





Figures
- FIGURE 1
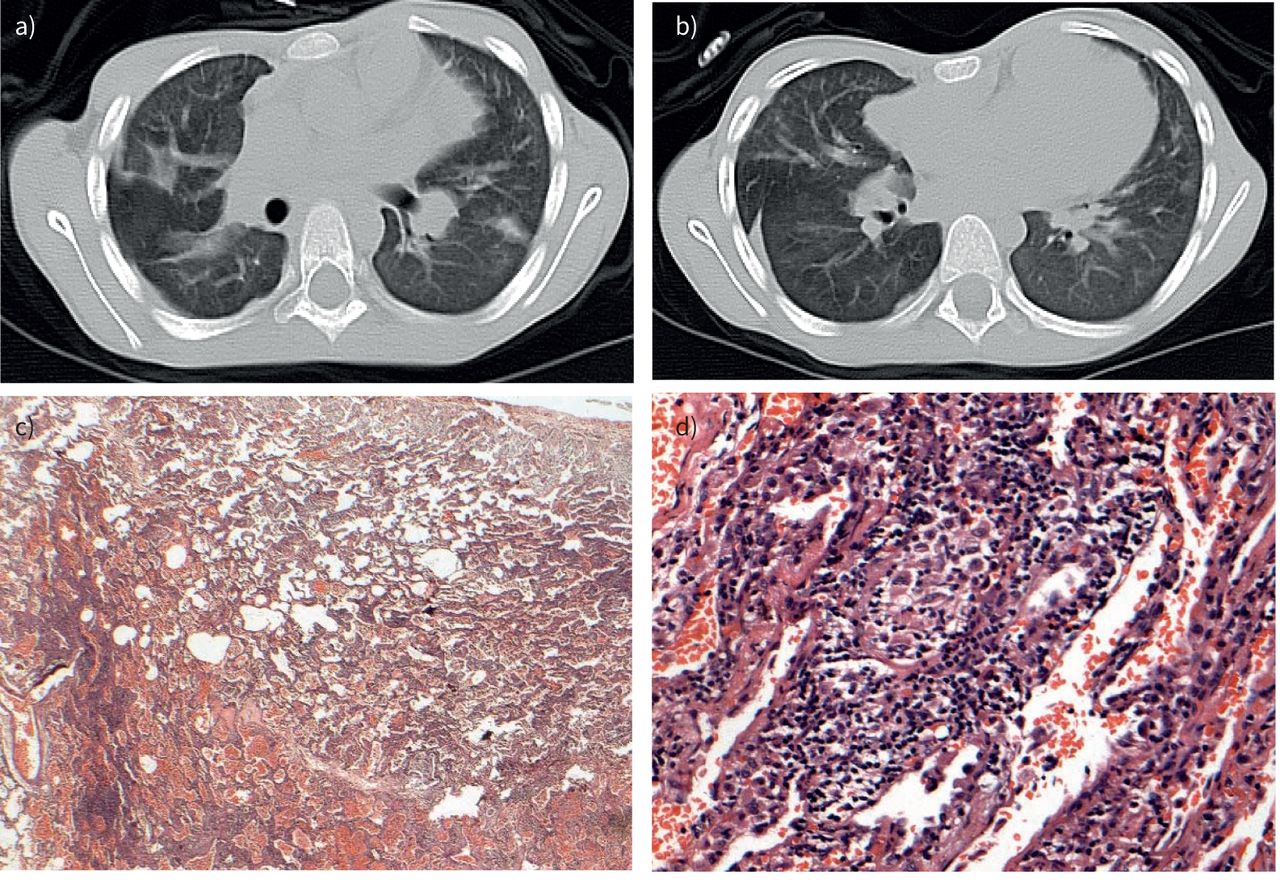
Subject 1: 9-year-old male referred with possible diagnosis of childhood interstitial and diffuse lung disease. He complained of recurrent attacks of dyspnoea and dry cough. He had a strong history of exposure to birds. On presentation, he was tachypnoeic and hypoxic (oxygen saturation 88% at rest in room air). He had marked failure to thrive with first-degree clubbing, and auscultation revealed widespread fine crepitations. Echocardiography showed dilated right side with pulmonary hypertension. a) Axial computed tomography shows bilateral scattered subsegmental consolidative patches associated with few scattered atelectatic bands; b) interlobular and fissural thickening; c) bronchocentric chronic inflammation (low power); d) small poorly formed granuloma (high power) (haematoxylin and eosin c) ×20, d) ×200). Overall, the features are consistent with hypersensitivity pneumonitis. There was a significant clinical improvement on elimination of bird exposure and systemic steroids.
- FIGURE 2
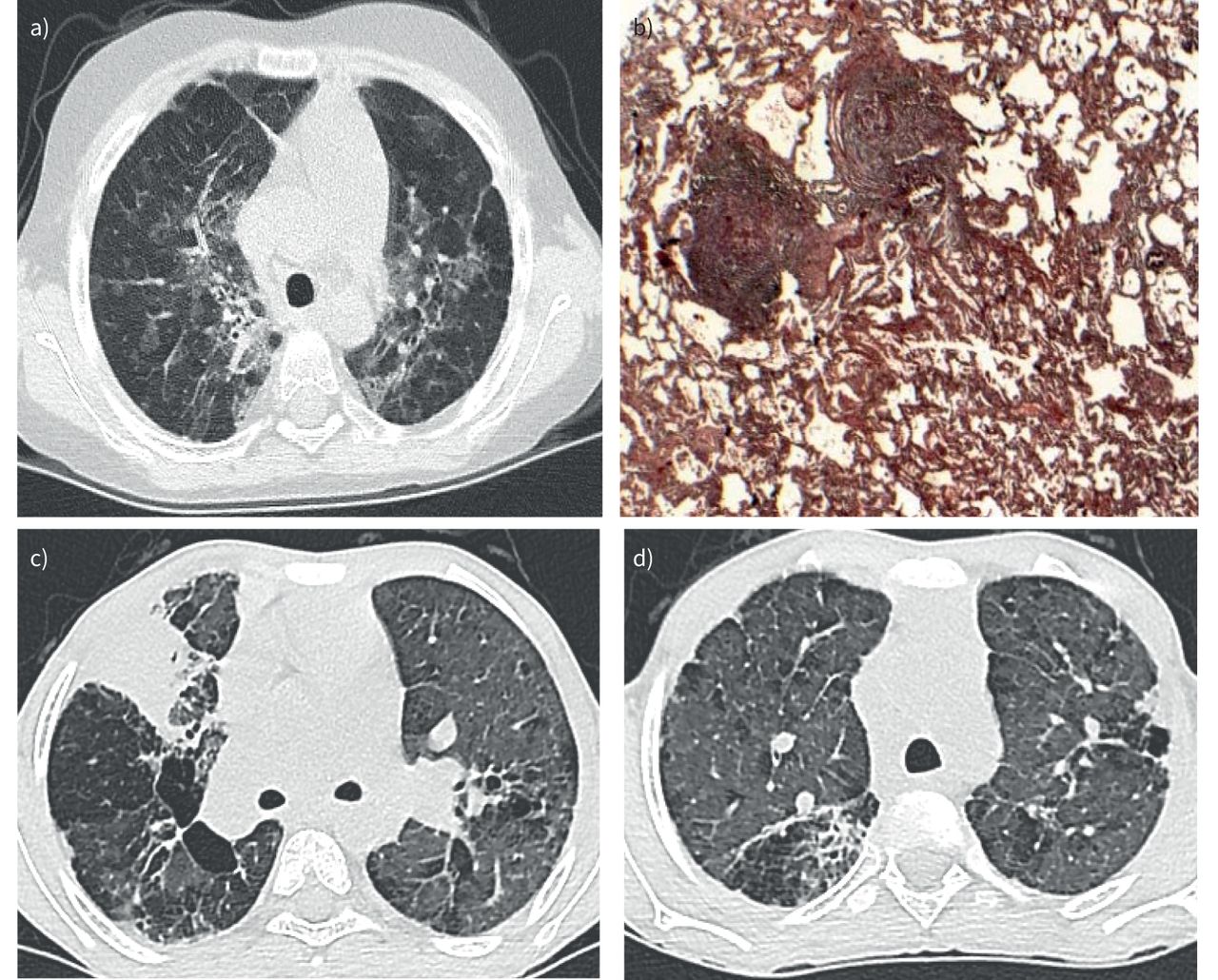
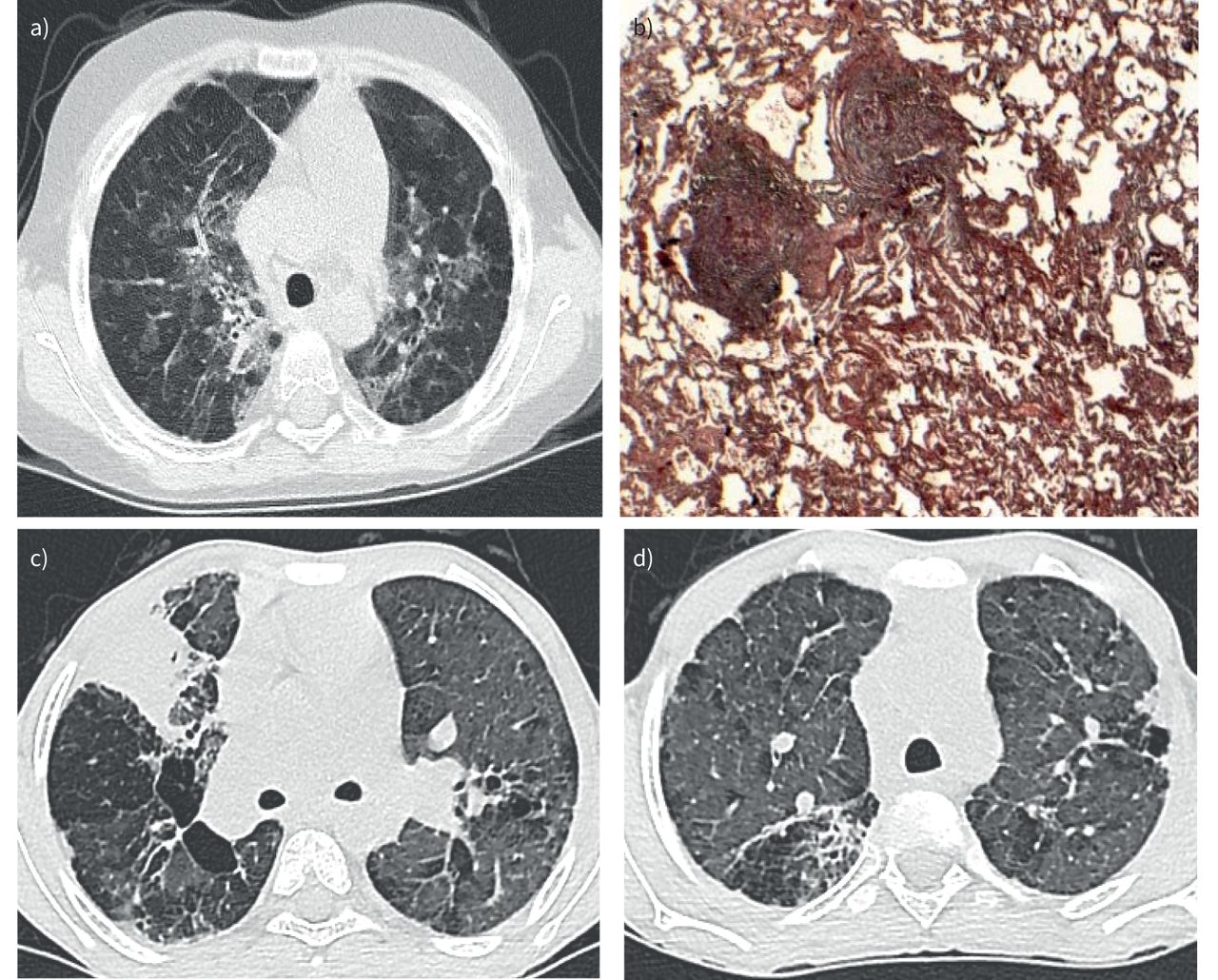
a, b) Subject 4: 5-year-old female patient, presented with severe failure to thrive and third-degree clubbing. She had profound hypoxaemia (oxygen saturation 80% at rest in room air), with widespread fine crepitations and severe pulmonary hypertension. a) Axial computed tomography (CT) shows bilateral scattered central and peripheral patchy areas of ground-glass opacities (GGO) and septal thickening. This is associated with a few areas of air trapping, giving a mosaic pattern; b) lung histopathology shows granulomas surrounded by a rim of chronic inflammatory cells (haematoxylin and eosin ×20). Thorough immunological testing was performed after the biopsy, and dihydrorhodamine (DHR) testing showed an abnormal response, confirming the diagnosis of chronic granulomatous disease. c, d) Subject 5: a 10-year-old male patient who presented with childhood interstitial and diffuse lung disease and was later diagnosed with chronic granulomatous disease (CGD). He had severe initial clinical presentation with hypoxia at rest (in room air) and marked failure to thrive. c) Axial CT shows bilateral peripheral and central large patchy areas of GGO with areas of air trapping giving a mosiac pattern, associated with septal thickening and a few mainly lower lobar emphysematous changes and central cystic changes. A large consolidative patch is noted affecting the anterior segment of the right upper lobe; d) abnormal bronchial thickening and minimal tractional bronchiectasis. Biopsy was planned, but it was deferred as he started to suffer from recurrent skin and deep-organ abscesses requiring surgical drainage. Further immune tests were done and DHR testing showed an abnormal response, confirming the diagnosis of CGD.
- FIGURE 3
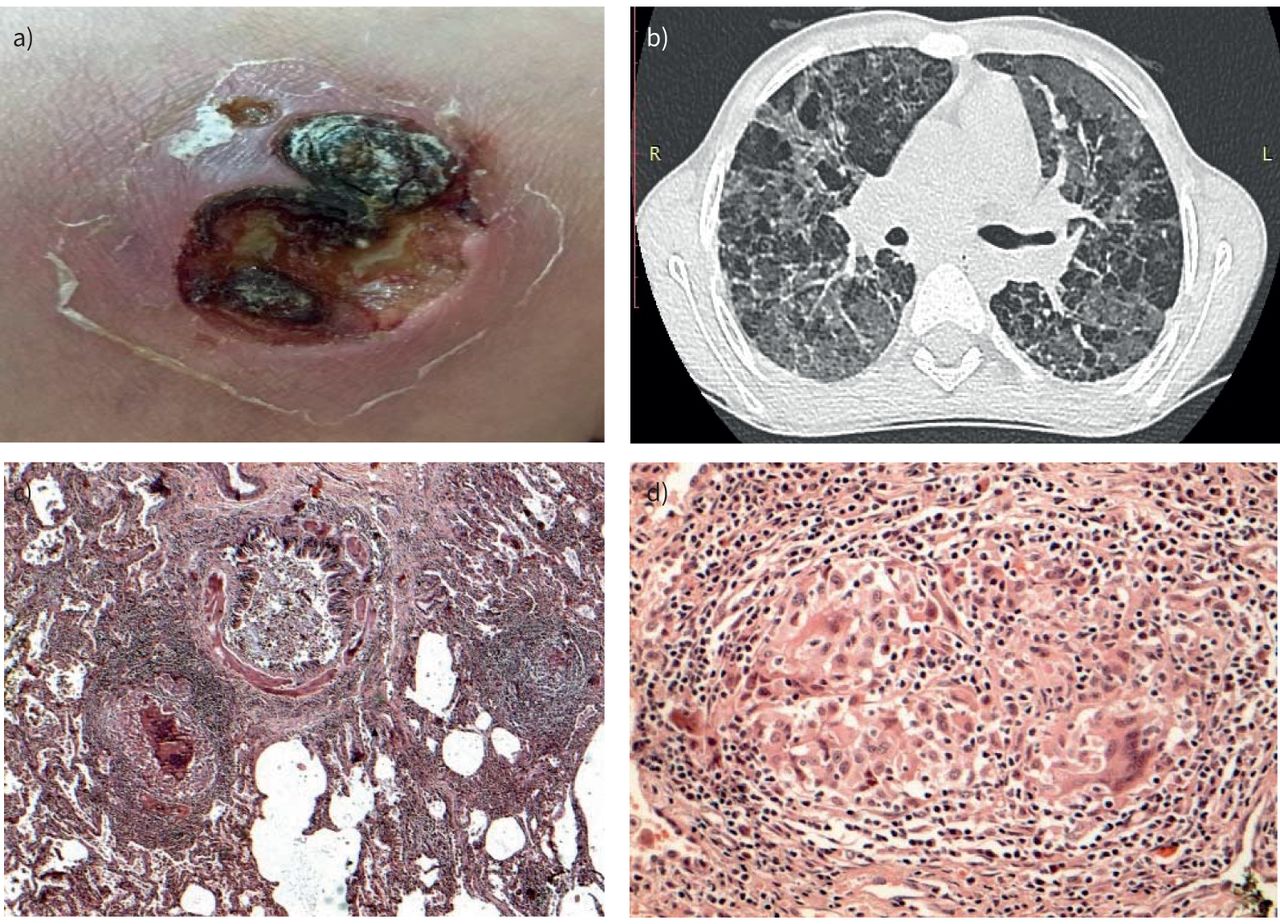
Subject 7: 8-year-old female had history of persistent dry cough and dyspnoea. She is the second child of first-degree consanguineous parents. In addition to the pulmonary symptoms, she had bouts of self-limiting noninfective diarrhoea and a) pustular skin lesions. In addition, she had a history of paediatric intensive care unit admission with severe sepsis which marked the disease onset. On presentation to us, she was tachypnoeic and hypoxic with widespread fine crepitations and wheeze by auscultation. An immunological profile showed elevated immunoglobulins and transient positivity of perinuclear anti-neutrophil cytoplasmic antibodies, which disappeared later on. Cluster of differentiation markers show borderline low natural killer cells and CD4 levels. Flow spirometry showed a restrictive pattern. b) Axial computed tomography shows bilateral mosaic appearance of both lung lobes (ground-glass appearance alternating with areas of air trapping), with peri-bronchial wall thickening and pre-septal thickening. c) Histopathology shows bronchocentric inflammation and granulomatous inflammation. d) Granuloma (high power). Haematoxylin and eosin c) ×40 and d) ×200. Histopathology findings were consistent with a granulomatous lymphocytic interstitial lung disease spectrum. Dihydrorhodamine test was normal and repeat immune studies showed persistent elevation of immunoglobulin levels, excluding underlying common variable immune deficiency.
- FIGURE 4
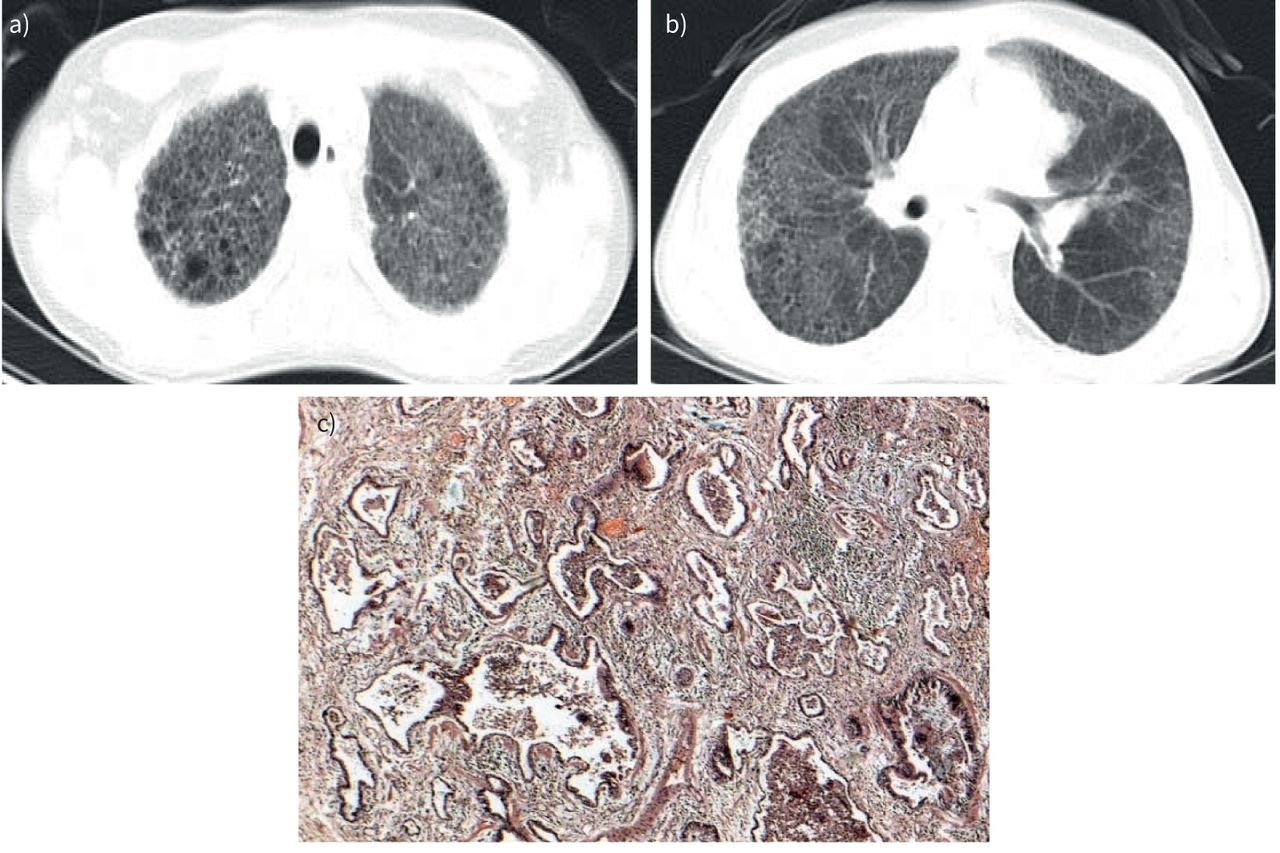
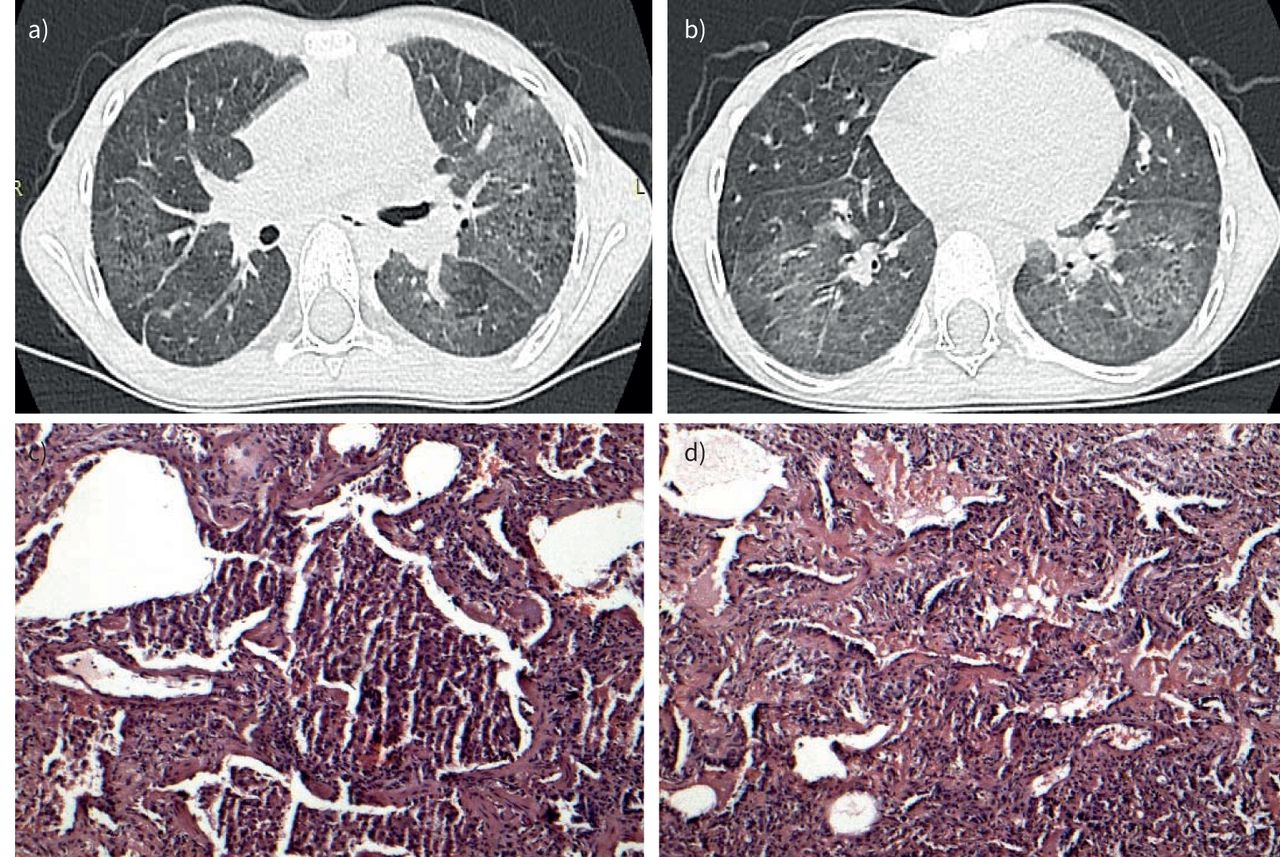
Subject 8: 8-year-old female patient referred for further assessment. She complained of chronic dry cough and progressive dyspnoea. She has a history of familial death with undiagnosed interstitial lung disease in the fifth decade (uncle). On presentation to us she was tachycardic, tachypnoeic and hypoxic (oxygen saturation 88% in room air). In addition, she had severe cachexia with third-degree clubbing. Echocardiography showed severe pulmonary hypertension with dilated right atrium and ventricle. a, b) Axial computed tomography shows bilateral predominantly upper lobar and peripheral ground-glass opacities associated with peripheral reticular infiltration and honeycombing. c) Histopathology shows that the lung architecture is completely lost, with replacement by end-stage (honeycomb) fibrosis (haematoxylin and eosin ×40).
- FIGURE 5
Subject 9: 7-year-old female, referred for further assessment. She had a history of dyspnoea shortly after birth, associated with failure to thrive. Her condition deteriorated to dyspnoea at rest and attacks of cyanosis. On presentation, she was markedly distressed, with respiratory rate 70 breaths·min−1, heart rate 150 beats·min−1 (tachycardia with gallop) and hypoxia (oxygen saturation 85% in room air, at rest). In addition, she had third-degree clubbing and marked failure to thrive. She had bilateral fine crepitations on auscultation with accentuated second heart sound and tender hepatomegaly. Echocardiography showed dilated right ventricle and severe pulmonary hypertension. Axial computed tomography shows a) bilateral (predominantly upper lobar) subpleural and intraparenchymal microcysts and b) bilateral diffuse pulmonary ground-glass opacities, with predominant affection of both lower lobes. Histopathology shows c) predominance of alveolar macrophage accumulation and d) diffuse and uniform interstitial chronic inflammation and mild fibrosis, characteristic of nonspecific interstitial pneumonia. This mixed histological pattern (fibrotic nonspecific interstitial pneumonia and desquamative interstitial pneumonia) in the paediatric age group is suggestive of an underlying surfactant protein disorder (haematoxylin and eosin c, d) ×100).
- FIGURE 6
Subjects 11 and 12: two affected siblings with a history of grandparent death of undiagnosed interstitial lung disease (ILD) in the fourth decade. a, b) Computed tomography (CT) images from the older sibling: a) diffuse pan-lobar pulmonary emphysema with areas of air trapping, abnormal bronchial wall thickening; b) bilateral lower lobar scattered tiny ground-glass nodules showing tree-in-bud appearance. c, d) CT images from the younger sibling: c) air trapping and hyperinflation; d) bilateral few peripheral lower lobar tiny ground-glass nodules with a few of them giving tree-in-bud appearance. The younger sibling presented with a worse clinical picture (severity score 5) and her spirometry showed a restrictive defect. The older sibling presented with significant symptoms and signs and hypoxia at rest and her spirometry showed mixed obstructive and restrictive defect, with negative reversibility test. e, f) Histopathology of the older sibling, with findings consistent with idiopathic bronchiolocentric pattern of interstitial pneumonias: e) peribronchiolar inflammation (low power); f) peribronchiolar metaplasia (higher power) (haematoxylin and eosin e) ×40 f) ×100). Grocott stain for fungi was negative. General causes of diffuse parenchymal lung disease were thoroughly excluded as well as immune deficiency and α1-antitrypsin deficiency. A specific cause for this histological pattern couldn't be precisely identified, but a strong family history with two siblings having respiratory symptoms since birth and grandparent death due to ILD raises serious concerns for an underlying genetic disorder.
- FIGURE 7
a, b) Subject 13: Male patient referred to our hospital by the age of 8 years with history of worsening dyspnoea and bouts of cyanosis. He had a history of recurrent attacks of dyspnoea and dry cough since birth, in addition to global developmental delay of unidentified aetiology. An initial diagnosis of bronchial asthma was made in primary care, yet there was no significant improvement on conventional asthma management. On presentation to us, he was tachypnoeic and hypoxic (oxygen saturation 89% in room air, at rest). Examination revealed marked failure to thrive, in addition to fine crepitaions and wheeze by auscultation. a) Axial computed tomography (CT) shows multiple scattered patchy areas of ground-glass opacities alternating with few areas of air trapping, giving a mosaic pattern; b) histopathology shows chronic bronchiolitis (haematoxylin and eosin ×40). c, d) Subject 14. c) Axial CT shows bilateral scattered tiny pulmonary ground-glass nodules 2–3 mm on average showing centrilobular and peribronchial distribution; d) histopathology shows chronic bronchiolitis with airway lumens focally containing mucin (haematoxylin and eosin ×20).
- FIGURE 8
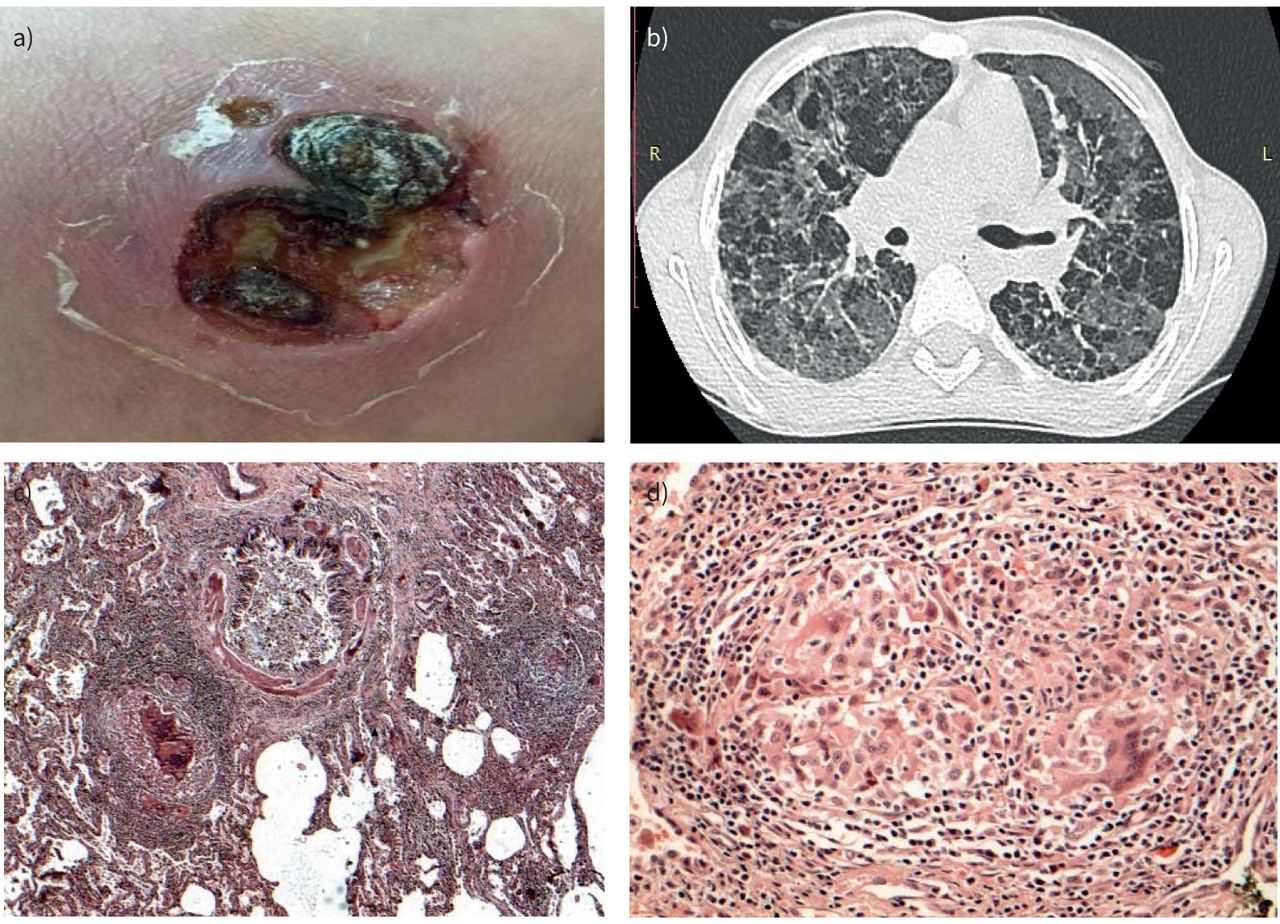
Subject 16: 9-year-old female, referred for further assessment of her poorly controlled asthma. On presentation she had dyspnoea and hypoxaemia at rest with widespread fine crepitations and wheeze by auscultation and a) notably puffy fingers. Initial lab investigations were nonconclusive. b) Axial computed tomography shows bilateral mainly lower lobar extensive ground-glassing associated with few areas of air trapping, more evidently affecting the right lower lobe, giving a mosiac pattern. c) Histopathology shows bronchocentric interstitial pneumonia: interstitial chronic inflammation, more marked around bronchovascular bundles (low power); d) an occasional focus of organising pneumonia is noted (haematoxylin and eosin c) ×40 d) ×100). In addition, she developed progressive digital tip ulcers, sclerodactyly, in addition to induration proximal to the metacarpophalangeal joint (this appeared later). Overall features confirm the diagnosis of systemic sclerosis.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Tables
- TABLE 1
Classification of enrolled subjects according to their clinical, radiological, laboratory and histopathology features
History Age at start of symptoms years Age at referral years Fan score Spirometry Chest CT Histopathology Significant laboratory/BAL findings Final opinion 1 Exposure to doves and chicken 4 9 5 RVD Consolidation, septal thickening GLD Specific Dx: chronic HP 2 Exposure to doves and chicken 2.5 3.5 2 Not done# Reticulations/diffuse micronodules GLD Eosinophilia Specific Dx: chronic HP 3 Exposure to doves/benzene/hookah 3.5 4 3 Not done# GGO/consolidation/reticulations Interstitial inflammation more marked around BVB Eosinophilia Specific Dx: subacute HP 4 Recurrent pneumonias 1 5 5 RVD GGO/air trapping/septal thickening GLD Elevated ESR/DHR: defective response Specific Dx: CGD (PID) 5 Recurrent skin abscesses /previous pulmonary TB infection 6.5 10 4 MVD Multiple findings (figure 2) Not done Elevated ESR/DHR: defective response Specific Dx: CGD (PID) 6 Recurrent pneumonias 8 13 5 RVD GGO/air trapping/septal thickening/reticulations/consolidation GLD Elevated ESR/DHR: defective response Specific Dx: CGD (PID) 7 Recurrent pustular skin lesions 5 8 4 RVD GGO/air trapping/septal thickening GLILD Elevated ESR/low NK cells and CD4/elevated immunoglobulins/negative viral serology Specific Dx: GLILD (non-CVID related) 8 Familial death of ILD (uncle)/chILD onset after severe pneumonia 6 8 5 RVD GGO/honey combing/reticulations Severe fibrotic NSIP (honeycomb lung) Negative viral serology and immune studies
No evidence of microbial infection (by BAL)Specific Dx: IP (fibrotic NSIP-honeycomb lung)¶ 9 Dyspnoea since birth Since birth 7 5 RVD GGO (with predominant affection of lower lobes), microcysts Mixed fibrotic NSIP and DIP Specific Dx: IP (NSIP/DIP)¶ 10 GDD/familial death of undiagnosed ILD (sibling) 5.5 6 2 Not done# GGO/air trapping NSIP (cellular) Specific Dx: IP (NSIP)¶ 11 Familial death of undiagnosed ILD in the 4th decade (grandparent) Since birth 11 4 MVD Emphysema/lower lobes tiny ground-glass nodules (tree-in-bud pattern) BPIP Negative immune studies Specific Dx: IP (BPIP)¶ 12 Familial death of undiagnosed ILD in the 4th decade (grandparent) Since birth 5 5 RVD Air trapping/hyperinflation/lower lobes tiny ground-glass nodules (tree-in-bud pattern) Parents refused (cases 11 and 12 are siblings) Negative immune studies Suggestive Dx: familial ILD of unidentified aetiology 13 GDD Since birth 8 4 Not done# GGO/air trapping Chronic bronchiolitis/interstitial chronic inflammation Specific Dx: chILD related to SAD with background IP+ 14 GDD 0.25 5 4 Normal Ground-glass nodules 2–3 mm (centrilobular and peri-bronchial distribution) Chronic bronchiolitis/interstitial chronic inflammation Specific Dx: chILD related to SAD with background IP+ 15 NICU admission at birth for 2 months/full term Since birth 14 2 MVD GGO (a few show crazy paving) Chronic bronchiolitis/interstitial chronic inflammation Specific Dx: chILD related to SAD with background IP+ 16 Puffy fingers/digital tip ulcers/sclerodactyly/induration proximal to MCP (late) 4 8 4 Not done# Bibasilar GGO BPIP + focal OP Abnormal nail-fold capillaries Specific Dx: Systemic sclerosis 17 Haemoptysis/admitted twice for blood transfusion for severe microcytic anaemia 4 5 2 Normal GGO Not done BAL: HLM >60% of cells/other causes of DAH were excluded Specific Dx: IPH 18 Haemoptysis/admitted six times for blood transfusion for severe microcytic anaemia 5.5 7 2 RVD GGO Not done BAL: HLM >45% of cells/other causes of DAH were excluded Specific Dx: IPH 19 Progressive dyspnoea over 2 months 11 11 5 Not done# Cysts (sparing CPA)/GGO/tiny nodules Death before any invasive tests Suggestive Dx: LCH 20 1 3.5 4 Not done# Cysts (sparing CPA)/GGO Dropped out Suggestive Dx: LCH 21 History of pulmonary TB 3.5 4.5 5 Not done# GGO/reticulations/atelectatic bands Clinically improving (not done) Negative immune studies Specific Dx: post-infectious chILD (post-TB) 22 Start of disease following attack of severe pneumonia 6 6 4 RVD GGO OP and reactive fibrous pleuritis Negative immune studies Specific Dx: post-infectious chILD (OP) CT: computed tomography; BAL: bronchoalveolar lavage; RVD: restrictive ventilatory dysfunction; GLD: granulomatous lung disease; Dx: diagnosis; HP: hypersensitivity pneumonitis; GGO: ground-glass opacities; BVB: bronchovascular bundles; ESR: erythrocyte sedimentation rate; DHR: dihydrorhodamine test; CGD: chronic granulomatous disease; PID: primary immune deficiency; TB: tuberculosis; MVD: mixed ventilatory dysfunction; GLILD: granulomatous lymphocytic interstitial lung disease; NK: natural killer; CVID: common variable immune deficiency; ILD: interstitial lung disease; chILD: childhood interstitial and diffuse lung diseases; NSIP: nonspecific interstitial pneumonia; IP: interstitial pneumonia; DIP: desquamative interstitial pneumonia; GDD: global developmental delay; BPIP: bronchiolocentric pattern of interstitial pneumonias; SAD: small airways disease; NICU: neonatal intensive care unit; MCP: metacarpophalangeal joint; OP: organising pneumonia; HLM: haemosiderin-laden macrophages; DAH: diffuse alveolar haemorrhage; IPH: idiopathic pulmonary haemosiderosis; CPA: costophrenic angle; LCH: Langerhans cell histiocytosis. #: too young or too dyspnoeic to do the test or suffering from global delay (noncooperative); ¶: further genetic testing required to exclude surfactant dysfunction mutation; +: future genetic studies are also warranted for this group, as symptom onset was at birth or shortly after birth.
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
TABLE S1 Comparison between chest X-ray and corresponding chest CT findings among enrolled subjects 00880-2020.tableS1
TABLE S2 Bronchoscopy and bronchoalveolar lavage (BAL) indications, characteristics and other relevant investigations for selected cases 00880-2020.tableS2
TABLE S3 Highlights on treatment changes after the diagnostic evaluation 00880-2020.tableS3










