





Abstract
Physiological phenotyping using daily home-based assessments reveals early improvement in load–capacity–drive imbalance following #AECOPD and feasibility of home parasternal electromyography measurement, which tracks symptoms, health status and spirometry https://bit.ly/3o6I0Ty
To the Editor:
Exacerbations of COPD remain a leading cause of emergency hospitalisations worldwide, and up to 28% of patients are readmitted within 30 days of discharge [1]. Recent analyses of more than 2.3 million COPD hospitalisations highlight the dynamic and time-dependent nature of readmission risk, which peaks within the first 72 h of discharge [2, 3]. Effective readmission prevention strategies remain elusive and recognition of re-exacerbations beyond daily symptom variability is challenging for both patients and clinicians. Promotion of transitional care services and 30-day readmission penalties implemented by policymakers worldwide have had limited impact [4]. Telemonitoring strategies incorporating symptom and vital observation monitoring (peripheral oxygen saturation (SpO2), heart rate, respiratory frequency) have consistently failed to demonstrate beneficial effects on hospitalisation risk [5]. Objective physiological monitoring has been explored using the forced oscillation technique. However, this also failed to prolong time to first hospitalisation [6].
Parasternal intercostal electromyography (EMGpara) is a noninvasive, effort-independent method of quantifying inspiratory muscle activity and may be used as a surrogate measure of neural respiratory drive. It has been used to evaluate load–capacity–drive imbalance of the respiratory muscle pump during COPD exacerbations, and inpatient measurements are sensitive to patient-reported and clinician-defined changes in clinical trajectory [7, 8]. In this study, we aimed to 1) conduct detailed physiological phenotyping of COPD exacerbation recovery using daily home-based measurements to elucidate mechanisms underpinning early readmission risk and 2) explore the feasibility of home EMGpara as a physiological biomarker of clinical trajectory to inform the design of effective transitional care strategies.
Consecutive patients admitted to a university hospital with a primary diagnosis of COPD exacerbation who were aged 40–80 years, did not require mechanical ventilation and had a body mass index (BMI) <35 kg·m−2 were enrolled. This prospective observational cohort feasibility study received ethical approval (18/LO/0157) and was registered prospectively (NCT03443505).
Assessments were performed within 16 h of hospitalisation, pre-discharge and daily at home for 30 days post-discharge. Home-based measurements were obtained during home visits conducted by one member of the research team (RFD). Symptoms were evaluated using the daily Exacerbations of Chronic Pulmonary Disease Tool (EXACT) [9] and modified Borg scale for breathlessness [10]). Physiological recovery was evaluated using daily measurement of heart rate, SpO2, respiratory rate and neural respiratory drive, quantified using EMGpara. EMGpara was measured with subjects in a seated position with the arms relaxed and supported to minimise tonic activity of adjacent chest wall musculature. Skin overlying the right and left second intercostal parasternal spaces and lateral aspect of the right clavicle was prepared using an abrasive gel (Nuprep Skin Prep Gel; Weaver and Company, Aurora, CO, USA) and alcohol wipe (Clinell, GAMA Healthcare, London, UK) prior to placement of wet-gel electrodes (Ambu Blue Sensor Q; Ambu, St Ives, UK), which were connected to bipolar and ground electrodes. Signals were amplified with a gain of 1000, band-pass filtered at 10–2000 Hz and AC-coupled prior to acquisition, and acquired using a 16-bit analogue-to-digital converter (Porti Physiological Amplifier; TMSi, Oldenzaal, the Netherlands). A nasal cannula (Intersurgical, Wokingham, UK) positioned in subjects' nares was connected to a differential pressure transducer (Pressure Sensor; TMSi) to aid identification of the respiratory cycle. Analogue-to-digital sampling was performed at 2 kHz and displayed on a laptop computer. At each home assessment, measurements were taken over 6 min of tidal breathing followed by sniff manoeuvres which were repeated until maximal volitional effort was achieved. For standardisation, home visits were conducted at the same time each day and EMGpara was measured before and after inhalation of patients' short-acting bronchodilator. Traces were analysed offline by converting raw EMGpara signals to root mean squared (RMS) using a moving window of 50 ms. RMS EMGpara peak values during tidal breathing were manually identified (mean EMGpara), normalised to the maximal volitional manoeuvre (EMGpara%max) and expressed as neural respiratory drive index (NRDI) (product of EMGpara%max and respiratory rate) [7, 8]. Standardised residuals (z-scores) were calculated using sex-specific normal values from healthy subjects [11]. Health-related quality of life (COPD Assessment Test (CAT) [12]) and handheld spirometry (forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), inspiratory capacity (IC) (EasyOne Diagnostic Spirometer; ndd Medical Technologies, Zurich, Switzerland)) were measured weekly.
Data are presented as mean±sem, median (interquartile range) and number (%; 95% CI). Data at successive time points were compared with repeated-measures ANOVA, with post hoc comparisons using Bonferroni correction. Linear mixed model (LMM) regression (adjusted for age, sex, BMI and annual exacerbation frequency) was used to analyse associations between EMGpara indices and other measured patient-reported and physiological parameters. Area under the curve (AUC) and coefficient of variation (CV) were used to analyse changes and variability in symptoms and EMGpara. Analyses were performed using SPSS Statistics (v26; IBM Corp, Armonk, NY, USA).
Between February 2018 and June 2019, 427 patients hospitalised with acute exacerbation of COPD were screened for eligibility and 29 (6%) were invited to participate. The most common reasons for ineligibility were age >80 years (n=92, 22%), need for acute mechanical ventilation (n=85, 20%) and having a home environment deemed unsafe for lone researcher visits (n=57, 13%). Six (21%) patients declined to participate and 23 (79%) were recruited, of whom four were withdrawn due to ineligibility, seven withdrew and 12 completed the study. Those who declined or withdrew cited the burden of daily home visits as their reason. The admission characteristics of those completing the schedule of assessments include age 68±2.6 years, 67% female, BMI 21.8±1.2 kg·m−2, FEV1 23% predicted (19–25% predicted), seven (58%) current smokers, 68±13 pack-years, annual exacerbation frequency (number of exacerbations in the 12 months preceding admission) 4±1, Charlson comorbidity index 4±1 (ischaemic heart disease in three (25%; 95% CI 0–50%) patients, cerebrovascular disease in two (17%; 95% CI 8.3–33.3%), hypertension in three (25%; 0–50%), type 2 diabetes mellitus in one (8.3%; 0–25%)), duration of hospitalisation 2 (1.25–4.5) days. Regular COPD medications included as-required short-acting β2-agonist (n=12, 100%), long-acting antimuscarinic (LAMA) (n=7, 58%; 95% CI 41.7–75.0%), combined inhaled corticosteroid (ICS) and long-acting β2-agonist (LABA) (n=9, 75%; 95 CI 58.3–91.7%), combination ICS–LABA–LAMA (n=1, 8%; 95% CI 0–25.0%), oral mucolytic (n=6, 50%; 95% CI 25.0–75.0%) and prophylactic macrolide antibiotic (n=2, 17%; 95% CI 8.3–33.3%). Patients received standardised acute medical therapy, including nebulised bronchodilation (n=12, 100%), course of antibiotic and corticosteroid (n=9, 75%; 95% CI 58.3–91.7%), corticosteroid alone (n=3, 25%; 95% CI 8.3–41.7%) and outpatient follow-up.
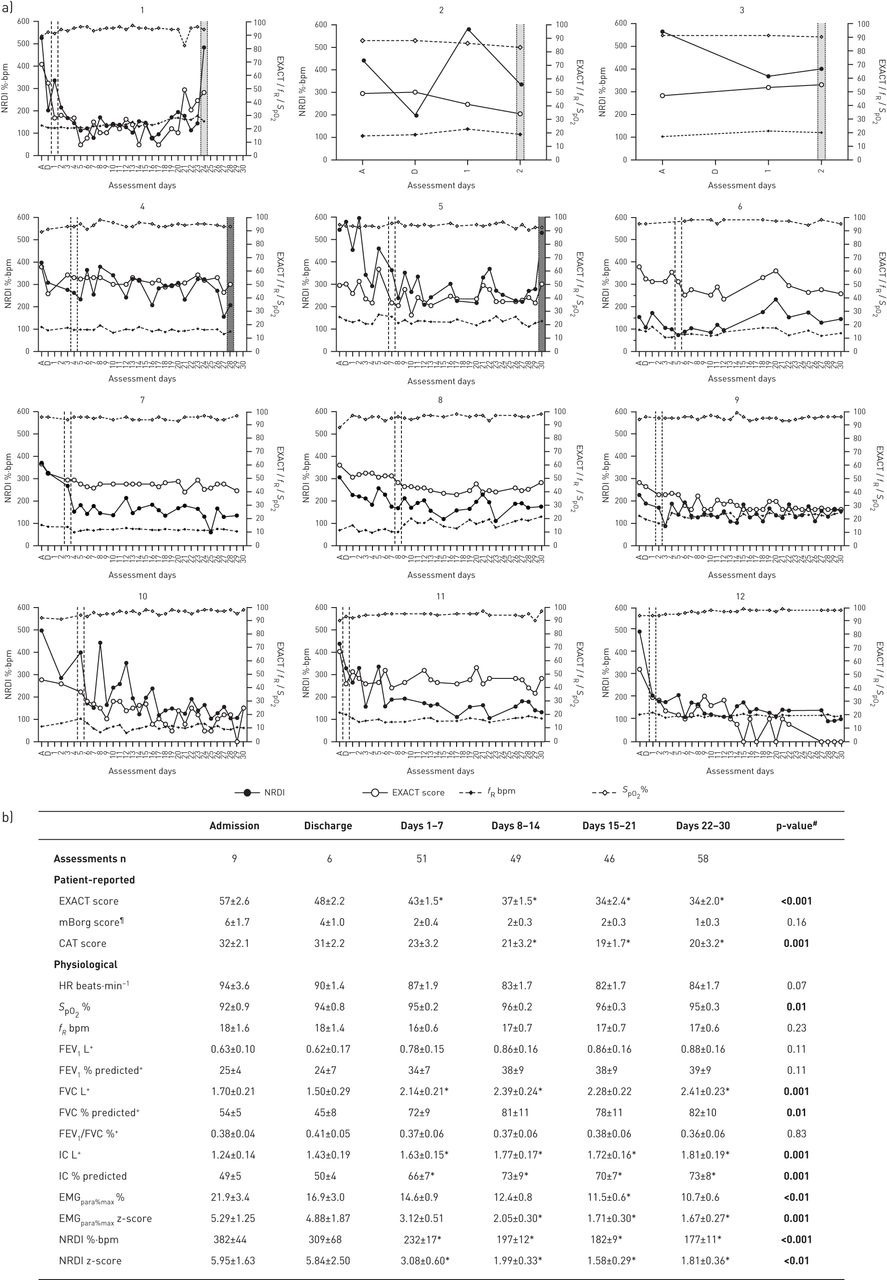
232 (79%) of a possible 292 home visits were performed. There was 100% adherence to EMGpara measurement. 457 traces were recorded; 100% were of analysable quality. Three (25%) patients were readmitted within 30 days of hospital discharge; two (17%) within 48 h. 12-month readmission rate and mortality were 75% and 42%, respectively. Patient-reported and physiological outcomes during 30-day follow-up are reported in figure 1. Improvements in EXACT score, FVC, IC and NRDI were observed between admission and week 1 post-discharge. 10 patients reached EXACT-defined recovery (sustained fall of ≥9 points from peak score), which corresponded to a 144±21%·bpm reduction in NRDI. In those not experiencing 30-day re-exacerbations, EXACT and CAT scores, SpO2, hyperinflation (FVC and IC) and neural respiratory drive indices (EMGpara%max and NRDI) improved between admission and day 30 post-discharge.

{kind=link}
a) Daily measurements of neural respiratory drive index (NRDI) and Exacerbations of Chronic Pulmonary Disease Tool (EXACT) score, respiratory rate (fR) and peripheral oxygen saturation (SpO2) at admission (A), discharge (D) and at home for 30-days post-discharge or until hospital readmission (1–30 days) for each patient (1–12). Dashed lines indicate the day of EXACT-defined recovery, if reached (9-point reduction from peak score sustained for 7 days [9]), dotted lines indicate a day of healthcare utilisation, with light grey bars representing hospital readmission (subjects 1–3) and dark grey bars representing non-readmission re-exacerbation (subjects 4–5). b) Trajectory of patient-reported and physiological outcomes in non-readmitted patients (n=9). Data are presented as mean±sem, unless otherwise stated. Bold type represents statistical significance. bpm: breaths per min; mBorg: modified Borg scale for breathlessness; CAT: COPD Assessment Test; HR: heart rate; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; IC: inspiratory capacity; EMGpara%max: normalised mean parasternal electromyography. #: repeated-measures ANOVA; ¶: n=6; +: n=1 unable to perform pre-discharge spirometry due to breathlessness. *: p<0.05 compared to admission, post hoc comparisons with Bonferroni correction were performed if a significant f ratio was obtained by one-way repeated-measures ANOVA across all time points.
Adjusted univariate LMM analysis demonstrated that NRDI was positively associated with patient-reported outcomes (total EXACT score (estimate of fixed effect 3.91, 95% CI 2.79–5.03; p<0.001), EXACT subdomains of breathlessness (estimate 2.40, 95% CI 1.76–3.05; p<0.001), cough and sputum (estimate 1.60, 95% CI 0.84–2.37; p<0.001) and chest symptoms (estimate 2.02, 95% CI 1.19–2.85; p<0.001), CAT score (estimate 2.56, 95% CI 0.47–4.65; p=0.02)) and heart rate (estimate 2.25, 95% CI 1.13–3.37; p<0.001), and inversely associated with SpO2 (estimate −11.58, 95% CI −16.92 to −6.23; p<0.001), FEV1 % predicted (estimate −1.87, 95% CI −3.62 to −0.12; p=0.04), FVC % predicted (estimate −1.36, 95% CI −2.29 to −0.44; p=0.01) and IC % predicted (estimate −1.26, 95% CI −2.29 to −0.23; p=0.02). Associations were present between the coefficient of variation for NRDI and total EXACT score (R2=0.39, p=0.03) and the EXACT breathlessness subdomain (R2=0.41, p=0.03). Associations between change and variability of NRDI and symptoms were strongest among the five patients experiencing 30-day re-exacerbations, in whom AUC for NRDI predicted AUC of total EXACT score (R2=0.94, p<0.01) and EXACT breathlessness (R2=0.94, p<0.01) and coefficient of variation for NRDI predicted coefficient of variation of total EXACT score (R2=0.98, p=0.001) and EXACT breathlessness (R2=0.94, p<0.01).
This study provides detailed novel insights into the close relationship between neural respiratory drive and routinely measured patient-reported and physiological parameters during recovery from severe COPD exacerbations. Furthermore, these data demonstrate that physiological recovery begins soon after hospital discharge, with improvements in hyperinflation (IC) and neural respiratory drive (EMGpara) reflecting early resolution of load–capacity–drive imbalance, with corresponding improvements in symptoms. Finally, home EMGpara measurement has been shown to be feasible to perform and tracks symptoms, health-related quality of life, peripheral oxygenation, heart rate, spirometry and IC during exacerbation recovery.
By day 30 post-discharge, three out of 12 patients were readmitted, two of whom were readmitted within 48 h of discharge, consistent with international data [2, 3]. Physiological phenotyping revealed improvements in IC, EMGpara indices and symptoms within 7 days of discharge and stability of FEV1/FVC and respiratory rate. The demonstrated trajectory of improvement indicates that the early physiological recovery observed is a consequence of improved expiratory flow, resolution of hyperinflation and enhanced operating lung volumes, consistent with studies evaluating patients at later stages of exacerbation recovery [13, 14]. Reasons for 30-day readmissions are multifactorial, with risk factors including annual exacerbation frequency, comorbidities and hospital length of stay [15, 16]. We propose that reported reductions in readmission risk immediately post-discharge are partially attributable to physiological recovery, involving improved expiratory airflow and reduced neural respiratory drive, perceived by patients as improved breathlessness [2, 3].
These data also demonstrate that home EMGpara measurements track COPD symptoms, health-related quality of life, spirometry and IC following hospitalisation with an exacerbation of COPD, and the relationship appears enhanced in those experiencing 30-day re-exacerbation. Measurement of EMGpara was found to be feasible and well-tolerated at home, as demonstrated by high adherence to daily measurements and consistent capture of analysable signals. This simple, effort-independent and non-aerosol-generating technique could be incorporated into existing community-based follow-up services to facilitate objective assessment of load–capacity–drive imbalance during exacerbation recovery and complement clinical evaluation and patient-reported outcomes. No home-based post-discharge patient-reported or physiological measure that predicts 30-day readmission has yet been identified [5, 6, 9, 17]. Future prospective validation is required to evaluate the clinical utility of EMGpara, either in isolation or in combination with conventional clinical measures, to predict re-exacerbation, facilitate early treatment and potentially avoid 30-day readmission. If found to be a sensitive physiological biomarker of re-exacerbation and readmission, translation of home EMGpara from the research environment to clinical application may be facilitated through equipment simplification, integration of a validated scoring algorithm to circumvent the need for manual scoring, training of nonmedical clinical staff and identification of signal thresholds that trigger clinical alerts [18].
Generalisability of our data is limited by the small sample, comprised predominantly of patients with very severe COPD who were willing to accept daily home-based assessments. Physiological evaluation of exacerbation recovery is notoriously challenging to conduct due to patient reluctance to attend repeated clinical assessments and perform forced respiratory manoeuvres during recovery [19]. Unlike previous studies, which have missing data and comparable sample sizes [13, 14], we mitigated loss to follow-up by using home-based assessments and achieved 100% adherence to EMGpara measurement.
Daily home-based monitoring of COPD patients following hospitalisation with an exacerbation reveals improvements in symptoms, hyperinflation and neural respiratory drive within the first week of discharge, indicating early resolution of load–capacity–drive imbalance. These patients are at high risk of 30-day readmission, and the immediate post-discharge period represents a window of opportunity to identify and manage patients failing to recover. Home parasternal electromyography is a feasible surrogate measure of neural respiratory drive that tracks symptoms, health-related quality of life, peripheral oxygenation, heart rate, spirometry and inspiratory capacity. It thus yields potential as an objective physiological biomarker of recovery and its utility in the transitional care setting is the focus of ongoing research.
Acknowledgements
We wish to thank the integrated respiratory team at Guy's and St Thomas’ Hospital NHS Foundation Trust for their assistance in identifying hospitalised COPD patients.
Footnotes
This study is registered at www.clinicaltrials.gov with identifier number NCT03443505. Individual participant data that underlie the results reported in this article will be made available following deidentification upon reasonable request to the corresponding author beginning 3 months and ending 5 years following article publication, to researchers who provide a methodologically sound proposal (upon approval of an internal commission) to achieve aims in the approved proposal for scientific purposes following the signing of a data sharing agreement.
Ethical approval: This study was approved by the London–Westminster Research Ethics Committee (18/LO/0157) and registered as a prospective observational cohort study (NCT03443505).
Author contributions: N. Hart and P.B. Murphy designed the study. R.F. D'Cruz acquired and analysed the data, and prepared the first draft of the manuscript. A. Douiri provided statistical support. All authors contributed to revising the manuscript for important intellectual content and approving the final version of the manuscript. N. Hart, P.B. Murphy and R.F. D'Cruz take responsibility for the accuracy and integrity of the data.
Support statement: R.F. D'Cruz was funded by the National Institute for Health Research to conduct this study (NIHR-INF-0415 and DRF-2018-11-ST2-037). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: R.F. D'Cruz reports a Clinical Training Fellowship and Doctoral Research Fellowship (NIHR-INF-0415 and DRF-2018-11-ST2-037) from the National Institute for Health Research during the conduct of the study.
Conflict of interest: E-S. Suh reports grants to his institution and fees for CPD approved activity from Philips Research outside the submitted work.
Conflict of interest: G. Kaltsakas has nothing to disclose.
Conflict of interest: A. Dewar has nothing to disclose.
Conflict of interest: N.M. Shah reports grants from Breas, with the funds held and managed by Guy's and St Thomas’ NHS Foundation Trust, outside the submitted work.
Conflict of interest: R. Priori is an employee of Philips Research.
Conflict of interest: A. Douiri has nothing to disclose.
Conflict of interest: L. Rose has nothing to disclose.
Conflict of interest: N. Hart reports an unrestricted grant for the OPIP Trial from Philips Respironics, nonfinancial support for development of the Myotrace technology from Philips Respironics RT Meeting (Myotrace), and unrestricted research grants for the HoT-HMV Trial from RESMED and Philips Respironics, outside the submitted work; in addition, he has patents for Myotrace issued in Europe and pending in the USA. His research group has received unrestricted grants (managed by Guy's and St Thomas’ Foundation Trust) from Philips and RESMED. Philips are contributing to the development of the Myotrace technology.
Conflict of interest: P.B. Murphy reports grants to his institution and fees for CPD approved activity from Philips, ResMed, F&P and Electromedical, personal fees for an advisory board from Santhera, and grants to his institution from GSK, outside the submitted work.
- Received September 29, 2020.
- Accepted January 15, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










