





Abstract
α1-antitrypsin deficiency (AATD) is a rare and under-recognised genetic condition. Owing to its low prevalence, international initiatives are key for conducting high-quality research in the field.
From July 2018 to December 2019, the European Alpha-1 Research Collaboration (EARCO) developed and conducted two surveys, one for healthcare providers and one for patients and caregivers, aiming to identify research priorities and barriers in access to treatment for AATD.
A survey on 164 research questions was electronically sent to 230 AATD experts in Europe, and 94 completed surveys from 24 countries were received. The top research areas identified by healthcare providers were causes of variable progression and poor outcomes, improvement in diagnosis, initiation and optimal dosing of augmentation therapy and effectiveness of self-management interventions. During the same period, 438 surveys were completed by patients and caregivers from 26 countries. The top research areas identified were improving knowledge about AATD, in particular among general practitioners, access to AATD specialised centres and access to reliable, easy to understand information about living with AATD. Regarding barriers to treatment, participants from countries where augmentation therapy was reimbursed prioritised improving knowledge in AATD, while respondents in non-reimbursed countries regarded access to AATD augmentation therapy and to specialised centres as the most relevant.
The main research and management priorities identified by healthcare providers and patients included understanding the natural history of AATD, improving information to physicians, improving access to specialised reference centres, personalising treatment and having equal opportunities for access to existing therapies.
Abstract
Surveys for patients and healthcare providers on research priorities in AATD, developed by the @EuroRespSoc CRC EARCO, show that international collaboration and engagement with patients are key development strategies needed for improvement https://bit.ly/2ItIzaW
Introduction
α1-antitrypsin deficiency (AATD) is an under-recognised genetic condition that affects ∼1 in 2000 to 1 in 5000 individuals and predisposes to early-onset emphysema and liver disease [1]. Owing to its low prevalence, AATD is considered a rare disease. Because of the variety in its clinical manifestation, many patients may remain undiagnosed until they develop a severe respiratory or liver disease.
A recent statement on AATD by the European Respiratory Society (ERS) [2] recommended organising the care of patients in reference centres because of the low prevalence of the disease. Reference centres must establish a registry of their activity that enables them to share data concerning the clinical characteristics and natural history of patients, nationally and internationally. In this context, the European Alpha-1 Research Collaboration (EARCO) was created in 2018 [3] as a Clinical Research Collaboration (CRC) of the ERS [4], composed of an international group of experienced and new researchers in the field of AATD committed to promoting research in different aspects of the disease: epidemiology, genetics, physiopathology, clinical management and prognosis of lung disease. The ultimate goal is to improve the quality of life of patients with AATD.
One of the initial objectives of EARCO was to build a network of patients' representatives, researchers and clinical investigators to identify research needs and establish an agenda for AATD research [3]. The involvement of patients' representatives and organisations is essential to conduct patient-centred quality research. To reach this goal, a task force of EARCO developed and conducted two surveys, one for healthcare providers and the second for patients and caregivers to better understand the key research needs and barriers to management in the field of AATD. In this report we present the development, results and implications of these surveys, which will guide the future research of EARCO.
Method
A working group comprising six EARCO members (four respirologists and two patient representatives) from five European countries and representatives of the European Lung Foundation (ELF) was established to develop two surveys: one for healthcare providers and another for patients and caregivers (figure 1).

Development of surveys for healthcare providers (HCPs) and patients and caregivers by the European Alpha-1 Research Collaboration (EARCO) survey working group. ERS: European Respiratory Society; ELF: European Lung Foundation.
Healthcare providers' survey
From June to August 2018 the working group analysed the research needs indicated in the recent ERS statement on lung disease in AATD (table 1) [2] and systematically evaluated the literature published after this statement to identify potential new areas of research. After this revision, 180 research questions were drafted and sent to an advisory group formed by five EARCO members for a final check. A final list of 164 research questions was defined, divided into eight research categories (epidemiology and natural course of the disease (n=25); diagnostic and screening (n=16); awareness and education for healthcare providers and for patients and registries (n=13); clinical manifestations (n=23); outcomes and monitoring (n=38); augmentation therapy (n=23); other treatments/AATD therapies (n=8); other non-pharmacological interventions (n=18)). From March 29 to May 1, 2019, an online survey was sent to AATD experts around Europe who were asked to grade each research question anonymously using a five-point scale (1=unimportant to 5=very important). Time for completion of the survey was estimated to be 20–30 min. The complete survey is shown in supplementary material S1.
Research priorities identified by the European Respiratory Society task force on pulmonary disease in AATD [2]
Patients’ survey
During the same period, a survey for patients and caregivers was developed. The survey was designed by the same working group of members of EARCO, including patient representatives and representatives of the ELF. The draft was reviewed by an advisory group of four expert patients with AATD from four European countries, and revised to ensure that it met the needs of the project and would be relevant, interesting and accessible for patients and caregivers.
The survey was provided in nine languages: English, Dutch, French, German, Italian, Polish, Portuguese, Serbian and Spanish. The survey was online for 6 weeks from November 2018 to January 2019 and promoted through the networks and social media of Alpha-1 Global, Alpha-1 patient organisations and groups, ELF, ERS and members of the CRC.
After collecting demographic data from the participants, the survey was divided into two parts: A) questions about the most challenging aspects of managing the disease and barriers to treatment and B) research needs. For part A, patients and caregivers were asked to rate the challenges and barriers using a four-point scale (1=very difficult, 2=difficult, 3=not very difficult, 4=not an issue). For part B, research need questions were divided into six categories: symptoms and burden of the disease, areas of research, diagnosis and awareness of the disease, treatment, treatment burden, and self-management and education. Participants were asked to rate each research priority question by order of importance (unimportant, not very important, important, very important, no opinion). Data are presented as the percentage of responders that rated each item as either important or very important. The complete survey is presented in supplementary material S2.
Statistical analysis
Because the survey was exploratory and there was no a priori hypothesis, no contrasts of hypothesis were performed. Data are presented as descriptive statistics only with mean values or percentages, when appropriate.
Results
Healthcare providers’ survey
The survey was sent electronically to 230 AATD experts in Europe and we received 94 complete surveys (response rate 41%) from 24 countries. The majority (76.6%) of the participants in the healthcare providers' survey were aged between 40 and 60 years old. Most responders (58.5%) had 5–20 years’ experience in following and treating patients with AATD, while 71% visited more than five patients with severe deficiency per year. Most of the responders (92.6%) were pulmonologists.
Table 2 shows the 20 highest-rated research priorities. The top five areas identified by healthcare providers were causes of variable progression and poor outcomes (mean score 4.6 out of 5), improvement of early and accurate diagnosis (4.52), initiation of augmentation therapy (4.51), effectiveness of self-management interventions (4.49) and optimal dose regimen for augmentation therapy (4.38). Other questions considered relevant addressed the definition of a fast decliner, severity and impact of exacerbations and improvement in awareness. The complete list of responses is shown in supplementary material S3.
Most-rated research questions by respiratory specialists
Patients, family members and caregivers’ survey
Characteristics of respondents
A total of 438 surveys from 26 countries were completed. 84% of respondent were individuals diagnosed with AATD and 16% were parents, relatives or caregivers. Among the individuals diagnosed with AATD, 70% had the PI*ZZ genotype. More than half of respondents were diagnosed by a respiratory specialist (56%), with the most likely cause for diagnosis being chronic obstructive pulmonary disease (COPD) (32%), followed by family testing (17%). Almost two thirds of respondents were former smokers (62%) (table 3).
Patients’ demographics and clinical characteristics
Among the survey responses, 124 (28%) were from people living in one of the countries where augmentation therapy is not currently reimbursed (Australia, Denmark, Finland, Ireland, Norway, Sweden and the UK) and 239 (55%) from people living in countries where augmentation is reimbursed (Argentina, Austria, France, Germany, Italy, Portugal, Spain, Switzerland and the USA). 75 surveys (17%) were from respondents from countries where reimbursement was only partial or had an unclear status. The characteristics of the respondents were similar in both groups (table 3).
Most challenging aspects to manage and barriers for treatment
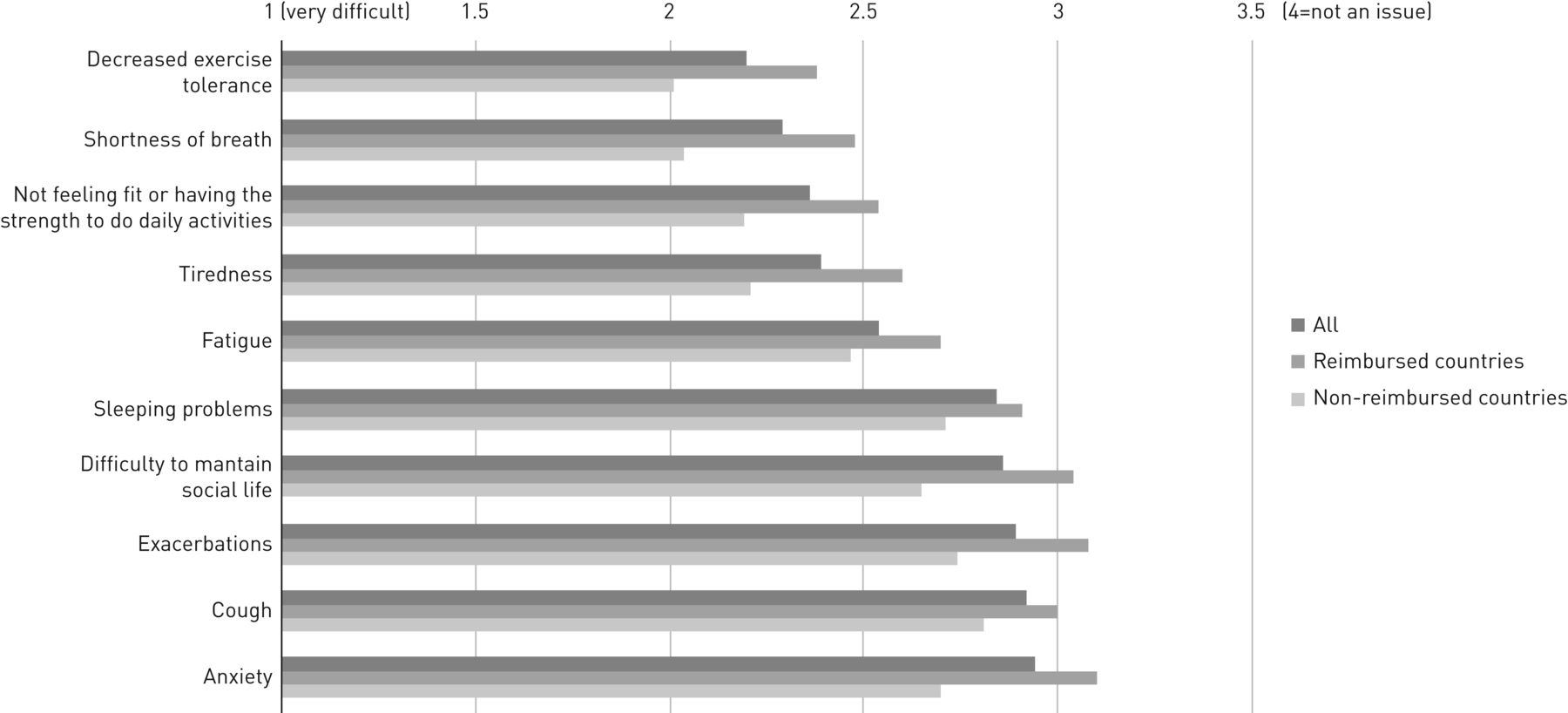
Figure 2 shows the aspects of the disease considered most challenging by patients and caregivers. Decreased exercise tolerance and shortness of breath were the most difficult aspects identified by patients, followed by not feeling fit or having the strength to do daily activities, tiredness and fatigue.

Most challenging aspects to manage for patients. The scale used is 1=very difficult, 2=difficult, 3=not very difficult, 4=not an issue.
Among the most challenging aspects/barriers for treatment, the three considered most important were access issues to augmentation therapy, professional implications of the diagnosis of AATD and access to maintenance classes or using fitness centres after rehabilitation for regular exercise (figure 3).

{kind=link}
{kind=link}
{kind=link}
Most challenging aspects/barriers for treatment. The scale used is 1=very difficult, 2=difficult, 3=not very difficult, 4=not an issue.
There were important differences between reimbursed and non-reimbursed countries. Respondents in non-reimbursed countries identified all aspects related to augmentation therapy as the most challenging barriers for treatment: access issues to augmentation therapy in their healthcare system, hospital administration of augmentation therapy and time consumed in augmentation therapy. By contrast, individuals in reimbursed countries identified access to maintenance classes or fitness centres to maintain fitness after rehabilitation, access to pulmonary rehabilitation and the impact of transplant on patients and their families as the most challenging barriers (figure 3).
Research prioritisation by patients and caregivers
Almost all respondents (99%) considered improving knowledge of AATD to be a priority, in particular in general practitioners (GPs). Other top research areas identified were access to AATD specialised centres (97%), access to reliable, easy to understand information about living with AATD (97%), being able to recognise an exacerbation (97%), targeted screening programmes for COPD and asthma patients (96%), and having an action plan for exacerbations and easy access to healthcare during episodes (96%) (table 4). The complete survey results by section are shown in supplementary material S4.
Most important research areas as rated by patients and caregivers
Differences in research prioritisation between countries according to reimbursement of therapy
Top research priorities identified by respondents in reimbursed and non-reimbursed countries are shown in table 4. For both groups, top research priorities included more evidence on effectiveness of augmentation therapy, education for physicians on diagnostic techniques, algorithms for treatment and interpretation of results, and improving knowledge of AATD in particular among GPs. Respondents in non-reimbursed countries considered access to AATD specialised centres and to reliable, easy to understand information about AATD a priority, as well as having an action plan for exacerbations. For individuals in reimbursed countries, a personalised integrated care plan including physical activity, targeted screening programmes for COPD and asthma patients, and being able to recognise an exacerbation were also relevant, among others. Research on alternatives to intravenous augmentation therapy was also considered relevant for these participants. The complete survey results by type of country are shown in supplementary material S5.
Discussion
International collaboration is crucial to develop strategies for improving patient care and research in the field of rare diseases. Although research in AATD has been conducted for more than 50 years [5], there are still several areas of uncertainty. This is a result of the limited number of patients affected by the disease, which is a hurdle for large epidemiological studies [6] or sufficiently powered clinical trials [7], and the reduced investment in research into rare diseases generally. These two challenges provide motivation to join forces and direct research to the aspects that are considered more relevant by researchers and, more importantly, by the patients themselves.
In this context, the ERS endorsed the creation of EARCO [3, 4], aimed at establishing a collaborative effort to advance understanding through research and to improve the quality of life of patients with the disease. The first objective of EARCO was to design and implement a prospective, international registry of patients with AATD to better understand the natural history of the disease and to investigate the impact of different therapies, including augmentation therapy, on the disease course [8]. This registry is already open and recruiting (information available at www.earco.eu/registry). Beyond the registry, or in addition to it, EARCO wants to establish a research agenda for AATD; to develop this agenda, a working group designed and conducted the current survey of unmet needs and challenging aspects to management and research in AATD for healthcare providers and patients.
Healthcare providers’ research priorities
The main research priorities that healthcare providers focused on was understanding the evolution of the disease and the risk factors for poor outcomes and, consequently, identifying the best candidates, the best regimens and the right time to initiate augmentation therapy. The first prospective studies of cohorts of AATD patients indicated the large variability in rates of lung function decline, in particular between index and non-index cases and between smokers and never-smokers [9, 10]. However, these factors do not completely explain the variability in the natural history of lung disease in AATD [11, 12]. Although individual cases may have poor evolution, it is recognised that the majority of never-smoker, non-index patients with AATD have the same survival as the general population and therefore may not require any specific treatment [13]. However, early identification of at-risk individuals is crucial because treatment only slows down the evolution of emphysema, it does not restore the damaged lung [14].
Indications for and regimens of augmentation therapy have remained unchanged for >30 years [15], but evidence has accumulated suggesting that treatment needs may be different for different patients [16]. Only recently, the biochemical efficacy of double doses of AAT was tested in a pilot study [17] and a clinical trial comparing different doses is ongoing [18]; different routes of administration, such as inhaled AAT, have also been explored [19]. It is clear that more research is needed on identifying the right therapeutic regimen in a more personalised approach to augmentation therapy [16]. Interestingly, the research priorities identified by the survey matched very well with those proposed by the ERS task force on AATD (table 1) [2].
Other research priorities that were selected by both healthcare providers and patients were the need for early and accurate diagnosis and the design of targeted screening programmes. Because both lung and liver AATD-associated diseases are irreversible, early identification is crucial to stop the evolution of the disease at mild initial stages [20, 21]. Studies conducted in the 1990s showed that, on average, patients with AATD had a delay in diagnosis of around 8 years and >20% of patients had visited four or more physicians before the diagnosis was established [22]. Moreover, this finding refers to those who were diagnosed, but epidemiological studies have indicated that despite several information campaigns and detection programmes, the majority of patients remain undiagnosed and do not receive appropriate care [1, 6]. It is not surprising that early diagnosis and the development of effective screening programmes were selected as top priorities by patients and healthcare providers.
Patients’ and caregivers’ research priorities
Dissemination of information about the disease is a necessary first step to improve early and accurate diagnosis of AATD. One of the first priorities for patients was improving knowledge about AATD among GPs. Different surveys in European countries have demonstrated the gaps in knowledge about AATD among different specialists, and in particular among GPs [23, 24]. This is relevant because in many countries GPs attend the majority of patients with COPD and they are the first contact for these patients with the health system; therefore, if early diagnosis is the goal, improving knowledge and awareness among GPs must be a priority action.
One of the top priorities for patients and caregivers was access to specialised, reference centres for AATD care. Owing to the low prevalence of AATD, it is almost impossible for a single clinician or department to accumulate enough expertise in its diagnosis and management; therefore, care for patients with AATD is best organised in reference centres that can provide the highest standard of care and advice to the individuals affected and their families while also contributing to knowledge accumulation. This is in line with the recommendations of the European Commission on management of rare diseases [25]. The recent ERS statement on AATD included a description of the optimised format of service provision by a reference centre for AATD [2]. These reference centres must establish a registry of their activity and collect information on the natural history of the patients prospectively. The development of registries is crucial because it is the only way to successfully accumulate knowledge about the clinical characteristics, evolution, natural history and response to treatment of patients with rare diseases such as AATD.
The next priority for patients was access to reliable information. This is very relevant in an era of misleading information, and it is important for patients to be able to identify reliable sources of medical information, e.g. information from scientific societies and patients' associations. Examples of reliable sources of patient information and support for the AATD community are ELF (www.europeanlung.org), Alpha-1 Global (www.alpha1-global.org), the Alpha-1 Foundation (www.alpha1.org) and several national Alpha-1 patients' associations, including the Alpha-1 UK Support Group (www.alpha1.org.uk) and Alpha1 Deutschland (www.alpha1-detschland.org).
Finally, among the top priorities for patients was the need to recognise an exacerbation and some aspects related to exercise and rehabilitation. These are medical aspects relating to self-management that can potentially improve the quality of life of the patients, but, interestingly, they were ranked just below some other organisational aspects of the disease.
Challenging aspects to manage for patients and barriers for treatment
Patients identified problems related to decreased exercise tolerance and shortness of breath as the most difficult to manage, followed by other similar concepts such as tiredness and fatigue. Other respiratory symptoms, such as cough or even exacerbations, were not perceived as so difficult to manage. This is related to the finding that access to pulmonary rehabilitation, to maintenance exercise classes and to fitness centres were among the most challenging barriers for treatment mentioned by patients. Strategies to provide adequate access to pulmonary rehabilitation and for maintaining adequate levels of physical activity must be encouraged.
Professional implications and additional costs due to the disease or therapy were also very high in the ranking of barriers for treatment. Patients with lung disease associated with AATD are younger than patients with usual COPD and in most cases professionally active. The disease may, therefore, have a huge impact on their professional lives and economic status.
Differences between patients living in countries where augmentation is reimbursed or not
The ERS statement on AATD [2] highlighted the differences in access to specialised care and specific treatments for patients in Europe. Regarding augmentation therapy, there are inequalities of access across different European countries [25, 26], which were confirmed in a recent European survey [27]. Even in countries where augmentation is available and reimbursed, there are differences in prescribing habits between regions, cities and even centres in the same city depending on personal views of attending physicians about efficacy of treatment [27]. These differences in access to treatment have an impact beyond the direct effect of therapy. In our survey, we observed worse scores in all challenging aspects of management in patients living in countries where augmentation is not reimbursed. It is likely that patients living in countries where augmentation is reimbursed may have more frequent contact with healthcare providers and better knowledge about their disease. This is a new and unexpected finding of our survey that requires corrective actions in countries without augmentation therapy available.
Not surprisingly, the most challenging barrier for treatment for patients in non-reimbursed countries was, by far, access issues to augmentation therapy, while patients in reimbursed countries indicated that maintenance of physical activity was the most challenging barrier for treatment. Again, in the majority of items, patients in non-reimbursed countries gave a lower (worse) score than patients in reimbursed countries.
Conclusions
The main research and management priorities identified by healthcare providers and patients included 1) markers of prognosis of the disease and understanding the natural history of AATD; 2) personalised treatment: when, which regimen and to whom; 3) improve information to physicians, including GPs, and improve early and accurate diagnosis; 4) access to specialised, reference centres and to reliable information for patients; 5) equal opportunities for accessing existing therapies: augmentation, pulmonary rehabilitation and maintenance of physical activity.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material S1 00523-2020.supplement_S1
Supplementary material S2 00523-2020.supplement_S2
Supplementary material S3 00523-2020.supplement_S3
Supplementary material S4 00523-2020.supplement_S4
Supplementary material S5 00523-2020.supplement_S5
Acknowledgments
We want to acknowledge the support from Elise Heuvelin and Céline Genton (European Respiratory Society, Lausanne, Switzerland) in logistics and organisation of EARCO, and from Barbara Johnson (European Lung Foundation) for helping in the organisation of this survey.
Footnotes
This article has supplementary material available from openres.ersjournals.com
Members of EARCO CRC: Timm Greulich (Germany, co-chair), Marc Miravitlles (Spain, co-chair). Steering committee: Joanna Chorostowska-Wynimko (Poland), Ilaria Ferrarotti, (Italy), Noel G. McElvaney (Ireland), Karen O'Hara (UK, patients' representative), Jan Stolk (Netherlands), Robert A. Stockley, Alice Turner (UK), Marion Wilkens (Germany, patients' representative). EARCO members: Angelo Corsico, Luciano Corda (Italy), Maria Sucena (Portugal), Miriam Barrecheguren (Spain, ERS early career representative), Cristina Esquinas (Spain), David Parr, Beatriz Lara, Ravi Mahadeva (UK), Jan Chlumsky (Czech Republic), Sabina Janciauskiene, Robert Bals (Germany), Jens Ulrik Jensen (Denmark), Kostas Kostikas (Greece), Malcolm Kohler, Christian Clarenbach (Switzerland), Alan Altraja (Estonia), Wim Jenssens, Silvia Pérez-Bogerd (Belgium), Caroline Gouder (Malta), Ana Hecimovic (Croatia), Aleksandra Dudvarski (Serbia), Alvils Krams (Latvia), Ruxandra Ulmeanu, Ana Zaharie (Romania), Jean-François Mornex (France), Arzu Yorgancioglu (Tukey), Karin Schmid-Scherzer (Austria), Hanan Tanash, Eeva Piitulainen (Sweden), Oleksandr Mazulov (Ukraine), Yavor Ivanov (Bulgaria).
Conflict of interest: M. Barrecheguren reports speaker fees from Grifols, Menarini, CSL Behring, Boehringer Ingelheim and GlaxoSmithKline, and consulting fees from GSK and Novartis, outside the submitted work.
Conflict of interest: K. O'Hara reports non-financial support from the European Lung Foundation/European Respiratory Society and Mereo BioPharma Group PLC, personal fees and non-financial support from NICE, and non-financial support from Alpha-1 Global; the Alpha-1 UK Support Group has received grants from CSL Behring, and receives donations from individuals/companies as a result of fundraising activities.
Conflict of interest: M. Wilkens reports reimbursement of travel costs by the European Lung Foundation during the conduct of the study; as chairman of the patient organisation Alpha1 Deutschland e.V., he does not personally receive any donations, but the organisation receives money from public funds and the pharmaceutical industry (grants as well as, e.g. travel costs).
Conflict of interest: J. Boyd is an employee of the European Lung Foundation.
Conflict of interest: E. Kolda has nothing to disclose.
Conflict of interest: B. Lara has nothing to disclose.
Conflict of interest: J. Chorostowska-Wynimko reports grants, personal fees and non-financial support from Grifols, AstraZeneca and Pfizer, personal fees and non-financial support from MSD and BMS, personal fees from GlaxoSmithKline, Novartis, Chiesi and Roche, grants and personal fees from Boehringer Ingelheim, grants, personal fees and non-financial support from CSL Behring and CelonPharma, and personal fees from Amgen and Lekam, outside the submitted work.
Conflict of interest: I. Ferrarotti has received speaker and consulting fees from CSL Behring and Grifols
Conflict of interest: J. Chlumsky reports personal fees and non-financial support from CSL Behring, personal fees from AstraZeneca, personal fees and non-financial support from GlaxoSmithKline, and personal fees and non-financial support from Boehringer Ingelheim, Actelion and Takeda, during the conduct of the study.
Conflict of interest: C. Clarenbach reports personal fees from Roche, Novartis, Boehringer, GlaxoSmithKline, AstraZeneca, Sanofi, Vifor and Mundipharma, outside the submitted work.
Conflict of interest: T. Greulich reports grants from CSL-Behring, Grifols and Kamada during the conduct of the study; personal fees for lectures and advisory boards from AstraZeneca, Berlin-Chemie, Boehringer Ingelheim, Chiesi, CSL-Behring, Grifols, GlaxoSmithKline and Novartis, and grants from Grifols and the German Centre for Lung Research (DZL), Marburg, Germany (Deutsches Zentrum für Lungenforschung), outside the submitted work.
Conflict of interest: M. Miravitlles reports speaker fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Menarini, Rovi, Bial, Zambon, Sandoz, CSL Behring, Grifols and Novartis, consulting fees from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Bial, Gebro Pharma, CSL Behring, Laboratorios Esteve, Ferrer, Mereo Biopharma, Verona Pharma, Kamada, TEVA, Sanofi, pH Pharma, Novartis and Grifols, and grants from GlaxoSmithKline and Grifols, outside the submitted work.
Conflict of interest: M. Sucena reports speaker or consulting fees from Boehringer Ingelheim, CSL Behring, Grifols and Novartis, and personal fees from Bial, Boehringer Ingelheim, CSL Behring, DarSaúde, Gasoxmed, Grifols, Linde, Menarini, Novartis and VitalAire, outside the submitted work.
- Received July 25, 2020.
- Accepted October 9, 2020.
- Copyright ©ERS 2020
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.
References










