





Abstract
Numerous oral indigenous microorganisms are constantly introduced into the stomach via the laryngopharynx, and a portion of these microorganisms irregularly reaches the lower airways and lungs. This study investigated the association between airflow limitation and the status of tongue microbiota, which is a primary source of ingested oral bacterial populations.
The study population consisted of 484 community-dwelling adults aged 70–80 years inhabiting Hisayama town, Japan, who underwent a regular health examination including dental examination and spirometry test in 2016. The bacterial density and composition of their tongue microbiota were determined using a previously used 16S rRNA gene to understand their relationship with oral health conditions. The present cross-sectional study compared the tongue microbiota status between elderly individuals with airflow limitation and those with normal airflow.
The total bacterial density of the tongue microbiota of individuals with airflow limitation was significantly higher than that of individuals with normal airflow. Logistic regression analysis demonstrated that a high-biomass tongue microbiota was significantly associated with airflow limitation after adjustment for smoking intensity and other covariates (adjusted OR 1.61, 95% CI 1.01–2.60). Of the predominant commensals, higher amounts of Prevotella melaninogenica and Actinomyces odontolyticus were associated with a higher prevalence of airflow limitation.
These results indicate that increased bacterial burden in the tongue microbiota is associated with a higher prevalence of airflow limitation.
Abstract
Bacterial enrichment in the tongue microbiota is associated with airflow limitation characterising COPD in community-dwelling elderly adults https://bit.ly/36qMf6G
Introduction
The oral cavity, an alternate entrance for inhaled air, is densely colonised by a diverse array of indigenous microbial populations. These numerous microbes are constantly introduced with saliva and diverted into the oesophagus by the epiglottis, a flap of elastic cartilage in the laryngopharynx [1]. However, a portion of these organisms also reach the lower airway and lungs via microaspiration and mucosal dispersion [2]; the lungs are not sterile, and normally harbour diverse microbes mainly derived from the oral cavity [1, 3]. This evidence suggests the possibility that increased and/or dysbiotic oral microbiota predisposes the lungs to chronic airway inflammation, leading to airflow limitations [4].
The dorsum of the tongue is colonised by numerous indigenous microorganisms constituting a unique and stable microbiota, which is a primary source of oral bacterial population ingested with saliva, among microbial communities formed on various oral niches [5–8]. We previously determined the amount and composition of the tongue microbiota of community-dwelling elderly adults who underwent a regular health examination in Hisayama town, Fukuoka, Japan, and characterised the variation according to different oral health conditions [9]. Most participants also received a spirometry test during the health examination. Thus, the present cross-sectional study investigated the relationship between airflow limitation and the tongue microbiota status of elderly individuals by utilising data on their tongue microbiota and pulmonary function. The biomass and composition of the tongue microbiota was compared between individuals with airflow limitation and those with normal airflow, and the bacterial taxa associated with airflow limitation were explored.
Materials and methods
Ethics statement
All participants understood the nature of the study and provided written informed consent. The Ethics Committee of Kyushu University approved the study design and the procedure for obtaining informed consent (reference number: 28–31). All experiments were performed in accordance with the approved guidelines.
Study population
A population-based prospective cohort study has been conducted in the town of Hisayama since 1961, and adult residents undergo regular health examinations [10]. In 2016, 508 residents aged 70–80 years underwent dental examination and the collection of tongue microbiota in the regular health examination; this included anthropometric measures, urinalysis, blood tests and spirometry tests, from June to August. All measurements for each individual were performed on the same day. We determined the microbial amount and composition of the tongue microbiota of 506 residents and investigated the relationship between tongue microbiota status and oral health condition in a previous study [9]. Of these participants, 487 underwent a spirometry test after the dental examination. After excluding three individuals due to missing data in relevant covariates, 484 individuals were analysed in this study (figure 1).

Flow diagram of study participant selection.
Dental examination and tongue microbiota collection
The details of the dental examination in the annual health examination were described previously [11]. Number of teeth and visible tooth decay were evaluated by visual inspection. Periodontitis severity was classified according to the suggested CDC and AAP case definitions for periodontitis surveillance [12]. Oral hygiene status or accumulation of dental plaque was evaluated according to the Silness and Löe [13] plaque index. Following dental examination, tongue coating samples were collected from a circular area with a diameter of 15 mm on the centre of the tongue dorsum, by using an electric toothbrush with a 3-s vibration, as a sampling device, as described previously [9].
Tongue microbiota analysis
Microbial density of the tongue microbiota was determined in our previous study [9]. In brief, quantitative PCR was performed using a QuantiFast SYBR green PCR kit (Qiagen, Hilden, Germany), which target V5 region of the 16S rRNA gene for total bacterial density and a fungal internal transcribed spacer 2 region of the rRNA operon for total fungal density, respectively.
The dataset on bacterial composition of the tongue microbiota was also constructed in our previous study [9], based on the V1–V2 region of 16S rRNA gene using Ion PGM (Thermo Fisher Scientific, Waltham, MA, USA). Similar sequences were assigned into operational taxonomic units (OTUs) using UPARSE [14], with a minimum pairwise identity of 97%. The taxonomy of representative sequences was determined using BLAST against 889 oral bacterial 16S rRNA gene sequences in the Human Oral Microbiome Database [15] with ≥98.5% identity. The relative abundance of each OTU were calculated following rarefaction with a depth of 5000 reads per sample using R. The sequence data utilised in this study were available in the DDBJ Sequence Read Archive as accession numbers DRA006979–DRA006983.
Spirometry test and airflow limitation definition
Spirometry evaluating expiratory airflow limitation was performed in accordance with the guidelines of the Japanese Respiratory Society (Committee of Pulmonary Physiology in Japanese Respiratory Society, 2004) without a use of bronchodilators, according to the protocols as described previously [16]. Airflow limitation was defined according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) fixed cut-off criterion for COPD (forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) <70%) [17].
Assessment of other covariates
Each participant completed a self-administered questionnaire covering smoking habits and alcohol intake. Body weight and height were measured, and body mass index (BMI) (kg·m−2) was calculated. Participants with any exercise habits were defined as physically active individuals. Alcohol intake status was divided into two categories: current or previous drinkers and participants who never drank alcohol. Smoking intensity was classified based on the Brinkman Index that is the number of cigarette smoked per day multiplied by the number of years of smoking [18], into nonsmokers (Brinkman Index=0), moderate smokers (0< Brinkman Index <400) and heavy smokers (Brinkman Index ≥400).
Statistical analysis
R (ver. 3.5.2) was used to perform all statistical analyses. Student's t-test, Chi-squared test and Fisher's exact test were used for comparison of general and oral conditions between the participants with normal airflow and the ones with airflow limitation, for continuous data and binomial data, respectively. A multiple logistic regression analysis was carried out to investigate the relationship between the presence of airflow limitation and prevalence of high bacterial biomass following binomial logistic regression. In addition, the total bacterial biomass was incorporated into the model as a continuous value after log transformation, which allows distribution to be normalised and reduces heterogeneity in variable variance. The unweighted and weighted UniFrac metric [19] was used to determine the dissimilarity between any pair of bacterial communities. Permutational multivariate analysis of variance (PERMANOVA) was used to assess the relationship between the microbiota composition and lung function. Discriminant OTUs of individuals with or without airflow limitation were explored using the Linear discriminant analysis Effect Size (LEfSe) approach [20]. Community type analysis used for enterotype clustering [21] were used for classification of tongue microbiota composition. The amounts of 21 predominant (mean relative abundance >1%) species-level OTUs was calculated by multiplying total bacterial density and the relative abundance of each taxon. Bacterial amount of each OTU was compared between participants with and without airflow limitation, using Wilcoxon rank-sum test. A multiple logistic regression analysis was carried out to investigate the relationship between the presence of airflow limitation and the bacterial amount of OTUs. The predominant taxa were not detected in some individuals in the bacterial compositional analysis because of the low relative proportion below the detection threshold (0.02%). Even though 0.01% of the 108 microbiota (104 copies) existed, their abundances had to be regarded as 0, resulting in discontinuity of the values. In addition, the OTU abundance threshold of each OTU varied depending on the total bacterial density of each microbiota. Therefore, the abundance of low-abundance OTUs was partially reliable in this study. Thus, we did not obtain a continuous value of OTU abundance, and therefore stratified them into quartile groups for incorporation into the multivariate model.
Results
The study population consisted of 484 community-dwelling elderly individuals (218 male and 266 female) residing in Hisayama town, aged between 70 and 80 years, who underwent a health examination including dental examination and spirometry testing in 2016 (figure 1). We previously determined the microbial amount and bacterial composition of their tongue microbiota, and characterised the variation according to different oral health conditions [9]. The present cross-sectional study utilised tongue microbiota data and results of their spirometry test conducted on the same day during the general health examination and investigated the relationship between tongue microbiota status and lung function.
Of the 484 elderly individuals, airflow limitation defined on the basis of pre-bronchodilator FEV1/FVC value <70%, was observed in 100 (20.6%) individuals. The general and clinical conditions are described in table 1. These individuals had a significantly older age, lower BMI, and comprised fewer women and non-smokers compared with individuals with normal airflow. No significant differences were observed in dental and periodontal conditions, whereas the total bacterial density of the tongue microbiota in individuals with airflow limitation was significantly higher than in those with normal airflow.
General and oral conditions of participants with and without airflow limitation
No significant difference was observed between the individuals with high- and low-biomass tongue microbiota in general and oral conditions, except for the presence of airflow limitation (table S1). A logistic regression analysis showed a significant relationship between airflow limitation and a high-biomass tongue microbiota in a univariate model, along with age, sex, BMI and smoking intensity (table 2). A multivariate model incorporating these covariates demonstrated that a high-biomass tongue microbiota was significantly associated with the presence of airflow limitation, independent of confounding factors, including smoking intensity (adjusted OR 1.61, 95% CI 1.01–2.60). Bacterial density of tongue microbiota was significantly associated with airflow limitation in a multivariate model when incorporating it as a continuous variable (adjusted OR 1.80, 95% CI 1.01–3.18) (table S2). A significant relationship between bacterial density and airflow limitation was also observed in a multivariate model when 32 current smokers were excluded from the analysis (adjusted OR 1.81, 95% CI 1.09–3.04) (table S3).
Odds ratio for airflow limitation in logistic regression analysis
We further investigated the tongue microbiota composition associated with airflow limitation based on the results of the 16S rRNA gene sequencing analysis. However, no significant differences were observed in the overall bacterial community structures of tongue microbiota between the individuals with airflow limitation, and those with normal airflow in both unweighted and weighted UniFrac analyses (p=0.25 and p=0.06, respectively, PERMANOVA) (figure 2). Community type analysis used for enterotype clustering [21] classified the tongue microbiota composition into four types, but no significant difference was observed in the prevalence of airflow limitation (table S4). On the other hand, the linear discriminant analysis effect size indicated that the relative abundances of some predominant taxa such as Neisseria flavescens and P. melaninogenica were different in the individuals with airflow limitation, and those with normal airflow (table S5).

A principal coordinate analysis plot showing similarity relationships between bacterial composition of the tongue microbiota from 484 participants using unweighted (a) and weighted (b) UniFrac metric. The points corresponding to the participants with and without airflow limitation are depicted in different colours. The ellipses cover 67% of the samples belonging to each group.
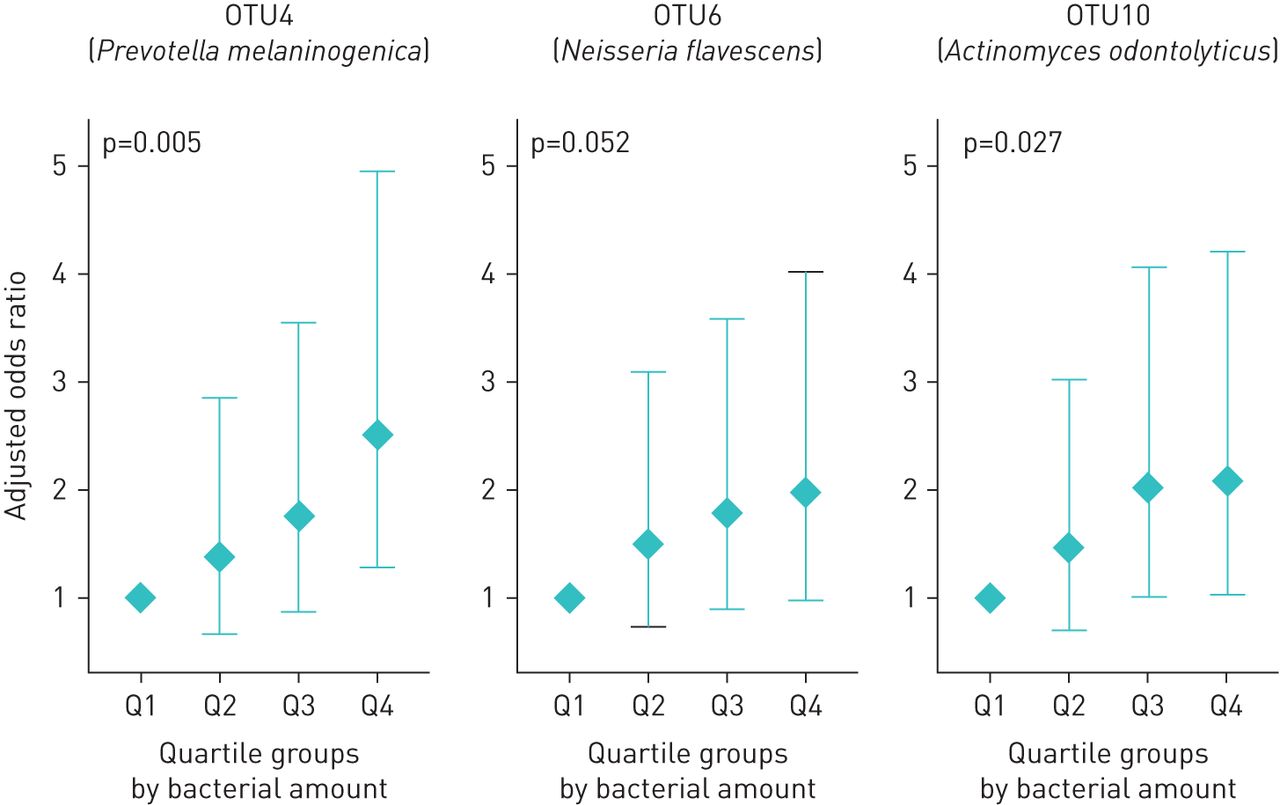
To identify the bacterial taxa associated with airflow limitation, we calculated the amounts of 21 predominant (mean relative abundance >1%) species-level OTUs by multiplying the total bacterial density and the relative abundance of each taxon. Of these, the amounts of three OTUs corresponding to P. melaninogenica, N. flavescens, and A. odontolyticus were notably higher in individuals with airflow limitation, than in those with normal airflow (p<0.01, Wilcoxon Rank Sum test) (table S6). The amounts of these OTUs were stratified into four categories based on the quartile values (quartile 1 to quartile 4) and incorporated into the multivariate model. The amounts of two of these OTUs (OTU4 and OTU10) were positively related to the presence of airflow limitation, after adjustment for smoking intensity and other covariates in logistic regression models with a significant linear relationship (p for trend=0.005, and 0.027, P. melaninogenica, and A. odontolyticus, respectively) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Adjusted odds ratio of bacterial amounts of three predominant operational taxonomic units (OTUs) for airflow limitation in logistic regression models. The bacterial amounts of each taxon were calculated by multiplying total bacterial density and the relative abundance of each OTU, and were classified into four categories based on quartile values (quartile 1 to quartile 4). A logistic regression model was constructed for each OTU for adjusting the effects of age, sex, body mass index, smoking intensity, alcohol intake, presence of decayed teeth and periodontal condition.
Discussion
This study demonstrated that bacterial density of the tongue microbiota was significantly higher in the community-dwelling elderly individuals with airflow limitation than in those with normal airflow (table 1). Logistic regression analysis revealed that a high-biomass tongue microbiota, especially higher amounts of P. melaninogenica and A. odontolyticus, were significantly associated with airflow limitation, after adjustment for smoking intensity and other covariates (table 2 and figure 3). These results indicate that increased bacterial burden in the tongue microbiota is associated with a higher prevalence of airflow limitation.
This study indicated that P. melaninogenica, with the highest biomass in the tongue microbiota (table S6), is a species associated with airflow limitation, along with some other predominant taxa (figure 3). Oral Prevotella spp. is commonly detected in the lung microbiota [2], indicating that the aspirated Prevotella spp. can reach and colonise the lower airway and lungs. Furthermore, Segal et al. [22] demonstrated that the enrichment of Prevotella spp. in the lung microbiota was associated with enhanced subclinical lung inflammation, including enhanced expression of inflammatory cytokines and elevated Th17 lymphocytes. It is reasonable to assume that the aspirated oral taxa, including Prevotella spp., are associated with an increased host response in the lower airway and lungs. On the other hand, oral commensal taxa have been identified in both diseased and healthy lungs, suggesting that exposure to oral-derived microbiota during health is a part of the homeostatic processes that regulate pulmonary inflammatory responses [1]. Nevertheless, considering that increased bacterial burden in the airways was reported to be associated with FEV1 decline [23], higher amounts of aspirated oral commensals would result in overstimulation of the host inflammatory response in the airway, and predispose the airway to chronic inflammation.
Although the association of poor oral health with COPD has been indicated in earlier studies [24–27], the studies have mostly focussed on periodontitis. Tongue microbiota is separate and distinct from the microbiota on teeth and gingiva [5, 6, 8, 28], and its total bacterial biomass is independent of teeth and periodontal conditions, as shown in our previous study [9] and confirmed in this study (table S1 and figure S1). The two taxa identified in this study to be associated with airflow limitation were recognised as tongue coating-specific bacteria, which localised on the tongue dorsum, and not in the supra- and sub-gingival plaque [28]. In addition, considering that its significant relationship with airflow limitation remained after adjustment for covariates, including periodontal conditions (table 2 and figure 3), increased bacterial burden of the tongue microbiota is associated with a higher risk of airflow limitation in a distinct manner from periodontitis.
Our cross-sectional data only demonstrated the association between bacterial enrichment of tongue microbiota and airflow limitation. It is possible that individuals with airflow limitation might be susceptible to accumulation of the tongue microbiota. Further longitudinal studies with information about the lower airway and lung microbiota are required to clarify this causal relationship. In addition, although the tongue microbiota is a relatively stable microbial community [8], we could not omit the possibility that the tongue microbiota of some participants might temporarily vary from their normal conditions during sample collection as the samples were collected at a single time point. Our study also lacks information on antibiotic use at sampling, which could temporarily decrease the bacterial burden and alter the microbiota composition. Future studies also require multiple sampling and detailed information on treatments and medication use. Information on dysphagia, gastric reflux and dry mouth would also be helpful in evaluating the relationship more accurately. Our results also need to be confirmed in a younger population, although it would require a larger sample size due to a lower prevalence of clinically apparent airflow limitation. Bacteriological studies on the inflammatory potential of P. melaninogenica and A. odontolyticus is also needed.
Although the tongue microbiota is a more dominant source of bacterial population constantly ingested with saliva than dental plaque, its clinical significance has been underappreciated except for oral malodour [29] and aspiration pneumonia in frail, dysphagic elderly individuals [30]. This study indicates that a high-biomass tongue microbiota is significantly associated with a higher prevalence of airflow limitation characterising COPD, which is a major burden on public health. This study also supports the importance of the oral–lung axis, which has recently garnered increased attention [4, 31, 32]. Maintenance of healthy tongue microbiota might be beneficial as a preventive approach for airflow limitation.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00616-2020.SUPPLEMENT
Figure S1 00616-2020.figureS1
Acknowledgements
We thank the staff of the Division of Health and Welfare of the Hisayama Town Office for their cooperation in this study.
Footnotes
This article has supplementary material available from openres.ersjournals.com
Conflict of interest: T. Takeshita has nothing to disclose.
Conflict of interest: K. Matsumoto has nothing to disclose.
Conflict of interest: M. Furuta has nothing to disclose.
Conflict of interest: S. Fukuyama has nothing to disclose.
Conflict of interest: K. Takeuchi has nothing to disclose.
Conflict of interest: H. Ogata has nothing to disclose.
Conflict of interest: M. Asakawa has nothing to disclose.
Conflict of interest: S. Kageyama has nothing to disclose.
Conflict of interest: J. Hata has nothing to disclose.
Conflict of interest: T. Ninomiya has nothing to disclose.
Conflict of interest: H. Inoue has nothing to disclose.
Conflict of interest: Y. Yamashita has nothing to disclose.
Support statement: This study was supported in part by Japan Society for the Promotion of Science (JSPS) KAKENHI grants JP19H03863, JP19K22722 and JP16H05557 (to T. Takeshita), and JSPS grant JP20H03901 (to Y. Yamashita). Funding information for this article has been deposited with the Crossref Funder Registry.
- Received August 27, 2020.
- Accepted January 22, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










