





Abstract
Nasal epithelial cells from very preterm infants have a functional defect in their ability to repair beyond the first year of life, and failed repair may be associated with antenatal steroid exposure https://bit.ly/39OFJs7
To the Editor:
Preterm birth rates are increasing and now account for >11% of global births. Simultaneously, advances in neonatal care have led to increased survival of lower gestation neonates. A complication of preterm birth, and the biggest determinant of survival, is lung and airway immaturity. After preterm birth, the immature respiratory system is exposed to pro-inflammatory stimuli like injury from resuscitation and oxygen toxicity. The airway epithelium, the physical barrier between insults and the airways, is particularly vulnerable to injury. If epithelial barrier integrity cannot be restored rapidly following damage (i.e. via aberrant repair), the respiratory system is left unprotected, increasing the risk of infection, inflammation and tissue damage. Altered epithelial repair may play an important role in the ongoing respiratory health problems experienced by preterm survivors, including severe respiratory infections throughout early life, or low and declining lung function [1–3]. Deficits are further exacerbated in those with bronchopulmonary dysplasia (BPD). The mechanisms contributing to ongoing respiratory problems are currently unknown, although probably begin in early life. Until now, understanding the role of the preterm epithelial barrier has been limited by a lack of appropriate cellular models. Our study aimed to assess the reparative capacity of the airway epithelium in survivors of preterm birth and its association with early life outcomes, with the hypothesis that preterm airway epithelial cells have an abnormal repair mechanism.
Primary nasal epithelial cells (NECs) were collected from infant survivors of very preterm birth (n=32; <32 weeks gestation; median (range) age 1.4 (1.2–1.5) years; corrected postnatal age 1.2 (1.0–1.3) years). BPD was defined as the requirement for ≥28 days supplemental oxygen. Perinatal data and lung function outcomes were collected as part of the Preterm Infant Function and Clinical Outcomes (PIFCO) cohort study (Child and Adolescence Health Service, Perth, Australia; ethics approval #2014083EP). Term-born infant samples (n=8; median (range) age 2.5 (2.0–2.7) years) were provided through the Western Australian Epithelial Research Program (WAERP) (St John of God Subiaco Hospital, Subiaco, Australia; ethics approval #901.1421). This study was approved by the relevant human ethics committees and written informed consent was provided by all parents.
NECs were collected from the nasal turbinate(s) as previously described [4, 5]. Cellular morphology was assessed via light microscopy, and epithelial cell lineage confirmed by PCR and immunofluorescence [4]. Confluent cultures were wounded using an Essen WoundMaker, and repair assessed over 72 h using image-tracking software (IncuCyte ZOOM, Essen BioScience) [4]. All experiments were completed between passage 2 and 3, to ensure consistency.
Perinatal factors including gestation, birthweight z-score, duration of respiratory support, BPD and antenatal/postnatal steroids were correlated with extent of wound closure (Spearman's Rho or point-biserial as appropriate). Mann–Whitney U-tests were used to assess statistical differences in wound closure rates (SPSS Statistics V26; IBM). p-values of <0.05 were considered statistically significant.
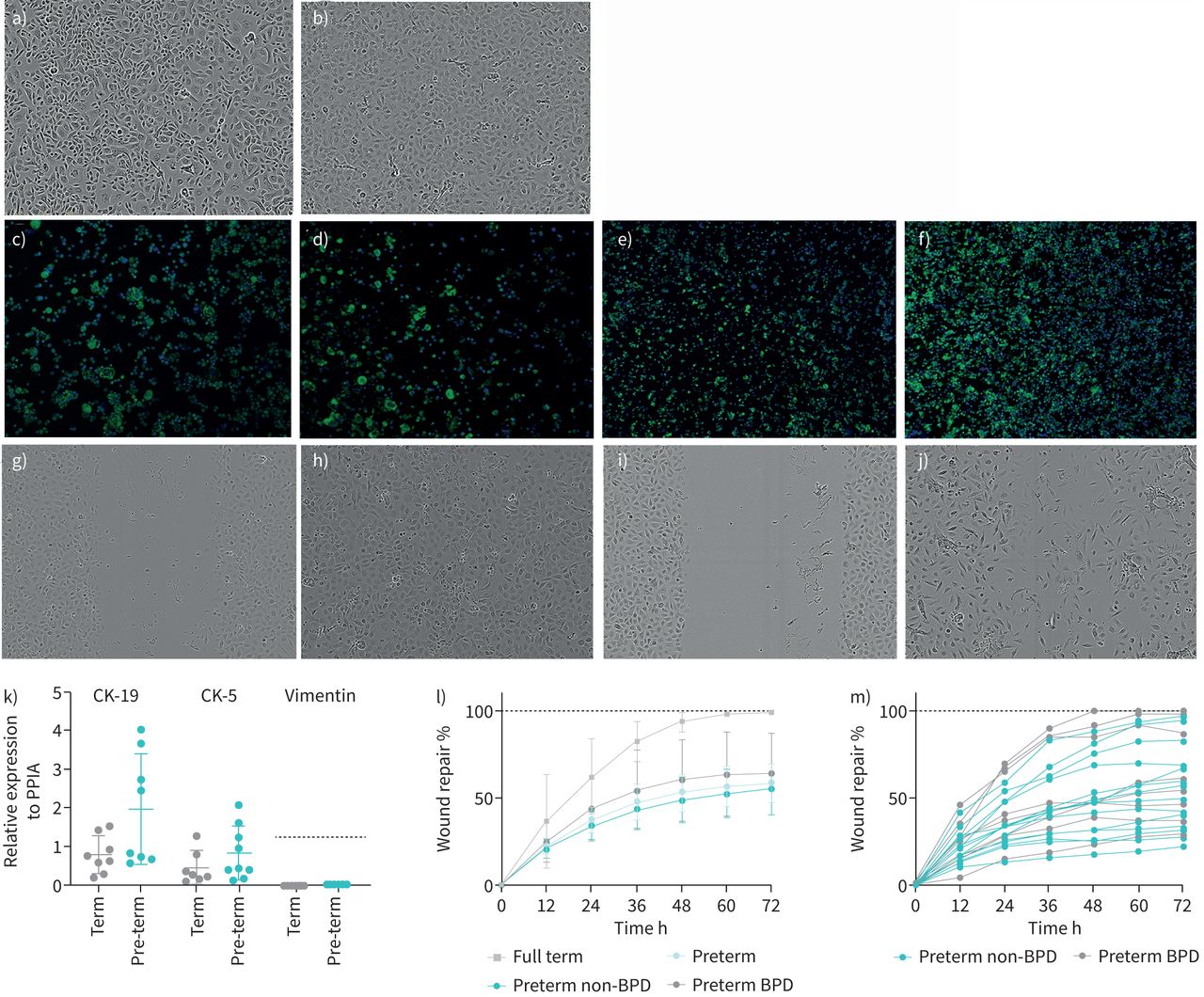
Successful cultures were established from eight term infants (eight brushed, 100% culture success) and 22 preterm infants (32 brushed, 69% culture success). All cultures exhibited a typical cobblestone epithelial morphology (figure 1a and b). Epithelial lineage was confirmed at both gene and protein levels (term n=7–8, preterm n=8–9) (figure 1c–f and k); established cells solely expressed epithelial-specific markers cytokeratin 5 and 19, with no significant differences, but not the mesenchymal-specific marker vimentin. Perinatal or anthropometric factors including gestational age, chorioamnionitis and respiratory support were not associated with culture success (data not shown).

{kind=link}
Establishment, characterisation and functional assessment of primary airway epithelial cells from preterm infants with and without bronchopulmonary dysplasia (BPD) and term controls. Established primary upper (nasal) epithelial cell cultures of a) term-born and b) preterm-born infants (10× magnification) exhibit a typical epithelial cobblestone morphology. c–f) Epithelial lineage expression was corroborated at the protein level using immunocytochemistry. Immunofluorescent staining of cells using the nuclear stain DAPI (blue) showed that all cells were positively stained (green) for c, d) cytokeratin (CK)-19 and e, f) CK-5 at c, e) term and d, f) preterm. g–j) Images of nasal epithelial cell repair for g, h) term and i, j) preterm at g, i) 0 h and h, j) 72 h. k) Gene expression of epithelial lineage markers CK-19 and CK-5 and mesenchymal cell lineage marker vimentin in term (n=7–8) and preterm (n=8–9) primary epithelial cells, relative to the peptidylprolyl isomerase A gene (PPIA). All established cultures strictly expressed epithelial lineage markers, with expression of CK-19 and CK-5 and no expression of vimentin. The median and interquartile range (IQR) are shown, and the dashed line represents the positive control for vimentin. l) Repair rates of airway epithelial cells from term (n=8), preterm (n=22), preterm non-BPD (n=14) and preterm with BPD (n=8) infants over a 72-h period, showing the median and IQR. Cultures from term infants completed full repair by 60 h, whereas those from preterm infants were significantly delayed and/or failed to repair over the same period. m) Repair rates of cultures from individual preterm non-BPD infants (n=14) and preterm infants with BPD (n=8). Diagnosis of BPD was not correlated with worse reparative capacity. Repair rates varied among cultures from preterm infants and no differences were observed between preterm BPD and non-BPD infants.
NEC cultures from infants born preterm had significantly impaired reparative capacity (p<0.05; figure 1l and m), while those from term infants completely repaired, typically by 60 h (figure 1l). Further assessment identified a spectrum of repair responses in the preterm group (figure 1m). Interestingly, NECs from only four preterm participants fully healed by 72 h, with cells from all remaining participants failing to completely repair (n=18). Of these, over half (10 out of 18) had wound closure below 50% (figure 1l and m). Wound repair capacity did not differ between preterm infants with or without BPD, nor correlate with gestation, birthweight z-score, duration of oxygen or respiratory support. However, decreased repair was associated with the administration of antenatal steroids >24 h prior to delivery (table 1).
Demographic data for preterm infants and correlation to airway epithelial cell wound repair at 72 h
This study is the first to identify functional defects in the reparative capacity of NECs of preterm infants. Almost all preterm infants in this cohort exhibited defective NEC repair in their second year of life, suggesting that not only is a defect present, but it is also retained beyond the neonatal period. Defective repair has previously been suggested by Been et al. [6], who showed that bronchoalveolar lavage fluid (BALF) collected from preterm infants after birth elicited defective wound repair when added to immortalised commercially available alveolar type II cells. Our findings advance the field further, showing that the effect is intrinsic to the airway epithelium and improving the clinical relevance by using primary NECs obtained from preterm infants.
A correlation between defective repair and antenatal steroid administration was identified in the present study. Similarly, Been et al. [6] observed worse repair with the addition of BALF of preterm infants receiving antenatal steroids. The association of antenatal exposure (in the absence of current steroid use) with dysregulated repair is intriguing and warrants further investigation into the impact of antenatal steroids on the epithelium. No additional correlations were observed between repair capacity and perinatal factors including gestation, birthweight, respiratory support or BPD diagnosis. The lack of correlation with perinatal factors suggests an underlying intrinsic mechanism may be driving the poor repair. Previous studies have shown defective repair in other chronic lung diseases such as COPD, asthma and cystic fibrosis [7–9]. Our previous work has investigated underlying mechanisms of defective epithelial repair in childhood wheeze and asthma, and we have found associations with impaired fibronectin-binding integrin expression [10, 11]. It is possible that a similar defect is driving dysregulated repair in the preterm epithelium, although alterations in cell migration and proliferation may also be contributing factors. Further research is required to identify and explore the underlying mechanisms driving poor repair in the preterm epithelium.
The clinical implications of aberrant NEC repair in preterm infants remain unknown. In other chronic respiratory diseases like asthma, the inability to maintain barrier integrity via defective repair has been associated with acute wheeze, symptom severity and increased hospital presentations [10]. The dysregulated repair in preterm infants may in part explain the high rates of hospitalisation, susceptibility to respiratory infection and longitudinal lung function decline observed throughout childhood. However, further investigation is needed to understand the mechanistic drivers of dysregulated repair in these children. It should be noted that this study utilised NECs, which may not represent the lower airway. However, the unified airways hypothesis suggests that upper airway cells can be used as a surrogate for the lower airway, although this remains unproven in a preterm cohort [12]. We acknowledge the age difference between our cohorts; however, it is unlikely that this limits interpretation, given that our prior work has found no age-related effects on repair capacity [9]. In conclusion, this study is the first to report a functional defect in NECs of infants born preterm. Only by understanding the cellular and molecular mechanisms underpinning poor respiratory outcomes after preterm birth will it be possible to optimise the treatment and clinical management of this population.
Acknowledgements
The authors would like to thank participants and their families from the PIFCO and WAERP studies.
Footnotes
Author contributions: J. Hillas, D.J. Evans and T. Iosifidis carried out acquisition and analysis of data. N. Hemy and E. Kicic-Starcevich recruited all participants. S. Ang and L.W. Garratt provided technical support. J. Hillas and D.J. Evans drafted the manuscript. S.J. Simpson and A. Kicic conceptualised the study, obtained funding and validated data for accuracy. All authors approved the final version.
Conflict of interest: J. Hillas has nothing to disclose.
Conflict of interest: D.J. Evans has nothing to disclose.
Conflict of interest: S. Ang has nothing to disclose.
Conflict of interest: T. Iosifidis has nothing to disclose.
Conflict of interest: L.W. Garratt has nothing to disclose.
Conflict of interest: N. Hemy has nothing to disclose.
Conflict of interest: E. Kicic-Starcevich has nothing to disclose.
Conflict of interest: S.J. Simpson has nothing to disclose.
Conflict of interest: A. Kicic has nothing to disclose.
Support statement: This work was funded by a Perpetual IMPACT Philanthropy Grant (IPAP2017/1355). S.J. Simpson is a NHMRC early career fellow. A. Kicic is a Rothwell Family Fellow. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received December 5, 2020.
- Accepted March 27, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org










