





Abstract
The European Cooperation in Science and Technology (COST) is a funding organisation for the creation of research networks, called COST Actions. COST Action 16125 was dedicated to European network for translational research in children's and adult interstitial lung disease. Working Group 5 of the COST Action CA16125 focussed on the problems of transition of children with interstitial lung diseases from paediatric to adult care. Results of this survey performed among members of the Working Group and some affiliated specialists showed highly variable and inadequate current system of transitions of these patients to adult care in most centres. In most centres there is no established and consistent procedure to guarantee appropriate transfer of information and prepare the patient for transition to a new specialist and a new team. Immediate action is therefore required. The Working Group has prepared a model procedure for the transition, based on protocols from several centres with established pathways, either for childhood interstitial lung disease or other chronic respiratory diseases.
Abstract
Transition of children with interstitial lung disease to adult care is a critical part of long-term follow-up and care. There is a lack of standardised procedures across European centres. This article suggests a structured procedure for this transition. https://bit.ly/2M2Y7EV
Introduction
Interstitial lung diseases (ILD) are a very heterogeneous spectrum of mostly chronic conditions that predominantly affect the alveolar wall, distal airways and interstitium. These pathological processes may lead to gradual loss of lung function characterised by restrictive pulmonary disease and reduced lung compliance. With advanced disease and impaired gas exchange the patients develop chronic respiratory failure and may need oxygen supplementation, ventilatory support and, eventually, lung transplantation. The prognosis of paediatric ILD (chILD) is generally better than that of adults. However, some children may be left with chronic disease continuing into adulthood. Even in those who obtain remission during childhood, there may be some serious sequelae of the disease and its treatment, for example systemic corticosteroids [1], and there may be a risk of later relapse.
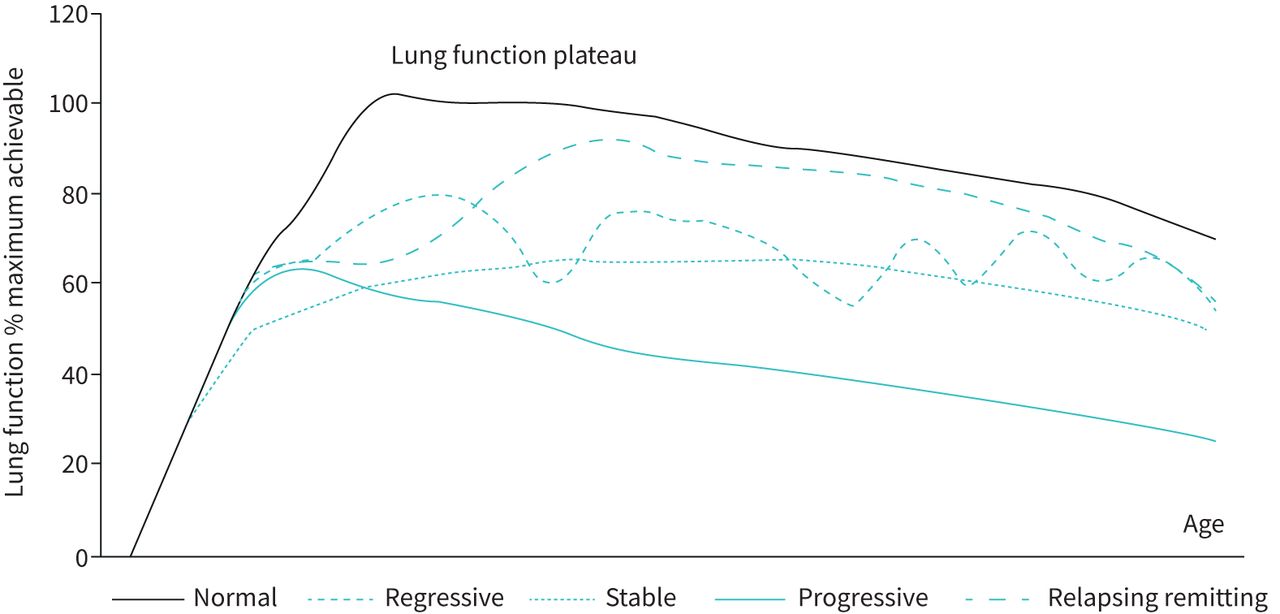
Following patterns of the disease development have been described (figure 1).

Different time courses of the disease according to the development of lung function.
Regression of lung disease
A spontaneous alleviation or disappearance of symptoms (e.g. neuroendocrine cell hyperplasia of infancy (NEHI) pulmonary interstitial glycogenosis (PIG)), which in some cases may be “accelerated” by treatment (e.g. corticosteroids in PIG) [2]. Residual deficits in lung function can be demonstrated in some individuals [3]. The long-term consequences of these diseases are not yet known (see OLS for NEHI sequelae in particular); however, a decrease in the growth potential of the lungs can be expected and their connection with some, so far idiopathic, pulmonary pathologies of adulthood cannot be completely ruled out.
Stable lung disease
Damage is caused by a single hit (e.g. severe viral infection causing obliterative bronchiolitis, radiation or toxic lung disease, and acute forms of exogenous allergic alveolitis with complete elimination of external antigen). Depending on the timing of the insult, some catch-up lung growth can be expected. In general, the earlier the hit, the greater the regenerative capacity of the lungs and the higher the compensatory potential. However, the full lung growth potential may not be reached and the normal adult age-related decline in lung function leads to a risk of early onset respiratory insufficiency. This group of patients requires special attention, as lung involvement may not apparently be significant at the time of transition.
Progressive pulmonary involvement
Over time, lung involvement worsens either due to persistent external noxious agents (e.g. permanent antigen exposure in a chronic form of exogenous allergic alveolitis) or a pathogenetic mechanism that continues after being initiated. This progression may occur even if the initial stimulus has been removed (e.g. chronic inflammatory activity in systemic “autoimmune” diseases, fibrotic processes, etc.). Ongoing disease progression may be accelerated by episodes of acute exacerbation.
Relapsing and remitting pattern
The disease has a variable course that may remain stable for some period of time but may frequently exacerbate due to various triggers (e.g. surfactant protein C deficiency).
Current ideas about the expected time course of selected chILDs are summarised in Online supplement table 1.
Hence, it is very important for those diagnosed with chILD to have guaranteed uninterrupted follow-up from childhood to the adult life.
Transition protocols have already been developed for a few chronic diseases (e.g. cystic fibrosis, cardiac and metabolic diseases, sickle cell anaemia) and are still being improved [4–10]. Much less work has been done about transition in rare respiratory diseases including chILD, where data on transition are virtually non-existent. However, from other chronic diseases we know that insufficient support during transition to adult care is often associated with deterioration of health status [11]. The highest risk is seen in children with less severe disease or with some degree of remission, who are often lost to follow up.
During the COST Action CA16125, European Network for Translational Research in Children's and Adult Interstitial Lung Disease (EnTER), a systematic analysis of the current situation in the care for paediatric and adult ILDs was performed with the goal of improving the long-term follow-up of chILD patients. Working group 5 (WG5) has been dedicated to the issue of transition of chILD patients to adult care. In this paper, we present the results of a survey identifying the disparities in provision for adults and children with ILD across Europe and the differences of the approaches to the transition of chILD patient. We aimed to identify limitations and current gaps and propose an ILD-specific model for transition.
Methods
The questionnaire covering various aspects of chILD transition was developed by P. Pohunek, M. Vašáková and A. Bush for the purpose of this survey. It comprised of general questions characterising: the respondent's background; the health-care system in the respective country to obtain data about the availability of services and medications; and the availability and structure of medical team of chILD/ILD centre (including dedicated specialists). Transition-specific questions followed.
The link to the survey questionnaire was sent to 111 individuals who either registered with the WG5 or expressed their interest and agreed to participate in the study. The full questionnaire is available at https://docs.google.com/forms/d/e/1FAIpQLSeR00CJgXlWWpCLItBqtumrbr3WBaJQxa6GhzdufLLDDamrBg/viewform?fbzx=-8896405808421949487 and in the online supplement. For questions related to the national situation, if we received more than one answer from that country, the results were analysed and manually adjusted and compacted to obtain results that were representative for the situation and practice in that country.
Based on the results of the survey, the critical aspects of the chILD transition to adult care were identified and the available transition protocols were analysed. Results were presented and discussed at the meetings of the members of the WG5 at the COST Action CA 16125 conferences in Belgrade (Serbia; November 1–3, 2018) and in Timisoara (Romania; September 11–13, 2019). Outcomes from the discussion were summarised into a suggested standard operation procedure for chILD transition into adult care. The final proposed document is presented below.
Results
The survey
After one round of reminders we eventually received 39 answers from centres in 21 countries: 19 European (Austria, Belgium, Croatia, the Czech Republic, France, Germany, Greece, Hungary, Ireland, Italy, the Netherlands, Poland, Portugal, Romania, Serbia, Spain, Sweden, Turkey and the UK) and two non-European (Australia, Israel). Most answers came from paediatric pulmonologists (27), and fewer from adult specialists (10). One paediatric radiologist and one “other” adult specialist participated as well.
The information on epidemiology of chILD in the individual countries was rather disappointing (n=14, no data available; n=7, only rough estimates with a wide span of ranges with no reliable data).
The availability of ILD multidisciplinary teams (MDT) involved in the care and transition were rather variable between countries. 20 (51%) of all responding centres reported availability of an established MDT. Pulmonologists or paediatric pulmonologists were the most involved members, with a radiologist, and a pathologist also being present in most countries. In paediatric centres (28) a pathologist skilled in chILD was often not available (nine positive answers, 32%). There was better availability of a radiologist skilled in chILD (14 centres, 50%). In adult centres (11) the situation was slightly better, specialist pathologists were available in five (45%) centres and a skilled radiologist available in seven (64%). A specialised nurse, nutritionist or dietitian were present less often. In two (5%) centres, a nurse was listed as the main member of the team without further specification. 19 (68%) paediatric centres routinely involved a psychologist in the care for children with serious chronic diseases and 34 (87%) of all centres involved physiotherapists. In only ten (26%) centres, there was routine formal co-operation between paediatric and adult ILD experts to guarantee smooth transition.
The age of transition from paediatric to adult healthcare was mostly 18 years, ranging from 16 to 21 years. There was a high variability in the answer about how long before the actual transition the transition process starts. This varied between 3 months to 4 years, with 1 year being most frequent.
Only three (11%) paediatric centres used a standard operating procedure (SOP) for the transition of patients with chILD to adult care, and five (18%) centres mandated diagnostic re-evaluation before transition. Nine (32%) centres had a standardised medical report form that accompanied the patient during the transition process.
Only four (14%) paediatric centres routinely organised a pre-transition meeting with the patient, parents and both the paediatric and adult teams, nine (32%) centres had a meeting between paediatric and adult teams without patient/parents, five (18%) paediatric centres organised a meeting of the paediatric team with patient/parents. Only two (18%) adult centres had an established system of long-term follow-up of patients with remitted chILD.
Main results of the survey from the paediatric (chILD) centres are shown in figure 2.

{kind=link}
{kind=link}
Summary of main survey results in paediatric centres. chILD: childhood interstitial lung disease; EUR REG: centres participating in the European registry (chILD-EU); REG: centres participating in another registry; PATH: skilled pathologist available; RAD: skilled radiologist available; SOP: standard operating procedure available; MEDREP: standardised transition medical report; AGESPEC: follow up for age-specific chILD established.
Based on the survey outcomes, the need for standardisation of the transition of chILD patients to adult care was obvious. Therefore, based on the discussion within the WG5, we have proposed a transition pathway to address this and we hope it will be widely applicable.
Proposal for the transition process
The objectives were to: 1) set up a standard protocol to ensure that paediatric and adult pulmonologists work together to maintain the continuity of specialised care for chILD patients; 2) standardise the individual steps in the process of transitioning paediatric patients to adult care - preparing the patient for transition, the actual transition process; and 3) define the minimal content of the transition medical report.
As chILD is much rarer and more heterogeneous than other chronic respiratory diseases in childhood, any universal transition protocol must be tailored for any individual patient.
Transition to adult care should be seen as a gradual process and should take place over a period of time (usually one year). The preparation of a patient for transition is the responsibility of the paediatric pulmonologist. Especially in complex cases, a paediatric psychologist should be involved. Finding a suitable adult pulmonology department to provide follow-up care is the next prerequisite for successful handover. The geographical accessibility of the centre also plays a role, but expertise and knowledge of the ILD centre must be the most important consideration. For the actual handover, a proper transition medical report must be prepared, containing clinical and laboratory information about the patient.
During transition, the young person will take over the responsibility for his/her health from parents or other caregivers. The nature of the disease, its current status and expected development and possible complications must be clearly grasped by the young person to ensure their sufficient cooperation. The following aspects should be highlighted: 1) the disease may still be active, or relapse with serious medical consequences; 2) there may be long term, as yet unappreciated complications of the disease (e.g. the obstructive lung disease reported after NEHI) [3]; 3) the disease and/or its treatment (especially corticosteroids) may impact on normal lung development; 4) there may be occupational implications of the disease and/or its treatment; and 5) there may be genetic implications for the young person who may want to start a family
Assessment of possible risk-taking behaviour, which is more common in children and young people with a chronic disease (e.g. HEADSS: Home, Education, Activities/employment, Drugs, Suicidality, Sex [6, 7]).
Transition from chILD centre
The patient should be re-assessed in detail during the last year of the follow-up at the chILD centre. The clinical status and functional evaluation should always be done and also radiologic ((chest) high resolution computer tomography (HRCT)) investigation should be considered depending on the specific diagnosis and activity of the disease. The transition process should be started in cooperation with the parents of the patient and a summary transition protocol created.
The format of the transition report may vary, but should always include the following information, most of which have already been gathered (see also OLS):
Age at diagnosis of chILD and first clinical symptoms leading to diagnosis along with all pertinent diagnostic tests (see 5. below)
Precise diagnosis and estimation of prognosis
Detailed data:
perinatal history
other morbidity; severe infections, need for ventilation support etc.
vaccinations, reactions after vaccination
exposure to external risk factors (smoking, allergens, chemicals and other toxins, environmental pollution, occupation exposure in adolescents; school and work), past and present
school, (considered) job preferences with regard to possible exposure to external risk factors
familial occurrence of risk factors (a full genogram should be prepared); miscarriage and still birth, death in neonatal/infant period; unexplained respiratory distress, sepsis, as well as occurrence of ILD in first- and second-degree relatives, especially in combination with hematopoietic disorders, liver, brain or thyroid disease, malignancies before the age of 35.
social and psychological history (social background, cooperation, adherence to the treatment regime, possible psychological problems, understanding of the disease and its acceptance)
Results of previous examinations relevant to the diagnosis and their development over time:
Physical examination, including anthropometric measurements, digital clubbing, any chest deformity
result of cardiological examination, if relevant; indirect signs of pulmonary hypertension, systemic hypertension
imaging; especially HRCT
lung function (spirometry, body plethysmography, diffusion capacity, objective assessment of exercise tolerance and its evolution over time, cardiopulmonary exercise testing; if available); see OLS
serological and genetic testing
result of bronchoscopic examination including results of bronchoalveolar lavage - differential count of leukocytes and their immunophenotyping, presence of haemosiderin laden macrophages, lipid laden macrophages, CD1a positive cells…
result of lung biopsy; age at examination, method and anatomical site of biopsy (side and lobe), microscopic finding including histopathological classification.
Clinical course of the disease; occurrence of acute pulmonary exacerbations, their triggers, method of treatment, development of lung function and laboratory findings with regard to the progression of lung disease
Current and past treatment:
pharmacological treatment (duration and response); systemic corticosteroids, other immunosuppressive agents; azathioprine, mycophenolate mofetil, (cyclophosphamide), hydroxychloroquine, azithromycin, possibly antifibrotics in a clinical study (active substance, dose, duration of treatment)
side effects of medication
non-pharmacological treatment; home oxygen therapy, respiratory physiotherapy, other treatment methods (diet…)
- densitometry, bone metabolism,
- oral glucose tolerance test
- ophthalmological examinations
Patient's perspective; important issues of the disease as perceived by the patient him/herself
Summary
Communication with ILD center for adults, MDT re-evaluation
In parallel with summarising the chILD patient's data for transition, the appropriate adult ILD centre should be identified. The selected adult ILD team is contacted and the first consultation is planned, optimally including the patient and parents. After this first visit and check, it is essential to make a therapeutic and follow-up plan.
Discussion
In this survey, we have found that even though the provision of care for children with ILD is generally adequate, for most paediatric centres there is no formal transition pathway to adult care. In this regard, the ILD community lags far behind, for example, systems of care for patients with cystic fibrosis. The reason probably lies in the paucity of cases of chILD and lack of systematic approach and centralisation in comparison with the cystic fibrosis care. Even in large paediatric respiratory centres chILD is very rare. As many of the chILDs may remit in childhood, either spontaneously or after treatment, the need for proper long-term follow up and systematic transition to adult care is not perceived as important as with some other diagnoses. This omission that may lead to missing some of the relapsing or slowly progressive cases. Although generic pathways such as “Ready, Steady, Go” [8] and the use of HEADSS [12, 13] to guide consultations are useful in transitioning any young person, there are child-specific issues which are not captured, despite the fact that late sequelae of some chILDs have already been documented [3, 14, 15]. Furthermore, there may be genetic implications if the young person elects to start a family. Many chILDs and their implications are unfamiliar to adult physicians, who see many totally different forms of ILD, and there is a big risk of interruption of care after transition. This needs urgently to be addressed, and we have proposed a pathway to alleviate this. Another important aspect of transition is to highlight patients in whom the diagnosis is not yet certain. The significance of previously uncertain genetic variants of ILD may become clear, and new disorders are being identified, some of which may have specific treatments. These patients should therefore have a diagnostic review at transition and regularly thereafter in the adult clinic.
To our knowledge, this is the first attempt to determine clinical practice in transition of chILD patients across Europe. The main weakness is that it relied on questionnaire data and thus physician recall, and also that the return rate of the questionnaire was incomplete and some of the questions were not answered by all the respondents. Nevertheless, 39 centres from 21 countries submitted data, and this is likely to represent the reality of practice across Europe. We fully acknowledge, that the suggested transition protocol is based on expert opinion and needs validation. We have reported an initial step, that should stimulate further research and enable later refinements of this protocol. As the availability of long-time follow up data of chILD patients will increase with increasing availability of data from the emerging registries, management of chILD in adults and guidance of transition care will be enhanced.
Conclusion
Transitional care in chronic respiratory diseases is an important yet underappreciated aspect of appropriate and complex health care. The situation in chILD patients is complicated by their rarity, heterogeneity and limited availability of evidence. Our multicentre survey showed virtually no guidelines for transition. Within COST Action CA16125 EnTER chILD WG5 expert opinion based protocol was suggested to improve the transitional care in chILD patient and highlight its importance for later health and long-term prognosis. The next step is for pan-European consortia to test whether this approach is helpful, or alterations are needed.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00964-2020.SUPPLEMENT
Acknowledgements
The authors wish to thank Suzanne Terheggen-Lagro, Dept of Pediatric Pulmonology, Academic Medical Center Amsterdam, Amsterdam, the Netherlands, for providing valuable supportive material for preparing the transition scheme.
Footnotes
This article has supplementary material available from openres.ersjournals.com
Author contributions: P. Pohunek, M. Vašáková and A. Bush contributed equally to the design of the survey and to the evaluation of the results. V. Koucký, P. Pohunek, M. Vašáková and A. Bush contributed equally to writing the manuscript, its editing and preparing of the final version of the submission. All authors agree with the final version of the manuscript.
Support statement: This study was supported as part of the COST Action CA16125 EnTER chILD. The work of V. Koucký and P. Pohunek was supported by the Ministry of Health, Czech Republic – Conceptual Development of Research Organisation (University Hospital Motol, 00064203). Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: V. Koucký has nothing to disclose.
Conflict of interest: P. Pohunek has nothing to disclose.
Conflict of interest: M. Vašáková reports grants and personal fees from F. Hoffmann La Roche, and personal fees from Boehringer Ingelheim, outside the submitted work.
Conflict of interest: A. Bush has nothing to disclose.
- Received December 21, 2020.
- Accepted February 13, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org










