





Abstract
Introduction The present study assessed the prevalence of nine treatable traits (TTs) pinpointing nonpharmacological interventions in patients with COPD upon first referral to a pulmonologist, how these TTs co-occurred and whether and to what extent the TTs increased the odds having a severely impaired health status.
Methods Data were collected from a sample of 402 COPD patients. A second sample of 381 patients with COPD was used for validation. Nine TTs were assessed: current smoking status, activity-related dyspnoea, frequent exacerbations <12 months, severe fatigue, depressed mood, poor physical capacity, low physical activity, poor nutritional status and a low level of self-management activation. For each TT the odds ratio (OR) of having a severe health status impairment was calculated. Furthermore, a graphic representation was created, the COPD sTRAITosphere, to visualise TTs prevalence and OR.
Results On average 3.9±2.0 TTs per patient were observed. These TTs occurred relatively independently of each other and coexisted in 151 unique combinations. A significant positive correlation was found between the number of TTs and Clinical COPD Questionnaire total score (r=0.58; p<0.001). Patients with severe fatigue (OR: 8.8), severe activity-related dyspnoea (OR: 5.8) or depressed mood (OR: 4.2) had the highest likelihood of having a severely impaired health status. The validation sample corroborated these findings.
Conclusions Upon first referral to a pulmonologist, COPD patients show multiple TTs indicating them to several nonpharmacological interventions. These TTs coexist in many different combinations, are relatively independent and increase the likelihood of having a severely impaired health status.
Abstract
Patients with COPD show numerous nonpharmacological treatable traits (TTs) upon referral to a pulmonologist. These TTs coexist in many different combinations, are relatively independent and increase the likelihood of a severely impaired health status. https://bit.ly/355mhpj
Introduction
COPD is a highly prevalent and complex disease, with an extraordinary heterogeneity in its clinical presentation [1]. While COPD is defined by the presence of an incomplete reversible airflow limitation, numerous intra- and extrapulmonary manifestations have been identified, which may be variably and/or transiently present, all adding up to the individual burden of disease [2]. Therefore, a personalised approach is advocated [3]. Hence, relevant and modifiable pulmonary, extrapulmonary and behavioural/lifestyle features, the so-called treatable traits (TTs), need to be identified through a comprehensive assessment and subsequently be addressed in a patient-centred management plan [4]. This comprehensive assessment must go beyond lung function measurements as relevant extrapulmonary and behavioural TTs cannot be captured solely with pulmonary function testing [5]. A broad assessment of TTs is common at the start of a comprehensive pulmonary rehabilitation program but is certainly not standard in primary and secondary-care work settings [6]. Regrettably, pulmonary rehabilitation is still markedly under-utilised as a potent nonpharmacological intervention option and often considered only late in the patient's disease career [7, 8]. Moreover, a considerable proportion of patients with COPD, who are cared for by the general practitioner (GP) and/or pulmonologist show evidence of physical, emotional and/or social TTs, that require nonpharmacological interventions beyond respiratory drug treatment, even when they are just in a mild stage of disease [9, 10].
In the Netherlands, GPs are the gatekeepers of the care system [11]. Therefore, COPD is primarily diagnosed by GPs and then treated according to the national guideline. According to the Dutch Standard of Care, patients with COPD can be referred to a pulmonologist for a hospital-based outpatient consultation if the treatment response in primary care is unsatisfactory and their burden of disease persists [12]. Such an outpatient consultation follows international recommendations and is usually limited to taking patients medical history, physical examination, biomedical assessments, such as pulmonary function, blood testing, pulmonary imaging, and, simple questionnaires to assess symptom burden [13]. However, although GPs and pulmonologists do have a clear understanding of what the content and methodology of a comprehensive outpatient hospital-based assessment should comprise, they generally do not measure TTs beyond lung function [14, 15]. Aims of the present study were to assess in patients with COPD upon first referral to a pulmonologist: the prevalence of nine potentially clinically relevant TTs pinpointing nonpharmacological interventions, the combinations in which they occur and whether the presence of multiple TTs increases the odds having a severely impaired health status. We hypothesised that patients with COPD upon first referral to a pulmonologist would have multiple TTs indicative for nonpharmacological interventions, that these TTs arise in different combinations, and that their presence would increase the odds of having a severely impaired health status.
Material and methods
Study participants
All patients with a confirmed diagnosis of COPD, with a first-time referral between October 2014 and December 2018 to the outpatient respiratory department of Radboudumc, Nijmegen and Bernhoven Hospital, Uden, both in the Netherlands, were deemed eligible for participation providing they had been free of an acute exacerbation for ≥3 months. The Research Ethics Committee of the Radboud University Medical Centre approved the study. Due to the observational nature of the study and the provision of usual care, written informed consent was waived (ref: 2017/3597).
Study design
This is a multicentre, ambispective, observational study. In the prospective study, upon referral by a GP, patients were assessed in a standardised comprehensive diagnostic care pathway to identify the presence of TTs indicative for nonpharmacological interventions [15, 16]. These nine TTs were selected because evidence-based interventions exist for them. Table 1 provides an overview of the examined nine TTs, the measurement instruments used, the applied cut-off values and appropriate evidence-based possible interventions. To quantify patients' health status, the Clinical COPD Questionnaire (CCQ) was used [31]. The CCQ has been accepted as valid and reliable questionnaire to measure health status in clinical practice in COPD patients [32], and, has been endorsed also as short but comprehensive disease-specific health status questionnaire for the ABCD assessment tool used in the GOLD document [13]. Additional details on the content of the diagnostic care pathway is provided in the online data supplement.
Examined treatable traits, measurement instruments, cut-off values applied and appropriate evidence-based nonpharmacological interventions
Analyses
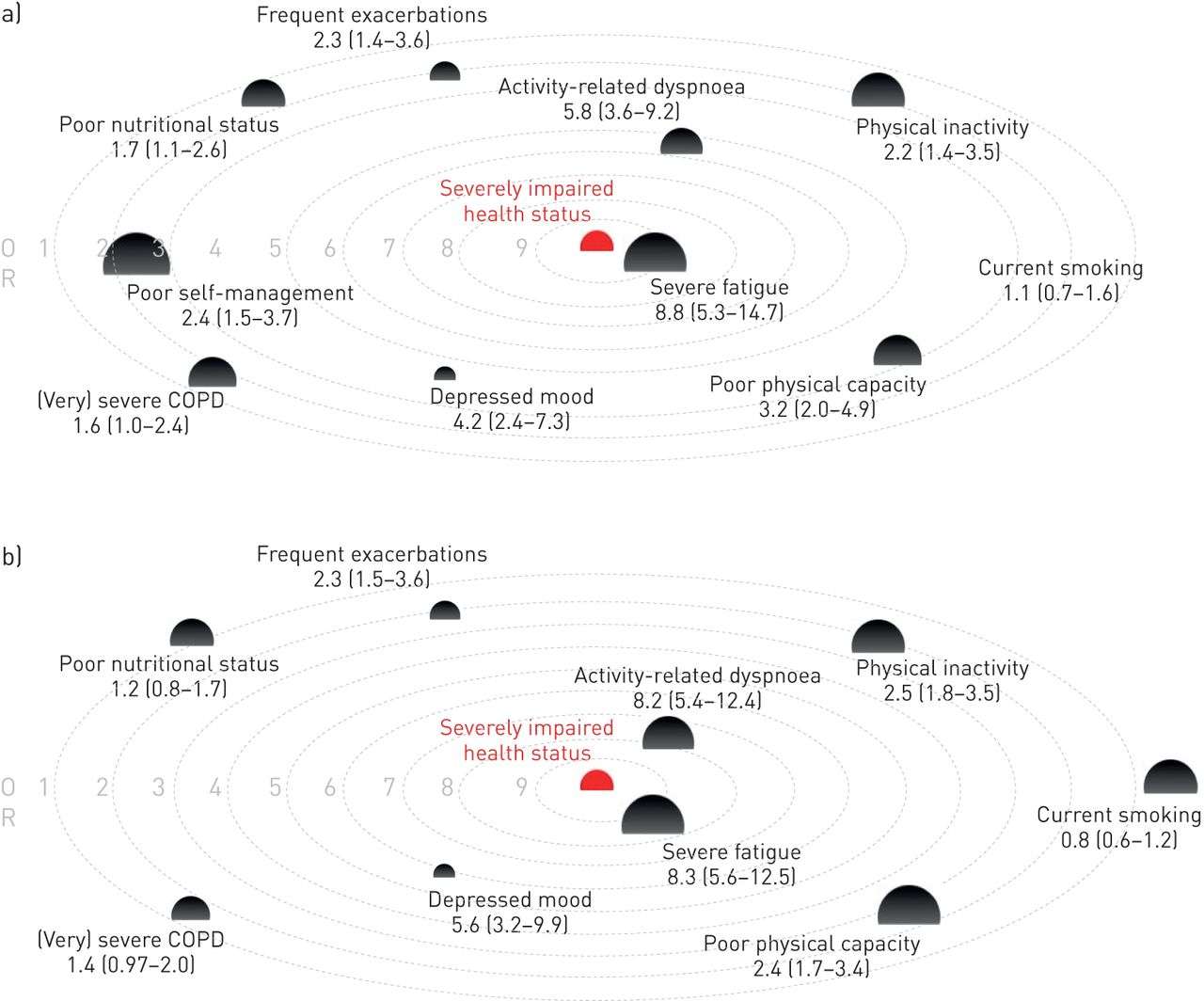
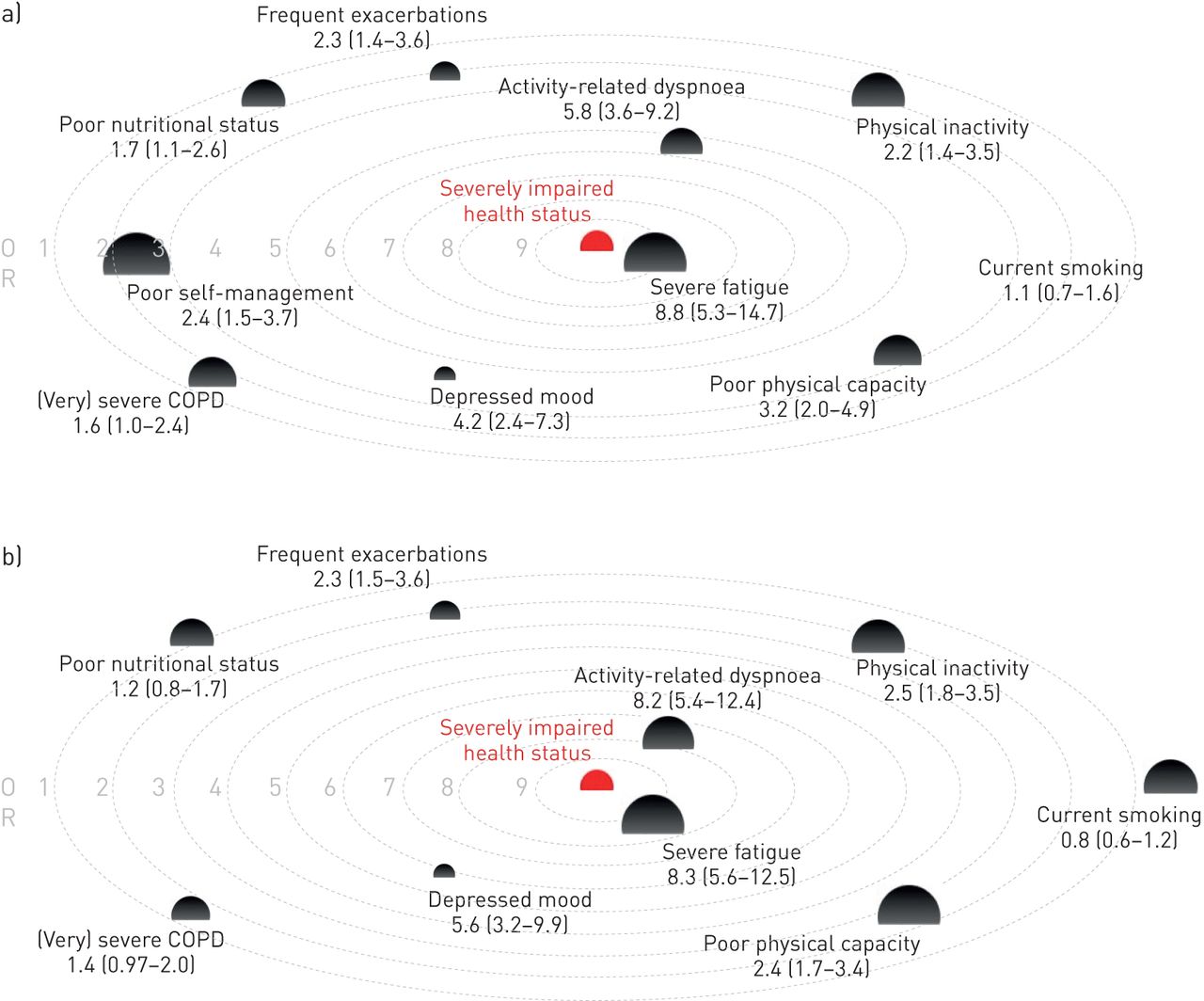
Inspired by Divo et al. [33] who developed the COPD ‘comorbidome’, we created the COPD ‘sTRAITosphere’. This is a graphical presentation of the combination of the prevalence of each TT (depicted with the size), and the TT's ORs of having a severe health status impairment (CCQ total score >2.0 points). The combined presentation allows to read the clinical relevance of each TT at a glance. Data from a retrospective study on a convenient second sample of 584 patients with COPD were used to validate the initial COPD sTRAITosphere. These were also all patients referred for the first time to the outpatient respiratory department of Amphia Hospital, Breda, the Netherlands, consecutively between April 2013 and December 2018, and free of an acute exacerbation ≥3 months. In this independent sample, except activation for self-management, all other eight TTs were assessed using the exact same methodology as in the primary sample.
Statistical methods
Descriptive statistics were used to summarise the data as means (sd), medians (ranges) or frequencies (proportions), as appropriate. The presence of the nine TTs was dichotomously determined in each participating patient. Subsequently, the prevalence of each TT was determined by calculating the percentage of patients who met the pre-defined criteria (table 1). With nine TTs a maximum number of 512 (29) unique combinations is possible. An individual sum score was calculated in patients with a valid registration of all nine TTs. The association between the nine TTs was assessed using Pearson's correlation coefficients. With nine TTs, this produces up to 36 ((92–9)×0.5) unique correlation coefficients. In these patients, the association between individual TT sum scores and FEV1 % predicted as well as CCQ total score were also assessed using Pearson's correlation coefficients. Moreover, TT sum scores were related to the CCQ impairment classification, that is, mild impairment (CCQ total score 0–1 point), moderate impairment (1–2 points), severe impairment (2–3 points), or very severe impairment >3 points, applying one-way ANOVA. To further elicit the clinical relevance of the number of TTs for health status, linear regression analysis was performed with CCQ total as response variable and FEV1 % predicted or the total number of TTs as explanatory variables. Logistic regression assessed the OR of having a severely impaired health status (CCQ total score >2 points) per TT and for (very) severe degree of airflow limitation (GOLD III/IV). Both regression analyses were checked for possible confounding by age and sex and the results were corrected where this was the case. All statistical analyses were conducted using SPSS version 22 (IBM Corp., Armonk, NY, USA). Significance levels were set to p<0.05.
Results
Patient characteristics
In total, 402 patients were included. General and COPD-specific patient characteristics including measures reflecting the burden of disease are summarised in table 2. More patients (48%) had a moderate airway obstruction, closely followed (36%) by severe obstruction, severe hypoxaemia was present in 16%, and a median of two comorbidities was found. The vast majority (80%) of the patients was symptomatic (GOLD group B or D). In the year preceding referral to secondary care, 109 patients (27%) had been referred to an allied healthcare professional, of which physiotherapy was the most frequent (83 cases; 20%).
General and COPD-specific patient characteristics
Prevalence of TTs
Prevalence of the nine examined TTs is shown in figure 1. The top-three TTs consists of severe fatigue, poor activation for self-management and low habitual physical activity. From 279 patients (70%), data points on all nine TTs were available. Of these, figure 2 shows the distribution of the 151 unique combinations of TTs (figure 2a), the frequencies of the number of TTs present per patient (figure 2b), a scatter-plot of CCQ total score against the number of TTs present per patient (figure 2c) and a scatter-plot of FEV1 % predicted against the number of TTs present per patient (figure 2d). A mean of 3.9±2.0 TTs per patient was observed. A significant correlation coefficient was found between 21 (58%) of the TTs. However, the vast majority (44%) correlated only weakly (range 0.11–0.28). Another 14% correlated moderately (range 0.32–0.53). Strong correlations did not appear. In table E1 of the online data supplement, the correlation matrix of the TTs is provided. Of the 151 unique TTs combinations, 91 (60%) occurred only once, 30 (20%) twice (60 patients), 14 (9%) three times (42 patients), eight (5%) four times (32 patients), four (3%) five times (20 patients), two (1%) eight times (16 patients), one (<1%) seven times (7 patients), and, one (<1%) occurred 11 times (11 patients). Figure 2 shows the heterogeneity in the number and combinations of the nine TTs.

Frequencies of the nine treatable traits. SM: self-management.

Total number of treatable traits (TTs). a) 151 unique combinations of TTs are illustrated in relation to the total number of TTs per patient. Red represents the presence of a particular TT whereas green represents the absence. The blue lines mark the subgroups with a corresponding total number of TTs. b) Frequencies of the number of TTs present per patient displayed. c) and d) A scatter-plot is presented of the total number of TTs and the Clinical COPD Questionnaire (CCQ) total score (c) and forced expiratory volume in 1 s (FEV1) % predicted (d), respectively. SM: self-management.
TTs and health status
The relationship between number of TTs and impaired health status and FEV1 % predicted is graphically presented in the two upper panels of figure 2. Significant correlation coefficients were found between the total number of TTs and FEV1 % predicted (r=−0.29; p<0.001) and CCQ total score (r=0.58; p<0.001). Linear regression analysis produced the following regression equation: CCQ total score=0.765+0.298×number of TTs (p<0.001). Correlation between CCQ total score and FEV1 % predicted amounted to only −0.19 (p<0.001). Regression analyses did not appear to require adjustment for age and sex. Mean total number of TTs summed up to 2.4±1.2, 3.4±1.6, 4.6±1.6 and 5.5±1.7 in patients with COPD with mild, moderate, severe or very severely impaired health status, respectively and differed significantly (p<0.001) between all four stages. In figure 3a the COPD sTRAITosphere is presented. A severely impaired health status is at the very centre of the sTRAITosphere and each TT and FEV1 % predicted is presented as sphere. The size of the spheres is proportional to the prevalence of the TT and the distance to the centre reflects the OR of having a severely impaired health status. The closer the TT is to the centre, the higher the likelihood of having a severely impaired health status.
{kind=link}
{kind=link}
{kind=link}
a) The COPD sTRAITosphere. A severely impaired health status (Clinical COPD Questionnaire (CCQ) total score >2 points) is at the very centre of the sTRAITosphere and each treatable trait (TT) is presented as sphere. The size of the spheres is proportional to the prevalence of the TT and the distance to the centre reflects the OR of having a severely impaired health status. b) Validation of the COPD sTRAITosphere.
Validation sample
Data points on all eight TTs were available from 381 patients (65%) of the Amphia validation sample and were used to validate the COPD sTRAITosphere. The patient activation measure (PAM) was not measured in the validation sample. The validation sample had similar characteristics compared to the initial COPD sample. In an online data supplement, general and COPD-specific patient characteristics of the validation sample (table E2), the prevalence of the eight TTs (supplementary figure E1), and the frequencies of the number of TTs present per patient (supplementary figure E2) are provided. Again, patients with a depressed mood (OR: 5.6 (3.2; 9.9)), activity-related dyspnoea (OR: 8.2 (5.4; 12.4)), or severe fatigue (OR: 8.3 (5.6; 12.5)) had the highest likelihood for having a severely impaired health status (figure 3b).
Discussion
The present study setting out to determine the prevalence of nine TTs, indicating nonpharmacological interventions of patients with COPD, with a first-time referral to an outpatient respiratory clinic shows three important findings. Firstly, patients exhibited on average four out of nine TTs qualifying for nonpharmacological treatment options. Secondly, the observed TTs appeared to be relatively independent of each other and emerged mostly in unique combinations, confirming the well-known phenotypical heterogeneity from the TTs perspective. Thirdly, the clinical relevance of the TTs was confirmed because a significant positive association was found between the number of TTs and the impaired health status, and, except for smoking status all individual TTs increased the likelihood of having a severely impaired health status. Combining these findings suggests that the TTs examined in this study form a window of opportunity to ease symptoms and to better daily functioning of highly symptomatic patients with COPD. Moreover, a reduction of ≥1 TTs may already result in a clinically relevant improvement in health status.
Health status impairment
Overall, 80% of the patients in the current study were highly symptomatic, which indeed justifies a referral by the GP to an outpatient consultation of the pulmonologist [34]. About 80% of the patients referred to secondary care had a significant COPD-related impaired daily functioning of whom nearly half was severely to very severely impaired, 44% of the patients were still smoking and 16% even presented with severe hypoxaemia, indicating them for long-term oxygen therapy. This shows that patients were referred late in their disease career to specialised respiratory care. It can be argued that the high impact on health status might have been (partially) prevented should these TTs have been addressed earlier. Another 10% of the referred patients were hardly symptomatic and were classified as GOLD A, which raises the question why these patients had been referred to a pulmonologist anyway. A plausible explanation for this is that there might have been doubts about the diagnosis by the GP and the reason for referral was to get a proper pulmonary diagnosis and/or to get clues and assistance with a view on improving the patient's health status. Indeed, setting the right diagnosis of COPD still seems difficult in primary care [35]. Empowering GPs in diagnosing COPD by ongoing training in interpreting spirometry might be a first solution here [36], and/or implementing remote quality control systems [37]. Incidentally, this study shows that patients with only a GOLD class A do not exclude the presence of clinically relevant TTs. Only 22% had no TT, 23% had one, 20% had two and 35% had ≥3 TTs.
The number and clinical relevance of TTs
To our knowledge, this is the first study reporting on the large prevalence and relative independency of TTs in patient referred for hospital-based outpatient consultation, which occurred mostly in unique combinations. Indeed, 60% of the identified 151 combinations of TTs occurred only once and the correlation between the number of TTs and FEV1 % predicted was poor. This TT approach nicely illustrates the known complexity and heterogeneity beyond the degree of airflow limitation [2]. This indicates the importance and opportunity to improve patients' health status should these TTs adequately be addressed in the clinical management. Results of the COPD sTRAITosphere suggests that fatigue, activity-related dyspnoea and depressed mood are the most outstanding TTs to better health status as patients with these TTs had the highest likelihood of having a severely impaired health status. These findings were confirmed in a second, independent sample of patients with COPD. With a mean of four TTs per patient and given that the minimal clinically important difference of the CCQ total score is between −0.5 and −0.3 points, it can be estimated from the regression equation that a clinically relevant improvement in health status can be obtained already when only one TT improves following treatment [38]. Indeed, positive effects of such an approach have been shown in a proof-of-concept study in COPD [39] and very recently also in patients with asthma [40]. The current findings emphasise the need for a comprehensive assessment in each individual patient with COPD early in the disease career, and, subsequently, a personalised COPD management program, including pharmacological and nonpharmacological treatment options. Such a comprehensive assessment is feasible to implement and does not require highly demanding recourses [16]. Seven out of nine TTs assessed in the present study can be appraised through readily available and validated questionnaires, which, these days, can be administered relatively easily and processed digitally. Only the assessment of physical capacity and physical activity requires additional efforts. Clinical decision making based on the presence or absence of a particular TT can be dichotomously determined by applying available validated cut-off values. With regard to choices about exercise-based interventions, the recently introduced Dutch model for profiling patients with COPD for adequate referral to exercise-based care is available [41].
Methodological considerations
Large observational studies such as ECLIPSE [42] and others [43], did provide important data on the complexity and heterogeneity of patients with COPD. However, these studies have used stringent inclusion criteria apparently limiting the generalizability of the findings of these studies [44]. The present observational clinical study specifically aimed to assess the presence TTs in nonselected COPD patients indicative for nonpharmacological interventions alongside drug therapy, who were referred for a routine outpatient consultation. The number of examined TTs in this study is certainly not inexhaustible. Other traits, deemed important, may also be relevant to consider in the phenotyping of patients with COPD [45]. We have chosen deliberately to use this set of TTs because for each of these TTs, evidence-based nonpharmacological interventions are available (table 1, last column) and because they are relatively easily to capture in a clinical routine. Obviously, the cross-sectional study design precludes a longitudinal follow-up of the TTs. However, TTs fluctuate over time, while the degree of airflow limitation may remain stable. For example, Peters et al. [46] showed that the proportion of COPD patients with severe fatigue doubled during 4 years of usual care, while the FEV1 % predicted remained stable.
Conclusions
Patients with COPD show a markedly impaired health status upon referral to a pulmonologist and present numerous TTs indicating them to nonpharmacological interventions. These TTs co-occur in various unique combinations, are relatively independent and increase the likelihood of having a severely impaired health status. Findings of this study stress the need for a comprehensive assessment and addressing these TTs early in personalised clinical management.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00438-2020.SUPPLEMENT
Figure E1 00438-2020.FigureE1
{kind=link}
FIgure E2 00438-2020.FIgureE2
{kind=link}
Acknowledgements
We would like to express our gratitude to all pulmonologists, respiratory nurses, pulmonary function technicians and workers of the clinometric department from both Bernhoven and Radboudumc who contributed to the collection of data for this study and for the interesting discussions we had during the process of explaining the results.
Footnotes
This article has supplementary material available from openres.ersjournals.com
Conflict of interest: A.J. van 't Hul has nothing to disclose.
Conflict of interest: E.H. Koolen has nothing to disclose.
Conflict of interest: J.C. Antons has nothing to disclose.
Conflict of interest: M. de Man has nothing to disclose.
Conflict of interest: R.S. Djamin has nothing to disclose.
Conflict of interest: J.C.C.M. in 't Veen reports grants from Boehringer Ingelheim, Teva, Chiesi and Sanofi outside the submitted work.
Conflict of interest: S.O. Simons has nothing to disclose.
Conflict of interest: M. van den Heuvel has nothing to disclose.
Conflict of interest: B. van den Borst has nothing to disclose.
Conflict of interest: M.A. Spruit reports grants from the Netherlands Lung Foundation and Stichting Astma Bestrijding, and grants and personal fees from AstraZeneca and Boehringer Ingelheim, outside the submitted work.
- Received June 26, 2020.
- Accepted August 26, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










