





Abstract
There is a lack of information about the influence of patient interfaces such as facemasks or mouthpieces on the effective dose of aerosolised drugs while using high-flow therapy in a clinical setting. These interfaces can improve pulmonary drug delivery over nasal cannulas but patient preference and comfort should also be considered.
The present work was to determine the effect of three different interfaces (nasal cannula, valved face mask, and mouthpiece) when combined with titrated oxygen flow on aerosol delivery in patients with COPD hospitalised due to acute exacerbation.
The variations between these interfaces were addressed in terms of change in lung function measurements pre-and post-inhalation, the delivered salbutamol dose, and patient tolerance to each interface.
A high-flow nasal cannula was the most comfortable interface used. However, its pulmonary drug delivery was significantly lower than both the valved face mask and mouthpiece (p<0.05). Although drug delivery was different with the three tested interfaces, the lung function improvements were similar.
Abstract
Delivery in high-flow therapy with a different interface https://bit.ly/3l7MJUb
Introduction
High-flow therapy (HFT) has acquired great interest in the past two decades as an alternative modality for providing respiratory support in critically ill patients [1]. However, the troublesome issue regarding HFT is the delivery of inhaled drugs efficiently to the lungs without temporarily stopping the gas flow to the patient. The obstacles that hinder efficient nebulisation and favour aerosol deposition within the HFT circuit are the existing humidified conditions and the use of higher flows in adults up to 60 L·min−1. Inhaling an aerosol through a nasal cannula creates turbulence and increases aerosol loss within the nasopharynx [2]. The use of patient interfaces such as a facemask or mouthpiece over a nasal cannula within a high-flow system can improve pulmonary drug delivery, but patient preference would be affected [3, 4]. The present work was to determine the effect of three different interfaces on aerosol delivery when combined with titrated oxygen flow within a high-flow system in patients with COPD. The variations were addressed between these interfaces in terms of change in lung function measurements pre- and post-inhalation, the delivered salbutamol dose, and patient tolerance to each interface.
Methods
The effects of a high-flow nasal cannula ((HFNC) Jiaxing Sim Medical Device Co. Ltd., Zhejiang, China), a high-flow valved facemask ((HFM) Aerogen Ltd., Galway, Ireland), and a high-flow mouthpiece ((HMP) NingboFiner Medical Instruments Co., Ltd., Zhejiang, China) were reported on the relative lung deposition and systemic bioavailability of salbutamol, routinely used in the management of acute exacerbations of COPD. Patients with COPD admitted to Beni-Suef University Hospital due to the incidence of acute exacerbations that had fallen into GOLD stages II and III, were randomised to receive the study dose of salbutamol by one of three interfaces (HFNC, HMP, and HFM) in a parallel design. The study was approved by the Ethical Committee of Faculty of Pharmacy, Beni-Suef University (REC-H-PhBSU-18002), and written informed consent was signed by all participants.
2.5 mg (2500 µg) of salbutamol (Farcolin respiratory solution, 5 mg·mL−1; Pharco Pharmaceuticals, Alexandria, Egypt) was delivered using a vibrating mesh nebuliser, Aerogon Solo nebuliser (Aerogen Ltd.) placed proximal to Fisher and Paykel heated humidifier (MR810, Fisher and Paykel Healthcare, Auckland, New Zealand) as shown in figure 1. A mixture of oxygen and room air was driven from the gas wall supply to obtain the target oxygen saturation (88–92%). The use of salbutamol by the patients was not allowed at least 12 h (washout period) before the experiments to ensure accurate measurement of salbutamol levels in urine. Ipratropium bromide (Atrovent Inhalation Solution, 2500 µg·mL−1, Boehringer Ingelheim, Egypt) was used as an alternative to relieve existing bronchoconstriction as the patients were hospitalised due to acute exacerbation.

Schematic diagram of in vivo setting showing the position of the aerosol generator and three different interfaces within the high-flow therapy circuit. A: mouthpiece; B: nasal cannula; C: facemask.
The study exclusion criteria were hypotension (systolic blood pressure <100 mmHg) as salbutamol use was contraindicated because of its vasodilator effect or arrhythmia or hypokalaemia or previously known hypersensitivity to salbutamol. Also, patients were not eligible to participate in the study if they had severe kidney dysfunction (glomerular filtration rate <20 L·min−1) as kidney function was a fundamental parameter in our study, based on the measurement of urinary pharmacokinetic parameters of the drug. The parent salbutamol drug and its metabolite are actively eliminated via renal excretion [5]. Consequently, if kidney function severely decreases, the drug will exhibit a longer half-life, and then its urinary pharmacokinetic parameters will be noticeably changed.
Pulmonary function tests were measured by a handheld spirometer (One Flow, Clement Clarke International, UK) before salbutamol inhalation (pre-bronchodilator (BD)) and 30 min after inhalation (post-BD). The manoeuvre was repeated three times to take the highest readings of forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), and FEV1/FVC ratio, according to the American Thoracic Society Guidelines [6]. Each patient included in the study collected a urine sample 30 min following dose inhalation and all urine up to 24 h following inhalation (cumulative 24-h urine sample). A 30-min urine sample and cumulative 24 h samples were used as indices of pulmonary salbutamol bioavailability and systemic bioavailability, respectively [7]. Any complaint from the patient regarding the interface was recorded.
On the next day, an ex vivo procedure was performed, where patients received their salbutamol dose by the same interface previously used. This time, a breathing filter was placed after the interface to collect the entire dose delivered. This procedure ensured that no salbutamol reached the patient [8]. Measurement of salbutamol mass in urine samples and breathing filters was performed by high-performance liquid chromatography [9]. Statistical analysis was performed by one-way ANOVA with the application of least significant difference correction to determine any difference between interfaces. A Chi-squared test was conducted to compare the number of patients complaining from each interface.
Results
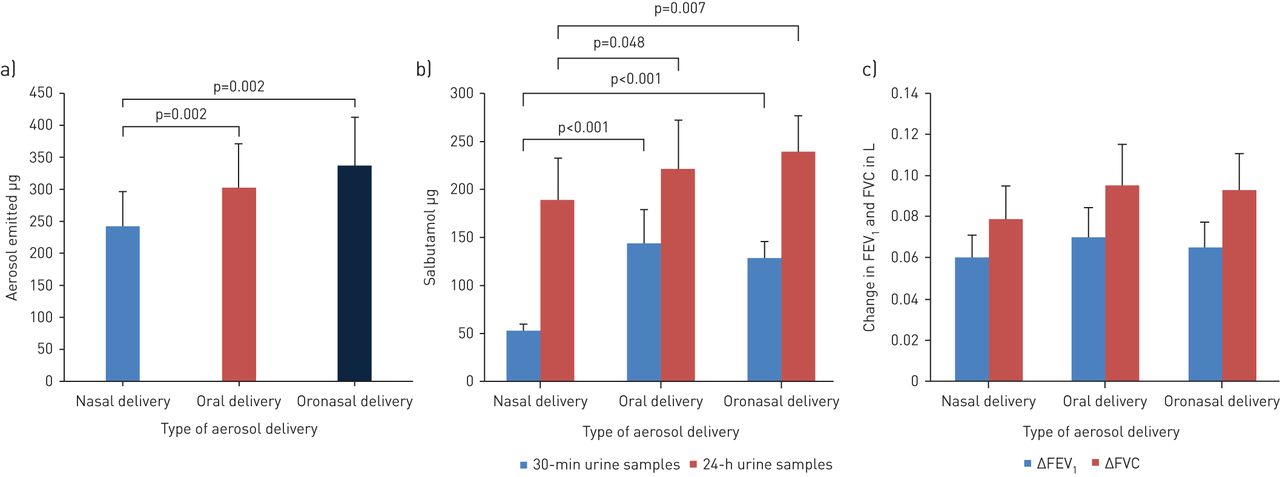
Thirty-six patients with COPD with a mean (sd) age of 62.6 (9.1) years, respiratory rate of 19.4 (3) breaths·min−1, and heart rate of 88.7 (8.6) beats·min−1 recorded by the multi-parameter patient monitor (Multi-parameter ECG Monitor Macs 10, SternMed, Germany) were included, where 12 patients were allocated to each group. Body mass index was 25.9 (4.2), 27.2 (3.5), and 26.3 (3.8) kg·m−2 for HFNC, HMP, and HFM groups, respectively. Comorbidities identified were hypertension, diabetes mellitus (DM), and gastro-oesophageal reflux disease (GERD). The percentage of participants who suffered from hypertension in each group was 25, 33, and 25% for HFNC, HMP, and HFM groups, respectively while the percentage of participants with DM was 25, 17, and 17% for HFNC, HMP and HFM groups, respectively. The percentage of participants had GERD was similar in each group (8%). No significant difference was found between the three groups in their demographic data and GOLD grading. The lowest salbutamol delivery to the ex vivo inhalation filter was found with HFNC compared with HFM and HMP at p=0.032 and p=0.002, respectively, while the salbutamol delivery with both HFM and HMP was statistically similar, as shown in figure 2a. Also, HFM and HMP showed statistically similar salbutamol amounts excreted in both 30-min and cumulative 24-h urine samples post-BD inhalation (figure 2b). HFNC resulted in the lowest salbutamol amount recovered from both 30-min urine samples (p<0.001) and cumulative 24-h urine samples (p=0.048 versus HMP and p=0.007 versus HFM). The oxygen flow reached by HFNC, HMP, and HFM to maintain target arterial oxygen saturation measured by pulse oximetry measured by pulse-oximeter was 12 (1.4), 16 (1.5), and 17.1 (1.1) L·min−1, respectively and inspiratory oxygen fraction was 30.2 (1.6), 37.8 (2.8) and 39.1 (2.2) for HFNC, HMP, and HFM, respectively.
{kind=link}
{kind=link}
Inhaled salbutamol delivery within the HFT system. a) Mean (sd) total emitted dose of salbutamol collected on ex vivo filters using different interfaces (nasal cannula, mouthpiece and valved facemask), b) mean (sd) salbutamol mass excreted in urine samples through the use of different interfaces, and c) mean (sd) change in forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) pre- and post-bronchodilator inhalation by different interfaces.
Mean (sd) spirometric parameters were as follows for HFNC, HMP and HFM groups: pre-BD FEV1=1.03 (0.21), 1.05 (0.19) and 1.07 (0.17) L, respectively and pre-BD FVC=1.71 (0.48), 1.75 (0.41) and 1.88 (0.37) L, respectively; and post-BD FEV1=1.09 (0.35), 1.12 (0.31) and 1.135 (0.26) L, respectively and post-BD FVC=1.79 (0.53), 1.84 (0.6) and 1.97 (0.46), respectively. These parameters were also expressed in percentage of predicted values for HFNC, HMP and HFM groups: pre-BD FEV1=37 (5.3) %, 37 (5) % and 36 (4.7) %, respectively and pre-BD FVC=46 (4.9) %, 47 (4.5) % and 49 (4) %, respectively; and post-BD FEV1=40 (4.6) %, 40 (4.3) % and 38 (3.6) %, respectively and post-BD FVC=48 (5) %, 49 (5.3) % and 52 (3.9) %, respectively. Change in pre-and post-BD values of FEV1 and FVC for each group is illustrated in figure 2c, where no significant difference was found between different groups in the measured lung function parameters.
The numbers of patients complained from HFNC, HPM, HFM use were 8.3%, 33.3%, and 50%, respectively. Examples of patient complaints recorded by the researcher were asking the nurse to remove the interface or intentionally removing it once or several times or noncompliance during the aerosol delivery procedure. The highest percentage of complaints were seen with HFM (p=0.001 and p=0.041 versus HFNC and HMP, respectively).
Discussion
The lowest values of ex vivo total delivered salbutamol dose and fractions recovered from 30-min and 24-urine samples were noticed with HFNC. These findings were consistent with many previous studies indicated the lower delivery efficiency of such interfaces [2, 10]. However, the highest patient tolerability and preference were reported with HFNC as only 8% of participants complained of this interface [2, 8, 10]. HMP and HFM showed approximately similar results of the ex vivo total delivered dose and the recovered fractions of salbutamol from urine samples and were significantly higher than that of HFNC (p<0.05). Consequently, a better pulmonary deposition could be obtained with HMP and HFM interfaces. The difference between these interfaces could be due to the breathing route targeted by each interface, which plays an important role in determining the dose reaching the lungs. HFNC targets nasal aerosol inhalation, while the nose acts as an efficient filter decreasing the penetration of the inhaled particles into the lower respiratory tract compared with the oral inhalation through the mouth targeted by either HMP or HFM [11]. However, the percentage of patients complaining about the use of HMP or HFM was significantly higher compared with the HFNC group (p<0.05). Also, the fraction of salbutamol recovered from 24-h urine samples significantly increased with using HMP or HFM compared with HFNC (p<0.05), and therefore patients would be subjected to more systemic side effects of the drug [12]. Facial and ocular depositions were the main complaints previously reported with the use of facemask in addition to hindering eating and speech leading to interface displacement and less compliance [13, 14]. The main problem noticed with HMP use was related to the inability of the patient to cooperate to maintain the interface in the mouth during the whole procedure. Therefore, its use in unconsciousness patients, during sleep, and for drug delivery with prolonged nebulisation time may be discouraged. The change in lung function parameters (FEV1, and FVC) post-dose inhalation was approximately similar to three tested interfaces ensuring their ability to saturate the target β2 receptors even with the lowest dose delivered by the HFNC. The increase in FEV1 was noted to be below that indicated for significant bronchodilator response (≥200 mL from pre-BD values). As three tested interfaces showed different drug delivery but with similar lung function improvements, the preference of one interface's use within the HFT system could depend on patient comfort and tolerability.
Limitations of the study included the absence of urinary salbutamol level pre-intervention (baseline level), small sample size, and the nonblinded and parallel design of the trial.
Conclusions
HFNC was the most comfortable interface used but lower aerosol delivery was achieved with its use. Although drug delivery was different with the three tested interfaces, lung function improvements were similar. HFNC could be replaced by either HMP or HFM to guarantee better delivery without temporary stopping of gas flow during dose administration.
Footnotes
Author contributions: Yasmin M. Madney: experiment, data entry, writing and statistics; Nabila Ibrahim Laz: concept and planning of study design; Ahmed A. Elberry: concept and planning of study design; Hoda Rabea: concept and planning of study design; Mohamed E. Abdelrahim: concept, planning of study design and writing.
Conflict of interest: Y.M. Madney has nothing to disclose.
Conflict of interest: N.I. Laz has nothing to disclose.
Conflict of interest: A.A. Elberry has nothing to disclose.
Conflict of interest: H. Rabea has nothing to disclose.
Conflict of interest: M.E. Abdelrahim has nothing to disclose.
- Received April 15, 2020.
- Accepted September 23, 2020.
- Copyright ©ERS 2021
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










