





Abstract
New findings on pathophysiology, epidemiology, and outcome have raised concerns on the relevance of the apnoea–hypopnoea index (AHI) in the classification of obstructive sleep apnoea (OSA) severity. Recently, a multicomponent grading system decision integrating symptomatology and comorbidities (Baveno classification), was proposed to characterise OSA and to guide therapeutic decisions. We evaluated whether this system reflects the OSA population, whether it translates into differences in outcomes, and whether the addition of AHI improves the scheme. A total of 14 499 OSA patients from the European Sleep Apnoea Database cohort were analysed. The groups were homogeneously distributed and were found to clearly stratify the population with respect to baseline parameters. Differences in sleepiness and blood pressure between the groups were analysed in a subgroup of patients after 24–36 months of treatment. Group A (minor symptoms and comorbidities) did not demonstrate any effect of treatment on outcome. However, groups B (severe symptoms, minor comorbidities), C (minor symptoms, severe comorbidities) and D (severe symptoms and comorbidities) were associated with improvement in either or both parameters with treatment. The AHI is an essential prerequisite of the diagnosis; however, adding the AHI did not improve the classification. Rather, it was inferior with respect to guiding the treatment decision. Thus, the Baveno classification allows a better stratification of the OSA population and may provide a better guidance for therapeutic decisions in OSA.
Abstract
The Baveno classification separates the OSA population into equivalent groups that are clearly separated with respect to clinical symptoms and comorbidities. These groups are characterised by differences in hypoxic load and PROMs. https://bit.ly/3sIZqJu
Introduction
The relevance of obstructive sleep apnoea (OSA) for the individual and the society is well recognised relating to its prevalence and impact on societal health-related costs and patient-related outcomes [1–4]. OSA affects 9–13% of the general population, substantially reduces quality of life and increases morbidity [5–7] and mortality, at least in subgroups of affected patients [8, 9]. This constellation encouraged clinicians, manufacturers and healthcare administrators to seek simple and easily accessible markers of the disease to screen risk groups, to predict outcome and to more precisely select optimal treatment. Breathing disturbances during sleep, often associated with snoring, are the most prominent quantifiable markers of OSA. Thus, the number of apnoeas and hypopnoeas per hour of sleep (apnoea–hypopnoea index (AHI)) became the most widely used metric to define the disease and to classify the severity in most national and international guidelines and healthcare standards, including those related to reimbursement [10–13].
However, criticism and concerns regarding the clinical and prognostic relevance of the AHI have recently been raised [13, 14]. First, experimental data and clinical experiences have demonstrated that the pathophysiology of OSA is not reflected by upper airway obstruction alone. Second, several cluster analyses of large databases have consistently shown that the classical phenotype of obesity, male sex, older age and severe daytime sleepiness represents only one-quarter of the OSA population [15–21]. Other phenotypes, such as breathing disturbances associated with movement phenomena or insomnia, young age with comorbidities or female sex with less distinct or atypical symptoms, may also be identified [15–23]. Finally, the AHI is a poor predictor for end-points such as cardiovascular comorbidities or mortality. Other aspects, such as hypoxic burden or sleepiness seem to better predict outcome in OSA [15, 24–29].
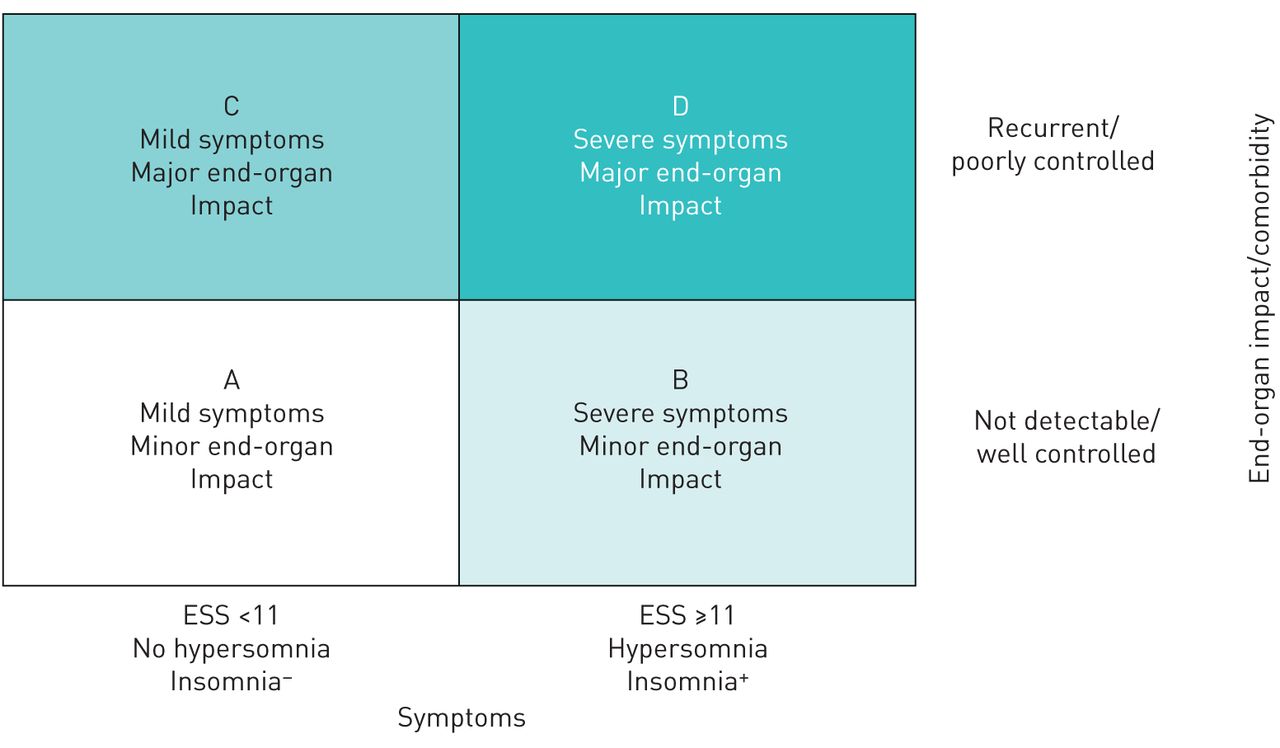
Based on these considerations, an ad hoc working group of the Sleep-Disordered Breathing Group of the European Respiratory Society and the European Sleep Research Society developed a new approach (beyond the AHI) to predict the disease, to integrate symptoms and cardiometabolic comorbidities. This workshop, which took place in Baveno, Italy [30], resulted in a two-dimensional scheme divided into four groups, A to D, and with the level of symptoms on the x-axis and the presence and severity of comorbidities on the y-axis (figure 1). The classification may guide indication and optimisation of treatment independent of the AHI. Affiliation to group D will strongly suggest treatment, while affiliation to group A will hardly indicate any active treatment other than general lifestyle recommendations. Groups B and C may warrant treatment either due to reduced quality of life or presence of relevant comorbidities.

The revised version of the Baveno classification. Details about symptom and comorbidity criteria are provided in the supplementary material. ESS: Epworth Sleepiness Scale. Reproduced from Randerath et al. [30].
However, this innovative proposal requires further validation before reshaping OSA routine care. Therefore, we evaluated whether the multicomponent grading system, namely the Baveno classification, can be transferred to a real-life situation in OSA patients. A slightly modified version of the Baveno classification system was applied to the large clinical cohort of the European Sleep Apnoea Database (ESADA) to determine whether:
the Baveno classification A–D sufficiently reflects the distribution of the patients in the ESADA cohort;
the addition of the AHI to the classification system might improve the characterisation of sleep apnoea patients; and
the classification translates in clinically relevant outcome parameters.
Methods
The ESADA registry is a multicentre, prospective patient cohort reflecting a network of 37 sleep centres in 20 countries in Europe and Israel [31, 32]. The overall objective of the ESADA is to generate a clinically representative cohort of subjects recently evaluated for suspected sleep-disordered breathing. A central web-based platform is applied to record patient information from the participating sleep centres. In brief, unselected patients (age 18–80 years) with suspected OSA are eligible for inclusion in the registry. At the time of initial sleep laboratory diagnostic work-up, anthropometric characteristics, information on daytime symptoms and health-related lifestyle, such as smoking and alcohol consumption, blood tests, medical history, medications and sleep data are collected. Subjective daytime sleepiness is quantified by the Epworth Sleepiness Scale (ESS) score [33]. The severity of sleep-disordered breathing is assessed by polysomnography (PSG) or polygraphy (PG) according to the prevailing clinical routine at each participating sleep centre [34]. The scoring criteria defined by the American Academy of Sleep Medicine 2007 definition have been used in the ESADA study protocol, which allowed hypopnoea scoring with either the recommended or the alternative definition [35]. The ESADA has previously analysed the impact of centre-specific differences in hypopnea scoring and the difference between AHI values from PSG and PG [34]. Office blood pressure is measured according to the current European Society of Hypertension and the European Society of Cardiology guidelines [36]. Corresponding follow-up data are collected when patients return as part of the clinical routine. The research ethics committee at each participating centre approved the ESADA protocol, and informed consent is obtained from all included patients.
For this analysis, we considered all patients with an AHI ≥5 h−1 and included all complete datasets for the parameters needed for allocation to the four Baveno groups. These parameters comprise symptoms and cardiometabolic comorbidities. Symptoms include daytime sleepiness, insomnia and hypersomnia. Comorbidities include atrial fibrillation, (uncontrolled) arterial hypertension, heart failure, stroke, and diabetes mellitus (see supplementary material for further details). For the baseline analysis, patients were classified as positive airway pressure (PAP) users based on the clinical decision to initiate any kind of PAP therapy, including continuous (CPAP), automatic (APAP) and bilevel PAP.
According to the heterogeneity of clinical practice and local healthcare regulations, follow-up data were available in a subgroup of the cohort. Follow-up data of 12–24 months were available for 1724 patients, 24–36 months for 1081, and >36 months for 953 patients. For the longitudinal analysis in this study, we used the data of those patients treated with CPAP (n=474) or APAP (n=468) at the time of their follow-up visits that occurred within a time window of 24–36 months. These groups and time windows were selected to generate a substantial number of patients and a relevant time frame for evaluation of an objective cardiovascular outcome parameter. Patients treated with bilevel PAP (n=95), or non-PAP therapies (n=29) were excluded.
In some part of the analyses, data were grouped according to the established severity levels of the baseline AHI (mild ≥5 to <15 events·h−1, moderate ≥15 to <30 events·h−1 and severe ≥30 events·h−1).
Statistical analysis
Continuous variables are expressed as median and quartiles 1 and 3. Data distribution was tested using the Shapiro–Wilk test. Data across patient groups were tested for significant differences applying one-way ANOVA with Tukey post hoc test for pairwise comparisons when normal distribution could be assumed. Otherwise, the Kruskal–Wallis test with Bonferroni post hoc tests was used. For comparisons between two groups, the t-test or the Mann–Whitney U-test were used as appropriate. Differences between baseline and follow-up within the same patients were tested with the one-sample Wilcoxon signed-rank test. Differences in percentages (if >0%) between two groups were tested with the two-proportions z-test with Bonferroni adjustment. The level of significance for all statistical tests was set at α=0.001. All analyses were performed using IBM SPSS Statistics for Windows (version 26.0; IBM Corp., Armonk, NY, USA).
Results
Baseline characteristics of the patients
The ESADA database currently includes 30 235 patients. After exclusion of files with missing data required for allocation to Baveno groups, 14 499 datasets were included for further evaluation, among which 943 were considered for follow-up analysis (figure 2). Study characteristics were as follows: 28% female, median age 55 (46; 63) years (median (quartile 1; quartile 3)) and body mass index (BMI) 31.6 (28.0; 36.2) kg·m−2.

Flow-chart of the inclusion process. ESADA: European Sleep Apnoea Database; PAP: positive airway pressure; PSG: polysomnography; PG: polygraphy; AHI: apnoea–hypopnoea index; SysBP: systolic blood pressure; DiaBP: diastolic blood pressure; CPAP: continuous positive airway pressure; APAP: automatic positive airway pressure.
The median ESS score was 10 (6; 13); 47% of the patients had a score <11 and 53% had ≥11. The median AHI was 30.8 events·h−1 (16.3; 52.9) and the oxygen desaturation index (ODI) was 27.0 events·h−1 (12.0; 50.8). The mean arterial oxygen saturation (SpO2) was 93% (91; 95), the minimum SpO2 was 81% (73; 86), and the cumulative sleep time when SpO2 was <90% (t90) was 15 min (2; 65).
Distribution according to the Baveno classification
The patient distribution of the total sample across Baveno groups A–D was: group A, n=3447 (24%); group B, n=2771 (19%); group C, n=4482 (31%); and group D, n=3799 (26%). There was a slight decrease of group A and increase of group D in patients with an AHI ≥30 events·h−1 (figure 3).

Distribution of the Baveno groups A–D in different apnoea–hypopnoea index (AHI) groups and in the overall patients.
There were no substantial differences in the sex distribution in each group. BMI increased linearly but slightly from groups A to D. The median age was highest (n=57 (48; 65)) in group C and lowest (n=52 (43; 60)) in group B (table 1).
Patient characteristics within the four Baveno groups A–D
AHI and ODI were higher in the groups with increased levels of clinical symptomatology (groups B and D); however, only group D showed relevantly lower median values of the mean and minimum SpO2. Interestingly, there were substantial differences in the t90, which was substantially higher in groups B–D compared to group A. Groups B and C differed only mildly from each other, while the figure for group D was remarkably higher (table 1).
Data on glycated haemoglobin (HbA1c) were available in 6104 patients. It was slightly and significantly (p<0.001) elevated in groups C (5.7% (5.4; 6.2)) and D (5.9% (5.5; 6.5)) as compared to the groups A (5.6% (5.3; 5.8)) and B (5.6% (5.4; 5.9)).
Clinical outcome according to the Baveno classification
The individual clinical decisions on therapy had obviously been made independent of the Baveno classification. Here we analysed how these decisions fit to the new system. At least 70% of the patients in every single Baveno group were prescribed PAP. However, therapy was more often considered for the symptomatic groups B and D (A: 71%, B: 80%, C: 70%, D: 82%). Overall, 943 patients on CPAP or APAP presented to follow-up visits between 24 and 36 months and all were considered for analysis. The median compliance was 6.0 h·day−1 (5.2; 7.0) and did not differ significantly according to Baveno groups, BMI quartiles, age or sex (see online supplement).
The median systolic and diastolic blood pressure improved significantly (p<0.001) and substantially by 5–10 mmHg compared to baseline in group C and group D, whereas there was no difference in group A and group B (figure 4).
The ESS score improved in all groups; however, the greatest changes were noted in groups B and D (figure 5).

Changes in systolic and diastolic blood pressure (BP) between baseline and follow-up in the different Baveno groups A–D. Circles denote outlier values (>1.5 interquartile ranges outside the box), asterisks denote extreme values (>3 interquartile ranges outside the box). #: p<0.001 baseline versus follow-up.
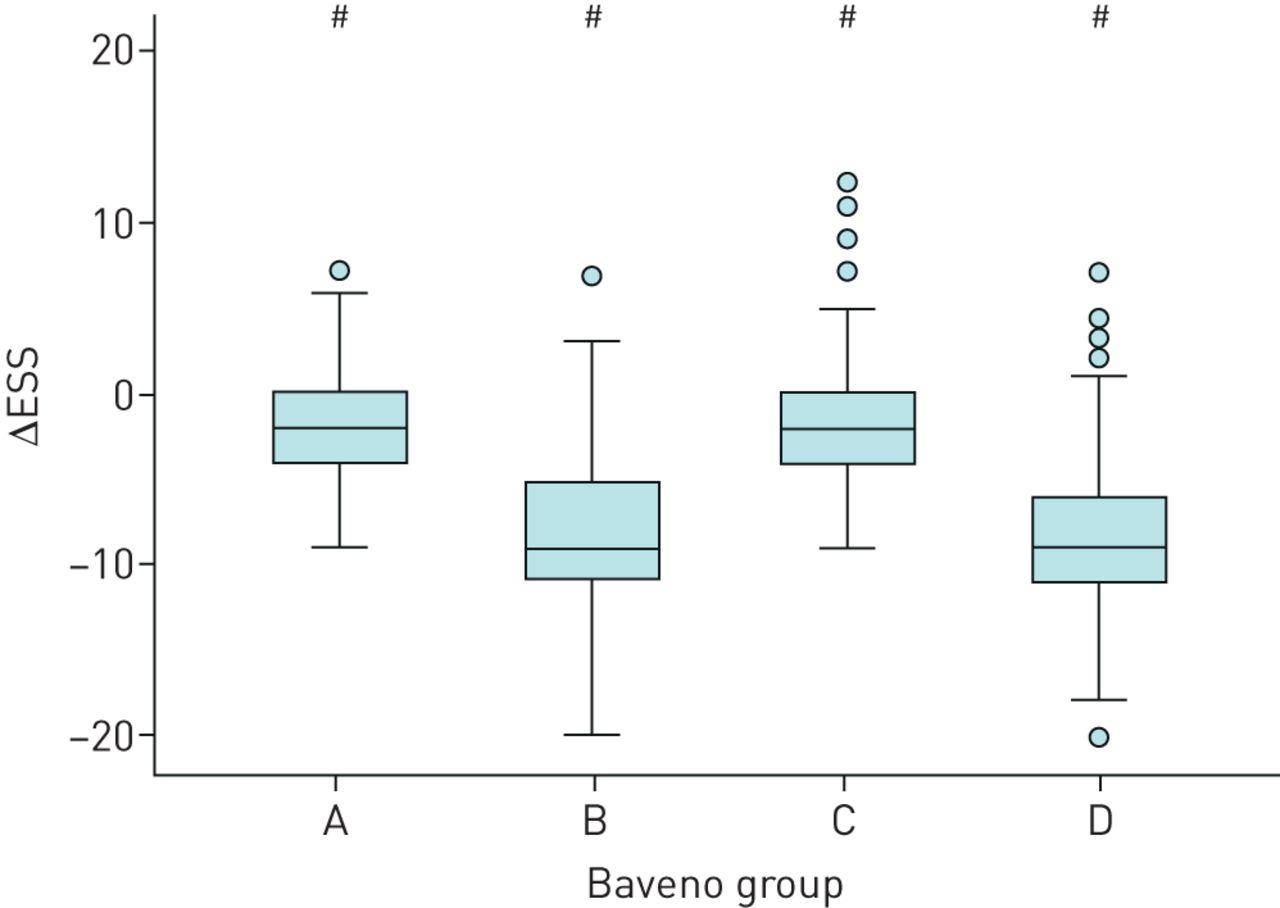
Change of the Epworth Sleepiness Scale (ESS) score between baseline and follow-up in the different Baveno groups A–D. Circles denote outlier values (>1.5 interquartile ranges outside the box). #: p<0.001 baseline versus follow-up.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percent of patients with positive airway pressure (PAP) prescription at baseline in the different apnoea–hypopnoea index (AHI) groups and in the whole study population. White columns represent actual PAP prescription as per conventional clinical routine decision; shaded columns represent PAP prescription as indicated by Baveno classification (i.e. Baveno groups B–D).
Discussion
The aims of this study focussed on the translation of the Baveno classification system of OSA to the ESADA cohort, a large real-life database. First, the findings demonstrate that integration of clinical symptoms and comorbidities as proposed in the Baveno system [30, 37] stratifies the population, independent of the AHI without considerable over- or underrepresentation any of the groups. The groups with severe symptoms and less comorbidity (B) and less symptoms and severe comorbidity (C) were similar regarding hypoxic burden while the most severe group in both parameters (D) clearly differed in most measurements of hypoxaemia and treatment indication. Second, symptoms seemed to drive the indication to treat more strongly than did comorbidities as shown by the different proportions of treated and untreated patients. Importantly, there was a substantial reduction of blood pressure in the groups with high prevalence of comorbidity. The median reduction of systolic blood pressure was 8.5 and 10.0 mmHg in groups C and D, respectively, which even exceeded the effects of CPAP on resistant arterial hypertension previously reported [38, 39]. Finally, the distribution of patients to the Baveno groups A–D did not differ substantially between AHI groups, except for a relatively higher value of group D in the AHI ≥30 group. This is in line with the results of recent studies emphasising the dominant relevance of other parameters than AHI to outcomes of OSA, such as symptoms, comorbidities, and hypoxic burden [13, 24, 25]. While the AHI is essential for the diagnosis of OSA, the Baveno classification may guide physicians better in their treatment decision.
The idea of advancing the classification of OSA based only on the AHI by a multicomponent scheme based on symptoms and comorbidities arose from several recent cluster analyses. Keenan et al. [16] studied 972 patients with OSA (AHI ≥15 events·h−1) in the Sleep Apnoea Global Interdisciplinary Consortium clustering the population based on 18 symptoms, cardiovascular and metabolic comorbidities. This study identified five groups as “disturbed sleep”, “minimally symptomatic”, “upper airway symptoms with sleepiness”, “upper airway symptoms dominant”, and “sleepiness dominant”. Bailly et al. [18] performed a cluster analysis of 18 263 participants of the French Sleep Apnoea Registry based on symptoms, findings, risk factors, and comorbidities and identified six clusters with 10–23% of the populations (“young symptomatic”, “old obese”, “multi-disease old obese”, “young snorer”, “drowsy obese”, “multi-disease obese symptomatic”). Zinchuk et al. [19] included polysomnographic parameters to their cross-sectional and longitudinal data analyses of 1247 patients. In a Cox-analysis, survival was significantly reduced in the clusters of “periodic limb movement syndrome”, “hypopnoea and hypoxia”, and “combined severe”. Importantly, the risk did not increase with AHI. Ye et al. [20] analysed 822 patients with moderate-to-severe OSA from the Icelandic Sleep Apnoea Cohort, and described three clusters (“insomnia”, “minimally symptomatic”, “excessive daytime sleepiness”) each containing 25–43% of the population. The clusters did not differ regarding sex, BMI or AHI. “Insomnia” and “minimally symptomatic” patients showed the highest prevalence of cardiovascular comorbidities. In addition, data from Arnardottir et al. [15] and Heinzer et al. [5], referring to the general population, showed no or limited association between the AHI and symptoms or comorbidities.
In our analysis, all classification groups contained substantial numbers of patients between one-fifth and one-third of the whole population. This suggests that the quartering of the OSA patients entirely based on symptoms and comorbidities represents an epidemiologically reasonable and clinically practicable compromise, supported by the distribution of recent cluster analyses [16, 18, 19].
The proportion of groups A–D did not differ substantially depending on the baseline AHI group. Therefore, the addition of the severity of breathing disturbances did not influence the relevance of symptoms and comorbidities to the classification of OSA in this population and underlines the previous findings from huge cluster analyses. There were almost no variations in patients with fewer comorbidities (A and B). Interestingly, there was a shift mainly from group A to D, with increasing baseline AHI severity. These groups did not differ regarding comorbidities but regarding symptoms. Thus, a therapy decision solely based on the AHI seems to miss severely ill patients with mild symptoms.
The mild but linear increase of the mean BMI from groups A to D probably reflects the association of comorbidities with the risk factor of obesity. Although there is no linear increase in the retrospective data for age, it was nevertheless higher in groups C and D (higher comorbidities) as compared to groups A and B.
Parameters of breathing disturbances during sleep also increased with the Baveno groups. This is especially true comparing groups A, B and C versus D. However, differences between B and C are much less pronounced. Interestingly, group B (more symptoms, fewer comorbidities) showed higher AHI and ODI as compared to group C (fewer symptoms, more comorbidities), whereas the hypoxic burden, as reflected by t90 [40, 41], did not differ between groups B and C. This suggests that the relevance of the disease and the indication for treatment of this half of the population is similar in patients who are either symptomatic or suffer from cardiometabolic comorbidities. However, the coexistence of symptoms and comorbidities (group D) results in the highest burden of the disease compared to all other groups.
The baseline AHI seems to play the most important role in PAP prescription in real life, irrespective of symptoms and comorbidities (figure 6). In the subgroup with low AHI (<15 events·h−1) PAP was prescribed in <30% of patients, although >70% had severe symptoms and/or comorbidities. In contrast, almost all patients with AHI ≥30 events·h−1 were prescribed PAP, although one-fifth presented neither symptoms nor comorbidities. Despite these findings, clinicians seem to indicate treatment in real life preferably based on symptoms rather than comorbidities as groups B and D show 10% higher prescription rates compared to group C. As the recently published [42] MERGE trial has found, even in mild OSA, PAP treatment significantly improves quality of life.
The PAP compliance in the complete follow-up population was 6.0 h·d−1 and did not differ when stratifying for the various comparisons of Baveno groups, sex, age and BMI. It is important to note that there were no relevant compliance differences between the Baveno groups A–D, which excludes an influence on the outcome parameters. The baseline data on hypoxic burden and the follow-up data on sleepiness and blood pressure confirmed the relevance of the classification system in several aspects: they proved the plausibility of the parameters included; they confirmed the separation of each of the four groups; and they confirmed the treatment indication based on the system. The median ESS score improved significantly in groups B and D by nine points each, which is of high clinical relevance. This shows that the parameters clearly discriminated between symptomatic and asymptomatic patients and confirms that CPAP has a huge effect in symptomatic patients. In addition, both systolic and diastolic blood pressure improved significantly and relevantly in patients with high impact of comorbidities (groups C and D). These results support the idea of indicating treatment based on the groups; groups B, C, and D improved in symptoms, in blood pressure or in both parameters. In contrast, group A differs in hypoxic burden, symptoms and comorbidities from all other groups and fails to show any benefit in the parameters investigated here despite similar compliance and thus, PAP treatment for these patients does not seem to be indicated. While the observed changes in blood pressure and ESS, especially in groups B and D, may in part be due to a regression to the mean, the (albeit lesser) improvement of ESS in groups A and C and the absence of an increase in median blood pressure in groups A and B strongly suggest that this is to a large extent an actual treatment effect. Our data reflect blood pressure recordings during clinical routine assessments with and without concomitant antihypertensive medication and thus, a large variability between blood pressure assessments in a proportion of patients could be expected. As each group comprises several thousand patients, a small group of patients with very large variability in blood pressure accounts for the occurrence of a certain proportion of elevated values on follow-up. Moreover, the proportion of hypertensive OSA patients was higher in groups C and D when compared to A and B (55% versus 30%). It is therefore expected that the blood pressure response to CPAP would be more pronounced in these groups.
Limitations
The retrospective design generally limits the conclusions of any study, mainly to incomplete or insufficient data. However, a strict exclusion process allowed for analysing only patient files with all relevant data required for the Baveno classification.
The classification of patients based on dichotomisation of continuous biological parameters might be seen as an oversimplification. However, the cut-off values for the ESS score and blood pressure we used are well established and substantiated in that they relate to outcome. Dichotomous cut-offs were deliberately chosen to make the Baveno system intuitive and accessible in the clinical routine. It may also be extended at a later stage by the introduction of parameters such as hypoxic load and/or therapeutic recommendations.
The ESADA database has its greatest strength in the baseline data while follow-up data are available only for a subgroup of patients. The validation of the Baveno classification on long-term outcome has to remain limited. Therefore, the system will require prospective evaluation of a large unselected population based on both patient-related outcome parameters, morbidity and mortality. Nevertheless, the ESS, the hypoxic burden, the blood pressure, and the treatment compliance between 24 and 36 months in a subgroup of this study may be considered as a surrogate of the outcome.
We are aware that the interpretation of the compliance may underlie a selection bias due to loss of noncompliant patients. Nevertheless, the data demonstrate that sufficient compliance is associated with cardiovascular improvement in those with severe comorbidities and a substantial improvement of severe symptoms.
Conclusions
The Baveno classification system is probably superior to the traditional OSA classification based on AHI as it combines patient-related parameters of symptomatology on one hand and prognostic parameters on the other. It integrates findings of several recent cluster analyses. Furthermore, the scheme is easily applicable in clinical practice as it uses simply available, but reliable data. Using the system for therapeutic decisions, it may avoid unnecessary treatments in patients with moderate-to-severe OSA, but without symptoms or comorbidities, and missing treatments in symptomatic or comorbid OSA patients with low AHI. However, these findings require further investigation in prospective studies.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00928-2020.SUPPLEMENT
Footnotes
This article has supplementary material available from openres.ersjournals.com.
Conflict of interest: W.J. Randerath reports speaking fees and travel grants from Philips Respironics, Heinen und Löwenstein, ResMed, Bioprojet, Bayer Vital and Vanda Pharma outside the submitted work.
Conflict of interest: S. Herkenrath has nothing to disclose.
Conflict of interest: M. Treml has nothing to disclose.
Conflict of interest: L. Grote reports grants from Bayer, the Philips Respironics Foundation and the ResMed Foundation for the ESADA network during the conduct of the study; and nonfinancial and other support from Itamar Medical, ResMed, Philips, AstraZeneca and Breas outside the submitted work. In addition, L. Grote has a patent on sleep apnoea therapy licensed.
Conflict of interest: J. Hedner reports grants from Bayer AG, the European Respiratory Society (for database maintenance) and Desitin GmbH outside the submitted work; in addition, J. Hedner has a patent issued on pharmacological therapy of OSA.
Conflict of interest: M.R. Bonsignore has nothing to disclose.
Conflict of interest: J.L. Pépin grants and research funds from the Air Liquide Foundation, Agiradom, AstraZeneca, Fisher and Paykel, Mutualia, Philips, ResMed, and Vitalaire; and fees from Agiradom, AstraZeneca, Boehringer Ingelheim, Jazz Pharmaceutical, Night Balance, Philips and ResMed.
Conflict of interest: S. Ryan has nothing to disclose.
Conflict of interest: S. Schiza has nothing to disclose.
Conflict of interest: J. Verbraecken reports an educational grant and an advisory board fee from ResMed; a consultancy fee from Philips; lecture fees from Sanofi and Agfa-Gevaert; an educational grant and an advisory board fee from Bioprojet; an educational grant from and study participation for Jazz Pharmaceutics; an educational grant from AirLiquide; a lecture fee from Springer; an educational grant from Westfalen Medical; an educational grant and a lecture fee from SomnoMed; educational grants from Vivisol, Total Care, Medidis, Fisher & Paykel, Wave Medical, OSG, Mediq Tefa, NightBalance and Heinen & Löwenstein; lecture fees from AstraZeneca; and educational grants from Accuramed, Bekaert Deslee Academy and UCB Pharma, all outside the submitted work.
Conflict of interest: W.T. McNicholas has nothing to disclose.
Conflict of interest: A. Pataka has nothing to disclose.
Conflict of interest: P. Sliwinski has nothing to disclose.
Conflict of interest: Ö.K. Basoglu has nothing to disclose.
- Received December 10, 2020.
- Accepted December 22, 2020.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










