapy can reduce the work of breathing in respiratory compromised patients, leading to more efficient alveolar ventilation and improvement in CO2 levels [11]. When compared to NIV, minute ventilation is lower on NHF treatment, whereas the rapid shallow breathing index is comparable, indicating a reduced respiratory muscle load [12, 27].
Data on NHF use in AECOPD are extremely limited to date. The first published papers, using NHF therapy in hypercapnic AECOPD were cases series, in which NHF was applied as a rescue therapy due to contraindications or intolerance of NIV. Results using NHF, showed complete clinical and laboratory improvements within 4 h [15, 16]. These results were further confirmed by Braunlich et al. [17] in an observational study, including patients with severe-to-moderate acidotic and nonacidotic hypercapnic AECOPD. Again, NHF was implemented if NIV could not be tolerated, and NHF showed significant improvement in pH and PaCO2 within the first hours of its use. In mixed populations with acute hypercapnic respiratory failure, and failure or intolerance of conventional oxygen therapy and NIV, two studies have recorded a reduction of PaCO2 levels and improvement of pH with an associated reduction in respiratory rate while using NHF [28, 29]. Nevertheless, although a significant proportion of the population had AECOPD, the conclusions can only be used as supportive evidence for studies that will be conducted solely with COPD patients.
Currently, the gold-standard ventilatory support device for hypercapnic AECOPD is NIV. However, NIV failure is not unusual among COPD patients, and a large number of them (∼20–30%) present with contraindications to NIV or inability to cooperate with NIV [6, 30], leading to intubation and invasive mechanical ventilation, as soon as there is no established alternative.
To date, there are only two randomised control trials showing noninferiority of NHF to NIV in post-extubated patients. The first, showed noninferiority of NHF to NIV for preventing or resolving acute respiratory failure after cardiothoracic surgery [31], while the other, showed noninferiority in re-intubation rates and post-extubation respiratory failure [32] in patients with high risk for re-intubation. Stephan et al. [31] attributed the results to the positive effects of NHF in reducing PaCO2and to the improvement in respiratory mechanics. On the other hand, Hernandez et al. [32], suggested that the use of NHF led to the reduction in hypoxaemia and work of breathing, while improving airway secretions and reducing the episodes of upper airway obstruction. Lee et al. [33], in a prospective observational trial comparing the effectiveness between NHF and NIV in severe AECOPD with moderate hypercapnic acute respiratory failure showed no statistically significant difference regarding the 30-day mortality and intubation rate.
So far, this is the only prospective study in patients with hypercapnic AECOPD. The study we are conducting is a multicentred unblinded randomised controlled trial. Our null hypothesis is that NHF will be inferior to NIV in patients with AECOPD and mild-to-moderate acute or acute on chronic hypercapnic respiratory failure. Our alternate hypothesis is that NHF will be noninferior to NIV in these patients. If we were able to reject our null and accept our alternate hypothesis, NHF could possibly serve as an effective alternative respiratory support device for patients with AECOPD and mild-to-moderate hypercapnic respiratory failure, especially in those who have contraindications to or cannot tolerate NIV.
There are some limitations of our trial. First, although the centres that participate in the study are highly equipped and educated in NIV and NHF therapy, there is likely to be differences in clinical practice that affect the interventions. We will address this on an intention-to-treat and a per-protocol basis in the statistical analysis. Second, nebulisation during NHF is still under investigation and it is possible that different positioning of the nebuliser may affect the outcome of the study [34]. Réminiac et al. [24], and Dailey et al. [35] found that in vitro, there was greater aerosol deposition at flow rates of 30 L.min−1 to 50–60 L.min−1 during distressed breathing in contrast to quiet breathing. In a further study, Réminiac et al. [36] showed that NHF itself produced a bronchodilation effect, thus suggesting that the underlying mechanism may be the positive airway pressure recruiting alveoli in the atelectatic areas and changes generated within the respiratory pattern, potentially leading to higher tidal volume and ultimately slower inspiration. It is worth noting that, while these studies are conducted in bench-models, the position of nebuliser has a significant impact on aerosol dose delivery. Nevertheless, it appears that in clinical studies, different positions do not impact as significantly on clinical outcomes. This could be explained by the existence of other factors that may be present during spontaneous breathing, such as the breathing pattern, inspiratory flow and respiratory rate and any potential leaks that could reduce the aerosol deposition [37, 38]. Finally, due to the study design, blindness is not possible. However, this study intent to become the largest prospective randomised trial looking at noninferiority of NHF versus NIV in hypercapnic AECOPD and its results is expected to have a significant impact in the management of these patients.
Footnotes
This study is registered at www.clinicaltrials.gov with identifier number NCT03466385. Data that are planned to be shared are the study protocol, statistical analysis and clinical study report. They will be shared 3 months after study publication with anyone who is interested in writing a meta-analysis or review.
Trial status: The study is currently recruiting. The first patient was enrolled in November 2018. Recruitment is expected to be completed by 31 December, 2021.
Conflict of interest: A. Papalampidou reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: E. Bibaki reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: S. Boutlas reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: I. Pantazopoulos reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: N. Athanasiou reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: M. Moylan has nothing to disclose.
Conflict of interest: V. Vlachakos reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: V. Grigoropoulos reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: K. Eleftheriou reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: Z. Daniil reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: K. Gourgoulianis reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: L. Kalomenidis reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: S. Zakynthinos reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Conflict of interest: E. Ischaki reports nonfinancial support from Fisher & Paykel in the form of devices and consumables during the conduct of the study.
Support statement: All authors would like to acknowledge the support of the Special Account for Research Grants of the National and Kapodistrian University of Athens, Greece.
- Received March 4, 2020.
- Accepted August 10, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










