





Abstract
Objective Improved pneumonia diagnostics are needed, particularly in resource-constrained settings. Lung ultrasound (LUS) is a promising point-of-care imaging technology for diagnosing pneumonia. The objective was to explore LUS patterns associated with paediatric pneumonia.
Methods We conducted a prospective, observational study among children aged 2 to 23 months with World Health Organization Integrated Management of Childhood Illness chest-indrawing pneumonia and among children without fast breathing, chest indrawing or fever (no pneumonia cohort) at two district hospitals in Mozambique and Pakistan. We assessed LUS and chest radiograph (CXR) examinations, and viral and bacterial nasopharyngeal carriage, and performed a secondary analysis of LUS patterns.
Results LUS demonstrated a range of distinctive patterns that differed between children with and without pneumonia and between children in Mozambique versus Pakistan. The presence of LUS consolidation or interstitial patterns was more common in children with chest-indrawing pneumonia than in those without pneumonia. Consolidations were also more common among those with only bacterial but no viral carriage detected (50.0%) than among those with both (13.0%) and those with only virus detected (8.3%; p=0.03). LUS showed high interrater reliability among expert LUS interpreters for overall determination of pneumonia (κ=0.915), consolidation (κ=0.915) and interstitial patterns (κ=0.901), but interrater reliability between LUS and CXR for detecting consolidations was poor (κ=0.159, Pakistan) to fair (κ=0.453, Mozambique).
Discussion Pattern recognition was discordant between LUS and CXR imaging modalities. Further research is needed to define and standardise LUS patterns associated with paediatric pneumonia and to evaluate the potential value of LUS as a reference standard.
Abstract
This study explored distinctive lung ultrasound patterns associated with paediatric community-acquired pneumonia in Mozambique and Pakistan, and found reliable pattern recognition critical to identifying pneumonia https://bit.ly/3eWWvXr
Introduction
Pneumonia remains the leading infectious killer of children [1]; effective and timely diagnosis is critical to saving lives. Paediatric pneumonia is difficult to diagnose, especially in resource-constrained settings [2]. Advantages of ultrasound (LUS), a point-of-care tool that can dynamically visualise lungs with promising diagnostic accuracy for pneumonia and greater sensitivity or specificity when compared with chest radiography (CXR), include lower cost, portability, ease-of-use and absence of ionising radiation [3–5]. Key to evaluating the use case of LUS in pneumonia diagnosis in resource-constrained settings is a better understanding of the LUS patterns associated with paediatric pneumonia. We conducted a pilot study in Mozambique and Pakistan to investigate use of LUS for diagnosis and found that among children with World Health Organization (WHO) Integrated Management of Childhood Illness (IMCI) chest-indrawing pneumonia, expert LUS interpreters may achieve substantially higher interrater reliability (IRR) for LUS compared to CXR [6]. We chose to focus on non-severe chest-indrawing pneumonia rather than more severe pneumonia in this study, since we believed it unlikely that LUS imaging would change initial management of severe pneumonia, which is typically treated with intravenous antibiotics. In this secondary analysis, we explore distinctive LUS patterns associated with paediatric pneumonia and potential patterns associated with viral and/or bacterial nasopharyngeal carriage.
Methods
Study design, setting and participants
Methods and primary results of this prospective, observational, facility-based cohort study were described previously [6, 7]. The primary objective was to provide evidence assessing whether the addition of LUS to current pneumonia care pathways improves identification of pneumonia in children presenting to district hospitals in Manhiça, Mozambique and Karachi, Pakistan. Secondary and exploratory objectives included identifying LUS patterns among children with and without chest-indrawing pneumonia and comparing those patterns to CXR patterns. We explored LUS patterns, and available biomarker and viral and bacterial nasopharyngeal carriage results.
Children aged 2 to 23 months meeting WHO IMCI chest-indrawing pneumonia case definition (chest-indrawing pneumonia cohort) in outpatient and/or emergency departments of the low-volume, rural Manhiça District Hospital in Manhiça, Mozambique and the high-volume, urban Sindh Government Children's Hospital–Poverty Eradication Initiative in Karachi, Pakistan were screened sequentially during working hours by study staff to determine eligibility (table 1, figure 1). A separate group of 40 children presenting with complaints of cough or difficulty breathing but without fast breathing, chest indrawing or fever (no pneumonia cohort) was also screened. Conducted in accordance with the International Conference on Harmonisation, Good Clinical Practice and Declaration of Helsinki 2008, the study was approved by the Western Institutional Review Board, Comité Nacional de Bioética para a Saúde (246/CNBS/17), Comite de Ética del Hospital Clínic de Barcelona (HCB/2017/0074) and Aga Khan University Ethics Review Committee, and registered with ClinicalTrials.gov (NCT03187067).
Study definitions and eligibility criteria

a) Flow of children with chest-indrawing pneumonia by country: Mozambique (M) and Pakistan (P). b) Flow of children with no fast breathing, no chest indrawing and no fever by country. #: 70 children in Mozambique (27.3% of screened) and 1318 children in Pakistan (81.8% of screened) met the “no chest indrawing” exclusion criterion.
Study procedures
After enrolment on Day 1, eligible children underwent history, physical examination and LUS and CXR examinations. Enrolled children received local standard of care without the results of LUS examinations informing clinical care.
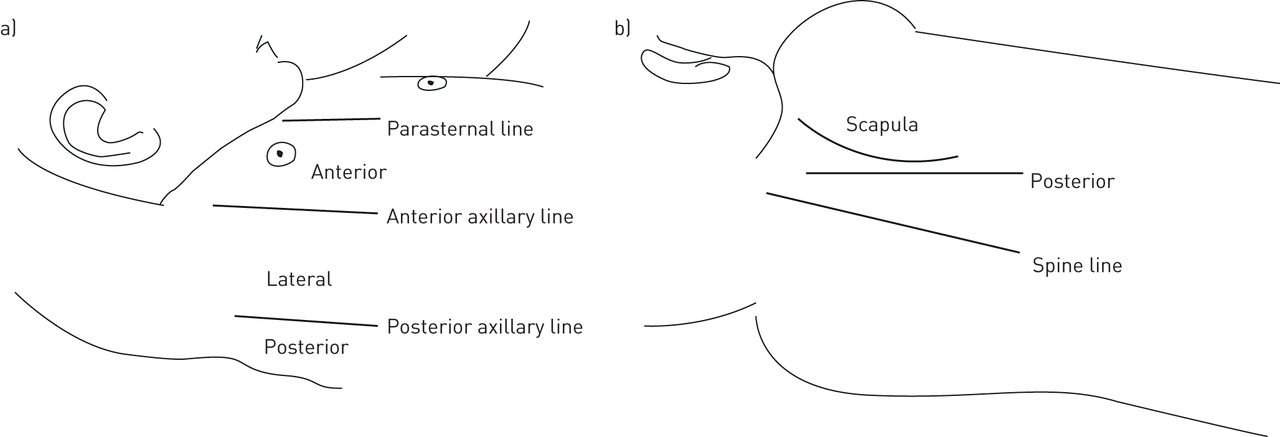
LUS examinations (longitudinal and oblique scans obtained of the anterior, lateral and posterior sides of the chest, figure 2) with a linear probe were performed by four trained non-physician healthcare personnel (nurse and medical agent in Mozambique, and two radiology technicians in Pakistan) who received a 1-day standardised training course and 3-day supervised practice. LUS interpretation using a standardised scoresheet targeted detection of typical lung consolidations, pleural effusions, interstitial patterns and obstructive atelectasis [7, 8]. End-point pneumonia using LUS was defined as the presence of consolidations or pleural effusions. At least two independent physicians expertly trained in LUS interpretation and blinded to clinical presentation interpreted each examination. If discordant, a designated expert LUS interpreter acted as arbiter. LUS operators at each site also interpreted LUS scans independently from one another. All interpretations were performed in batches at a later time using the same standardised scoresheet.

{kind=link}
{kind=link}
Lung ultrasound examinations consisted of longitudinal and oblique scans obtained of the anterior, lateral and posterior sides of the child's chest.
Anteroposterior CXR images were collected based on standard practice at each study site. A CXR interpretation panel of six expert interpreters investigated radiographic indicators of WHO CXR standardised primary end-point pneumonia [9–12]. At least three independent WHO CXR-trained physicians interpreted each CXR. Three interpretations were randomly selected, and if the first two interpretations were discordant, the third would act as tiebreaker.
Blood samples were tested for haemoglobin and C-reactive protein in Mozambique and Pakistan, and for procalcitonin, malaria and HIV in Mozambique. Nasopharyngeal aspirates and/or swabs were tested for respiratory viral PCR in Mozambique and Pakistan, and bacterial PCR in Mozambique using commercial multiplex tests.
Statistical analysis
Chi-squared tests, Fisher's exact tests, and t-tests were used to compare baseline characteristics of children by country and cohort. Tests were two-sided with α=0.05. Multiple comparison adjustments were not made, given the exploratory aims of the analyses. IRR among expert LUS interpreters and among expert CXR interpreters were estimated by cohort using Cohen's kappa (κ). All analyses were performed using R (version 3.5.1; R Foundation for Statistical Computing).
Results
Enrolment began in August 2017 in Mozambique and October 2017 in Pakistan. The last visits were completed in June 2018 in Mozambique and April 2018 in Pakistan. Baseline LUS videos were available for 98 out of 100 and 128 out of 130 children with chest-indrawing pneumonia in Mozambique and Pakistan, respectively (figure 1a), and all 40 in the no pneumonia cohort (figure 1b), with baseline characteristics by cohort and country provided in table 2. One child with an oxyhaemoglobin saturation <90% was incorrectly enrolled in the chest-indrawing pneumonia cohort in Mozambique. The results reflect the available data from these 226 children in the chest-indrawing pneumonia cohort and 40 children in the no pneumonia cohort. Among children with pneumonia, there were more fevers (21.4% versus 8.6%, p=0.01), but less fast breathing (53.1% versus 64.6%, p=0.10) in Mozambique than Pakistan. One child had hypoxaemia in Mozambique and none in Pakistan. C-reactive protein measurements were available for 93 and 128 children with pneumonia in Mozambique and Pakistan, respectively, and were on average lower in Mozambique than Pakistan (38.8 versus 109.9 µg·mL−1, p<0.01). Among children without pneumonia, C-reactive protein measurements were available in Mozambique, and on average were lower than those among children with pneumonia (18.2 versus 38.8 µg·mL−1, p=0.03). Procalcitonin measurements were available for 93 children with pneumonia and 20 children without pneumonia in Mozambique. Average levels were higher in the former group (1.7 ng·mL−1) than the latter (0.2 ng·mL−1) (p=0.07).
Baseline characteristics of enrolled and analysed children by cohort and country
Nasopharyngeal viral carriage results were available for 98 children with pneumonia and 20 children without pneumonia analysed from Mozambique, and 100 children with pneumonia analysed from Pakistan (supplementary appendix 1). Presence of any respiratory virus was similarly high across all tested children in both countries (91.8% Mozambique pneumonia; 84% Pakistan pneumonia; 95% Mozambique no pneumonia). However, the average number of viruses per child was higher among children with pneumonia in Mozambique (1.67) than in Pakistan (1.08; p<0.01) or among children without pneumonia in Mozambique (1.25; p=0.01).
Streptococcus pneumoniae nasopharyngeal carriage results were available for 97 children with pneumonia in Mozambique, while remaining bacterial carriage results were available for all 100 children with pneumonia and 20 children without pneumonia in Mozambique. Most children with pneumonia in Mozambique tested positive for S. pneumoniae (86.6%); 3.1% were positive for Bordetella pertussis and 3.1% for Mycoplasma pneumoniae (table 2). No children without pneumonia were positive for carriage of any of the tested bacterial strains.
Among 97 children with pneumonia in Mozambique for whom both viral and bacterial carriage results were available, eight were positive for at least one bacterial but no viral carriage, 12 were positive for at least one viral but no bacterial carriage and 77 were positive for at least one of both; no children were negative for all tested strains of both (table 3). Among viral-only positives, respiratory syncytial virus (RSV) and rhinovirus were the only strains that appeared without additional viruses in more than one child (three and two, respectively). Among mixed (both viral and bacterial) positives, RSV with S. pneumoniae (14 children), rhinovirus with S. pneumoniae (eight children) and adenovirus with rhinovirus with S. pneumoniae (seven children) were the three most common combinations present. Other combinations were each present in four or fewer children.
Baseline lung ultrasound pattern by nasopharyngeal carriage in the chest-indrawing pneumonia cohort in Mozambique
LUS patterns
Presence of any LUS consolidation was more common in children with chest-indrawing pneumonia than those without pneumonia (15.3% versus 0.0%, p=0.07, Mozambique; 45.5% versus 5.0%, p<0.01, Pakistan) as was presence of any LUS interstitial pattern (24.5% versus 10.0%, p=0.24, Mozambique; 62.5% versus 30.0%, p=0.01, Pakistan, table 4). Neither LUS presence of pleural effusion nor obstructive atelectasis was significantly different between those with and without pneumonia in Mozambique (0.0% throughout) or Pakistan (1.6% versus 0.0%, p>0.99; 2.3% versus 0.0%, p>0.99, respectively). Among those with pneumonia, LUS consolidation and interstitial patterns were significantly more common in Pakistan than Mozambique (p<0.01 for each comparison), though LUS effusion and obstructive atelectasis were not (p=0.51; p=0.26, respectively). Among those without pneumonia, consolidation and interstitial patterns were not significantly more common in Pakistan than Mozambique (p>0.99; p=0.24, respectively), and effusion and obstructive atelectasis patterns were absent in all children.
Baseline lung ultrasound imaging patterns of children by cohort and country
Expert LUS interpreters showed very high levels of IRR in overall determination of pneumonia (κ=0.915), consolidation (κ=0.915), effusion (κ=1) and interstitial patterns (κ=0.901) among children with pneumonia; estimated IRR was lower, but still moderate to good for obstructive atelectasis (κ=0.746) (table 5). Of note, the unusual κ=1 occurred because of very small numbers of children with pleural effusions.
Inter rater reliability among lung ultrasound experts
When both expert LUS interpreters determined a given imaging pattern was absent for all children, the κ-value for that imaging pattern was undefined, as was true for children without pneumonia with respect to presence of effusion and obstructive atelectasis. Among children without pneumonia, IRRs for overall pneumonia and for consolidations were estimated to be 1, but these were due to the small number of children with any findings on LUS. IRR for interstitial patterns was moderate (κ=0.635), but again, numbers were small.
No additional patterns of differences in LUS results were evident when comparing children with and without viral nasopharyngeal carriage (data not presented). Among children with pneumonia in Mozambique for whom viral and bacterial nasopharyngeal carriage results were available, presence of consolidations differed significantly between bacterial-only, mixed positives and viral-only (50.0% versus 13.0% versus 8.3%, p=0.03); other imaging patterns did not (table 3).
CXR patterns
Differences in presence of CXR imaging patterns between cohorts within each country were not significant except for interstitial patterns in Pakistan. CXR interstitial patterns were common in both countries for children with pneumonia (36.1%) and less common among those without pneumonia in Mozambique (15.0%, p=0.12) and Pakistan (10.0%, p=0.04). Presence of CXR consolidation was more common in Mozambique than Pakistan in both chest-indrawing pneumonia and no pneumonia cohorts (18.6% versus 9.8%, p=0.09; 20.0% versus 0.0%, p=0.11, respectively) (supplementary appendix 2). Presence of effusion was detected by CXR in one child with pneumonia in Mozambique (1.0%), while obstructive atelectasis was detected by CXR in one child with pneumonia in Pakistan (0.8%).
Comparison of LUS and CXR patterns
In assessing concordance between expert LUS versus expert CXR interpretations regarding presence of consolidation in the chest-indrawing pneumonia cohort, κ=0.453 for Mozambique and κ=0.159 for Pakistan; for the no pneumonia cohort, four consolidations were detected by LUS but none by CXR in Mozambique, resulting in κ=0, and one was detected by CXR but none by LUS in Pakistan, also resulting in κ=0 (supplementary appendix 3). Regarding presence of effusion in the pneumonia cohort (data not shown), although two were detected by LUS in Pakistan, none were detected by CXR, resulting in κ=0; likewise, 1 was detected by CXR in Mozambique but none by LUS, also resulting in κ=0. Corresponding κ-values were undefined for those without pneumonia because no effusions were detected by either modality.
Discussion
In our pilot, LUS demonstrated a range of distinctive patterns that differed between children in the chest-indrawing pneumonia and no pneumonia cohorts and between children in Mozambique versus Pakistan. Presence of consolidation or interstitial patterns was more common in children diagnosed with chest-indrawing pneumonia based on WHO IMCI criteria than in those without pneumonia. Presence of pleural effusion or obstructive atelectasis patterns was not significantly different among those children with and without pneumonia, though this was based on small numbers of LUS effusions and obstructive atelectasis. In Pakistan, differences in identification of consolidation and interstitial patterns between those with and without pneumonia were statistically significant. Rates of consolidation and interstitial patterns were significantly higher in Pakistan than Mozambique, possibly due to differences in severity of disease for those eligible and enrolled. Other possible explanations for the different LUS patterns observed among children with chest-indrawing pneumonia include differing epidemiologies of etiological pathogens, presentations of disease, host susceptibility and environmental factors, healthcare-seeking behaviours, and healthcare facility levels (low-volume, rural district hospital in Mozambique and high-volume urban hospital in Pakistan), among others.
Among children with chest-indrawing pneumonia, most children with consolidation also had interstitial patterns in one or both lungs (12 out of 15 (80.0%), Mozambique and 54 out of 57 (94.7%), Pakistan). Of those children with chest-indrawing pneumonia with interstitial patterns, 50% (12 out of 24) in Mozambique and 32.5% (26 out of 80) in Pakistan demonstrated interstitial patterns without consolidation. Thus, children with chest-indrawing pneumonia demonstrate a mix of LUS patterns.
Among children with chest-indrawing pneumonia in Mozambique, consolidations were detected at a higher rate in those with bacterial carriage only (no viral carriage), and more frequently but to a lesser extent among those with mixed bacterial and viral carriage, than among those with viral carriage only. Interstitial patterns were again most frequent among those with bacterial carriage, but least frequent among those with mixed bacterial and viral carriage. One could hypothesise that LUS might be able to assist with etiological detection although in the absence of microbiological diagnosis and confirmation, more research would be necessary. It is not surprising that we find a high percentage of nasopharyngeal carriage in children without pneumonia, but this also implies that these comparisons between carriage and disease are not necessarily indicative of clinical disease status or severity. In a study evaluating LUS use during the 2009 H1N1 influenza A pandemic, investigators defined viral pneumonia as the presence of small subpleural consolidations usually <0.5 cm and/or individual B-lines or confluent B-lines (interstitial pattern), and bacterial pneumonia as the presence of lung consolidation with air bronchograms, and based on 54 observations found that IRR for distinguishing viral from bacterial pneumonia was 0.82 (0.63 to 0.99) [13].
While some variability in LUS pattern findings exists, in our study, LUS appears to be consistent with clinical presentation in identifying consolidation (except for one child in the no pneumonia cohort in Pakistan identified with consolidation on LUS). In the no pneumonia cohort LUS appears to overdiagnose interstitial patterns (eight children) while CXR appears to overdiagnose both consolidation (four children) and interstitial patterns (five children). Abnormal imaging patterns in the absence of clinical disease could lead to overtreatment with antibiotics.
Based on our limited sample, IRR between LUS and CXR was poor in identifying consolidation and pneumonia. Using LUS, it appears there is significantly more disease in Pakistan than Mozambique; however, using CXR, the opposite seems true (although not significantly). Depending on which imaging modality is used, there is different recognition of disease. The fact that recognition of disease on imaging differs between the study sites by imaging modality may appear paradoxical; however, this may be due to chance or to a lack of an imaging gold standard, making it unclear whether it is LUS or CXR that is performing poorly.
Because study populations and underlying epidemiologies were different between Mozambique and Pakistan, and sample sizes of enrolled children were relatively small at each study site, there were limitations in comparisons that could be made between sites, and between pneumonia and no pneumonia cohorts. Of note, of those screened, 81.8% in Pakistan versus 27.3% in Mozambique were not enrolled because they did not have chest indrawing. Possible explanations for this difference could include differences in healthcare-seeking behaviour at the two study sites and/or differences in screening procedures. Importantly, though, great care was undertaken to ensure that all eligibility criteria were met at both study sites. Enrolment in the pneumonia cohort in Mozambique was slower due to smaller presenting numbers than in Pakistan as evidenced by larger differences in those screened versus enrolled in Pakistan, and this may have led to sicker children being enrolled in Pakistan (as suggested by higher average C-reactive protein measurement, lower average oxyhaemoglobin saturations, and more LUS consolidation and interstitial patterns in Pakistan).
Additional limitations related to imaging interpretation. For LUS interpretation, detailed expert consensus on what constitutes clinically relevant disease does not exist. While LUS videos were reviewed independently, our expert reviewers were not completely independent because one had been trained by the other. For CXR interpretation methodology, despite being used widely for epidemiological and vaccine effectiveness studies, current WHO CXR interpretation methodology is not intended for clinical use; rather it is intended to serve as a research end-point, and thus, our expert CXR interpretations may miss more subtle disease.
Apart from being difficult to obtain, time-consuming, expensive and exposing its subject to ionising radiation, CXR is also not an ideal reference standard due to its high interrater variability [2–4, 12, 14–19]. In our study, CXR had poor IRR, even among expert CXR interpreters. Pattern recognition was discordant between LUS and CXR imaging modalities. Despite this discordance, LUS imaging may be preferable in identifying patterns; however, further research is needed to define and standardise LUS patterns associated with paediatric pneumonia. In addition, while more data may be needed to support LUS as a reference standard, in favour of LUS as a preferred imaging modality for paediatric pneumonia is its high IRR among expert LUS interpreters for overall determination of pneumonia, consolidation and interstitial patterns. LUS pattern recognition and image analysis is a potential tool to allow machine-learning and artificial intelligence-assisted automatic diagnosis of pneumonia. More research is needed to define and standardise LUS patterns associated with paediatric pneumonia and to evaluate the potential value of LUS as a reference standard.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00518-2020.SUPPLEMENT
Acknowledgments
We thank the dedicated study staff at Manhiça District Hospital in Manhiça, Mozambique and Sindh Government Children's Hospital–Poverty Eradication Initiative in Karachi, Pakistan for implementing the study and providing patient care. We thank Adelina Malembe and Zumilda Arão Boca in Mozambique and Fariha Sohail and Zunera Qasim in Pakistan for conducting and interpreting the lung ultrasound (LUS) examinations. We thank Campos Mucasse and Vania Afuale in Mozambique and Farrukh Abbasi, Zehra Aziz, Ghazala Sheikh, and Naveed Ahmad in Pakistan for general coordination and support of the study. We also thank the trial participants, their caregivers, and the local community in Manhiça, Mozambique and Karachi, Pakistan for their participation and support. In addition, we acknowledge Nick Fancourt and Steve Lacey for their technical guidance in the CXR portion of the study, and the expert panel of CXR interpreters (Rachel Benamore, Vera Manduku, Eric McCollum, Kate Park, Joyce Sande and Pui-Ying Iroh Tam) as well as Angelo Giovanni Del Monaco for providing LUS arbitration. We acknowledge Lilliam Ambroggio for her guidance in developing the standardised LUS and chest radiography forms.
Footnotes
This article has been republished to correct an error in the authors' affiliations.
This article has supplementary material available from openres.ersjournals.com
This study is registered at www.ClinicalTrials.gov with identifier number NCT03187067. Upon request, deidentified participant data that underlie the results reported in this article will be made available to researchers who provide a methodologically sound proposal following publication of the planned primary and secondary analyses. Proposals should be directed to the corresponding author.
Author contributions: A.S. Ginsburg conceptualised the study, obtained research funding, designed the study and data collection instruments, coordinated and supervised data collection from the sites, interpreted the data, and drafted the manuscript. J. Lenahan designed the study and data collection instruments, and coordinated and supervised data collection from the sites. A. Lamorte and G. Volpicelli provided input on the design of the study and designed the lung ultrasound methodology. F. Jehan and Q. Bassat provided input on the design of the study and supervised teams that acquired the data. Among the authors, P. Vitorino, M. Valente, B. Balouch, M.I. Nisar and Z. Qasim conducted the clinical procedures and acquired the data. J. Hwang and S. May performed the statistical analyses and interpreted the data, and drafted sections of the manuscript. C. Muñoz Almagro conducted laboratory analyses from Mozambique. All authors worked collaboratively to review and revise the manuscript and agree to be accountable for the work.
Conflict of interest: A.S. Ginsburg reports grants from the Bill and Melinda Gates Foundation during the conduct of the study.
Conflict of interest: P. Vitorino has nothing to disclose.
Conflict of interest: Z. Qasim has nothing to disclose.
Conflict of interest: J.L. Lenahan has nothing to disclose.
Conflict of interest: J. Hwang has nothing to disclose.
Conflict of interest: A. Lamorte has nothing to disclose.
Conflict of interest: M. Valente has nothing to disclose.
Conflict of interest: B. Balouch has nothing to disclose.
Conflict of interest: C. Muñoz Almagro has nothing to disclose.
Conflict of interest: M.I. Nisar has nothing to disclose.
Conflict of interest: S. May reports grants from the Bill and Melinda Gates Foundation during the conduct of the study.
Conflict of interest: F. Jehan has nothing to disclose.
Conflict of interest: Q. Bassat has nothing to disclose.
Conflict of interest: G. Volpicelli has nothing to disclose.
Support statement: This work was supported by grants from the Bill and Melinda Gates Foundation (OPP1105080) and Save the Children. Hosting of lung ultrasound and chest radiography interpretation data via REDCAP at The Institute of Translational Health Sciences was supported by a grant from the National Institutes of Health National Center for Advancing Translational Sciences (UL1 TR002319). CISM is supported by the Government of Mozambique and the Spanish Agency for International Development. ISGlobal receives support from the Spanish Ministry of Science and Innovation through the “Centro de Excelencia Severo Ochoa 2019–2023” Program (CEX2018-000806-S), and support from the Generalitat de Catalunya through the CERCA Program. Funding information for this article has been deposited with theCrossref Funder Registry.
- Received July 24, 2020.
- Accepted November 4, 2020.
- Copyright ©ERS 2021
This article is open access and distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0.










