





Abstract
Background: Infection control measures for coronavirus disease 2019 (COVID-19) might have affected management and clinical state of patients with COPD. We analysed to which extent this common notion is fact-based.
Methods: Patients of the COSYCONET cohort were contacted with three recurring surveys (COVID1, 2 and 3 at 0, 3 and 6 months, respectively). The questionnaires comprised behaviour, clinical and functional state, and medical treatment. The responses to the questionnaires were compared amongst themselves and with pre-COVID information from the last visit of COSYCONET.
Results: Overall, 594 patients were contacted and 375 patients (58% males, forced expiratory volume in 1 s (FEV1) 61±22% predicted) provided valid data in COVID1 and COVID2. Five patients reported infections with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Most patients – except for patients with higher education – reported compliance with recommended protective measures, whereby compliance to hygiene, contact and access to physicians slightly improved between COVID1 and COVID2. Also, patients obtained more information from physicians than from public media. In the majority of cases, the personal physician could not be substituted by remote consultation. Over time, symptoms slightly increased and self-assessed physical capacity decreased. Results of COVID3 were similar. Women and patients with more exacerbations and dyspnoea avoided medical consultations, whereas Global Initiative for Chronic Obstructive Lung Disease (GOLD) D patients were more amenable to tele-consultation.
Conclusion: In well-characterised COPD patients, we observed on average slight deteriorations of clinical state during the period of COVID-19 restrictions, with high and partially increasing adherence to protective measures. The data suggest that in particular, women and GOLD D patients should be actively contacted by physicians to identify deteriorations.
Abstract
During the period of #COVID19 restrictions, slight deteriorations of clinical state with increasing adherence to protective measures were observed. In particular, women and GOLD D patients are at risk of deterioration. https://bit.ly/2S7fhEo
Introduction
On March 11, 2020, coronavirus disease 2019 (COVID-19) was declared a pandemic and on March 22, 2020 Germany declared its first lockdown. Even though no general curfew was enacted, restrictions regarding personal contacts were imposed. While treating COVID-19-positive patients and tracing relevant contacts, the public health system tried to uphold medical care as much as possible. Patients with COPD are considered a risk group for severe COVID-19 courses [1, 2]. At the same time, these patients regularly require care from specialised clinics or practices. Therefore, public infection control measures can not only have beneficial effects, but also adverse effects on COPD patients, especially when access to medical care, physiotherapy and pulmonary exercise groups is limited by such public measures [3, 4].
A cross-sectional investigation of the experiences of COPD patients during Spain's first lockdown indicated only a low impact of disease control measures on their disease [4]. However, with the prolongation and tightening of such measures as the pandemic progressed, effects on the disease status may have become more pronounced over time. A detailed analysis of long-term changes and their impact on individual clinical history is not available yet but may be useful to improve the management of COPD patients in a pandemic.
The aim of the present study was to monitor the impact of the COVID-19 pandemic on COPD patients through repeated surveys. The focus of the surveys was placed on patients’ behaviour, potential limitations of medical treatment and burdens of the disease, including depression scores. The study was conducted within the COSYCONET framework (COPD and Systemic Consequences–Comorbidities Network) between May 2020 and February 2021 and comprised three consecutive assessments. The relation to COSYCONET offered the opportunity to link questionnaire data to individual pre-COVID information on lung function, comorbidity profile and psychological status.
Methods
Study population
Patients of the German COPD cohort COSYCONET, which is a multi-centre study focusing on the role of comorbidities in COPD [5], and participating at visit 6 (6 years after recruitment) were contacted by mail and asked to respond to a specifically designed COVID-19 questionnaire (see supplementary material). The COVID-19 questionnaire included questions to capture patient behaviours such as hygiene measures, disease-specific behaviour, physician and physical therapy visits, use of video and telephone consultations, health status and physical activity. Details on COSYCONET, its inclusion/exclusion criteria and assessments have been published previously [5]. Fifteen study centres participated in this sub-study, whereas five could not participate due to logistic reasons during the pandemic. The COVID-19 questionnaire was at three intervals (at 0, 3 and 6 months). The mailing of the COVID-19 questionnaire started from May to July 2020, August to October 2020, and November 2020 to January 2021 for the assessments scheduled at 0, 3 and 6 months, respectively. After return of the questionnaires, the data base was finalised in February 2021. The collection of data over a 6-month period aimed to map potential long-term behavioural and health status-related changes during the evolving pandemic. The three consecutive questionnaires are referred to as COVID1, COVID2 and COVID3. The primary analysis focused on patients who returned at least COVID1 and COVID2, as the number of participants dropped from 564 in the first to 381 in the second to 241 in the third iteration of the survey; the latter is only shown in a secondary analysis.
The COSYCONET study has been approved by the ethical committees of all study centres, and all patients gave their written informed consent [5]. The additional examination of patients with the COVID questionnaire was also approved by the Ethics Committee (COSYCONET study, Amendment 11, AZ 200/09). The COSYCONET study was conducted in accordance with the Declaration of Helsinki.
Assessments
During the regular visits of the COSYCONET study, a detailed recording of all COPD-specific characteristics, demographics, comorbidities, medication, generic and disease-specific quality of life, and psychological disorders was performed [5]. Lung function was assessed following the standard operating procedures of COSYCONET in accordance with guidelines [6, 7]. The assessments included forced expiratory volume in 1 s (FEV1) and its ratio (FEV1/FVC) to forced vital capacity (FVC), as well as diffusing capacity of the lung for carbon monoxide (CO) in terms of transfer factor (TLCO) and transfer coefficient of the lung for carbon monoxide (KCO). Predicted values for spirometry and diffusing capacity were taken from the Global Lung Function Initiative (GLI) [8, 9]. On the basis of the lung function at the time of recruitment, we also determined the annual decline of lung function over the follow-up visits prior to the COVID-19 pandemic, to be able to assess the potential link between the responses to the questionnaire and the decline in lung function.
Symptom burden was evaluated by using the disease-specific COPD Assessment Test (CAT) and the Modified Medical Research Council (mMRC) dyspnoea scale [10, 11]. The Patient Health Questionnaire Depression Scale 9 (PHQ-9) was used as a tool for screening depression [12]. Education was categorised in three groups based on the number of years of education completed (basic education ≤9 years, secondary education 10–11 years, higher education >11 years) [13]. We used data of the COSYCONET visit 6 for comparison with pre-pandemic measurements. The median time interval between visit 6 and the first COVID survey was 1.6 years.
COVID-19 restrictions in Germany
In Germany, the first lockdown was declared on March 22, 2020. The restrictions included control measures such as social distancing and limitations of personal contacts, and accordingly hospitality, recreational and cultural facilities were shut. These restrictions were attenuated between May and October 2020 on a local basis, due to the decrease in the daily number of cases. From April 29, 2020 onwards, the wearing of face masks had become compulsory in public transport sytstems, schools and shops. During the first lockdown, non-urgent physician visits in both outpatient and inpatient settings were cancelled by the healthcare providers, postponed or replaced by telephone visits. In the time between May and November 2020, the German healthcare system's capacity was at no time exhausted, and all healthcare services could be offered to the fullest extent. The second wave of the pandemic led to a further lockdown (called “Lockdown Light”), which was declared on November 2, 2020. Several cultural and business institutions were shut down again, but the school system was initially kept open. These measures were tightened on December 13, 2020 and were still in place at the end of our survey. However, the second lockdown did not lead to a general reduction in healthcare services, and elective surgical procedures were postponed only in individual hot-spot areas owing to increased utilisation of intensive care units.
Statistical analyses
Regarding baseline characteristics of the study population and dropouts, differences between groups were identified using chi-square tests for categorical variables and analysis of variance (ANOVA) for continuous variables. To analyse changes in CAT, PHQ-9 and mMRC scores prior to versus during the pandemic and over the course of the pandemic, mean values were compared using pairwise t-tests. Additionally, the PHQ-9 categories “healthy to severe depression” [12] were compared using Wilcoxon signed-rank tests for dependent samples.
The questions in the COVID questionnaire had to be answered on a 5-item scale with the response options 1=“does not apply at all” to 5=“fully applies”. Differences in the distribution of responses between COVID1 and COVID2 were analysed by histograms and Wilcoxon signed-rank test for dependent samples. To analyse the responses from COVID1 to COVID 3, the nonparametric Friedman test for repeated measures was used. Furthermore, we investigated the dependence of responses in COVID1 on several patient characteristics using chi-square tests. Statistical analyses were performed using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA), and p-values of ≤0.05 were considered statistically significant.
Results
Study population
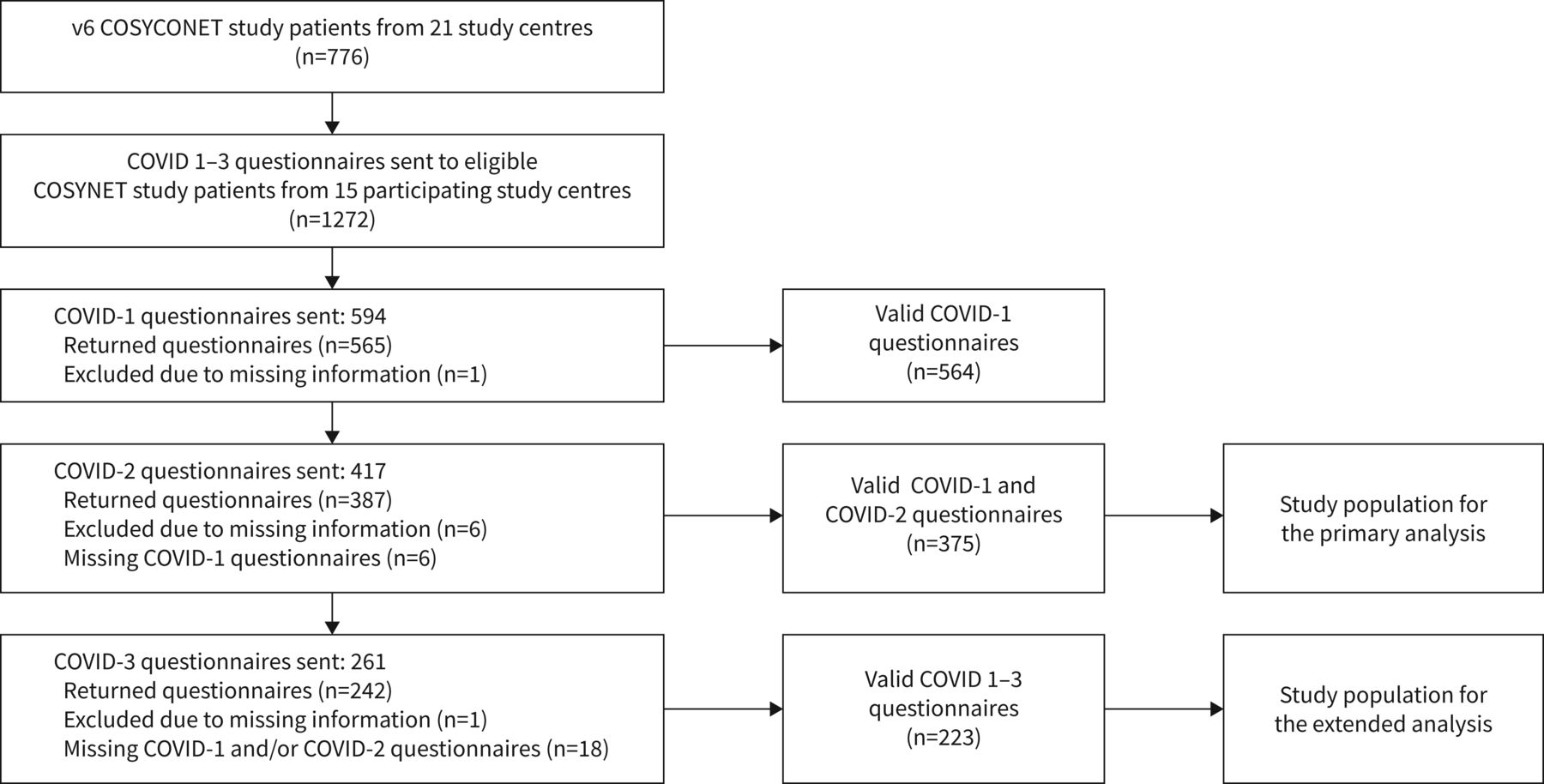
Overall, 594 patients from 15 study centres were contacted, of whom 565 (95%) responded to at least one questionnaire. In total, we received 1186 complete COVID-19 questionnaires, 565 COVID1, 381 COVID2 and 241 COVID3. Complete responses to COVID 1 and COVID 2 were available for 375 patients, and 223 patients returned all three questionnaires. For purposes of the primary analysis, we defined the 375 patients as study population who returned both the COVID1 and COVID2 questionnaire (see figure 1, consort diagram). Five out of all 565 patients reported to have been diagnosed with COVID-19.

CONSORT flow chart of coronavirus disease 2019 (COVID-19) survey study participants. The questionnaires were only sent out again by the study centres if the first or second questionnaire was returned. Furthermore, owing to the increasing capacity bottlenecks caused by the COVID-19 pandemic, not all study centres were able to send out the questionnaires at the third timepoint. This led to differences in the number of questionnaires sent out on each occasion.
Table 1 shows patients’ characteristics obtained at the COSYCONET visit 6, i.e. prior to COVID, and stratified according to the study population and the excluded patients. Significant differences between groups were found for the frequencies of gastrointestinal disorders, asthma and treatment with oral corticosteroids (p<0.05, each), whereas the distribution of sex, age, Global Initiative for Chronic Obstructive Lung Disease (GOLD) grades and groups, and educational status was not different.
Baseline characteristics
Results of the repeated surveys
The comparison of COVID1 and COVID2 revealed a small increase in total CAT score (p<0.05), specifically CAT item 3 (chest tightness). The increase in mMRC score was not statistically significant. For PHQ-9, COVID2 showed a higher proportion of the upper three categories, due to an increase in mild depression (p<0.05; table 2).
Changes in COPD Assessment Test (CAT), Patient Health Questionnaire Depression Scale 9 (PHQ-9) and Modified Medical Research Council (mMRC) scores
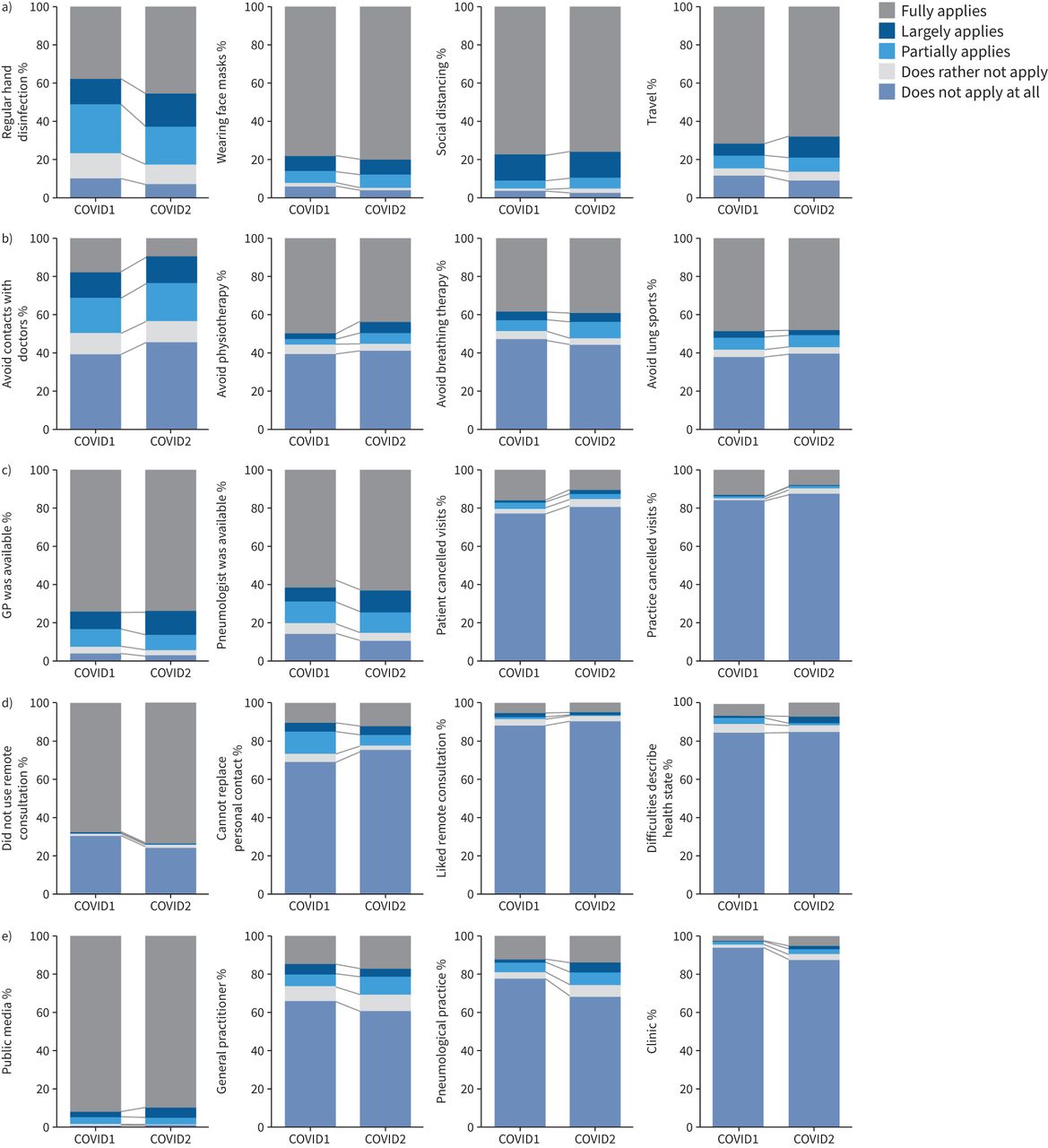
Individual measures of hygiene
Figure 2a shows the results regarding individual measures of hygiene, i.e. hand disinfection, use of face masks, social distancing and dispensing with travels. The only apparent change between COVID1 and COVID2 was the higher adherence to hand disinfection in the second questionnaire; there was an increase of 7% in the answer “fully applies” for “regular hand disinfection”.
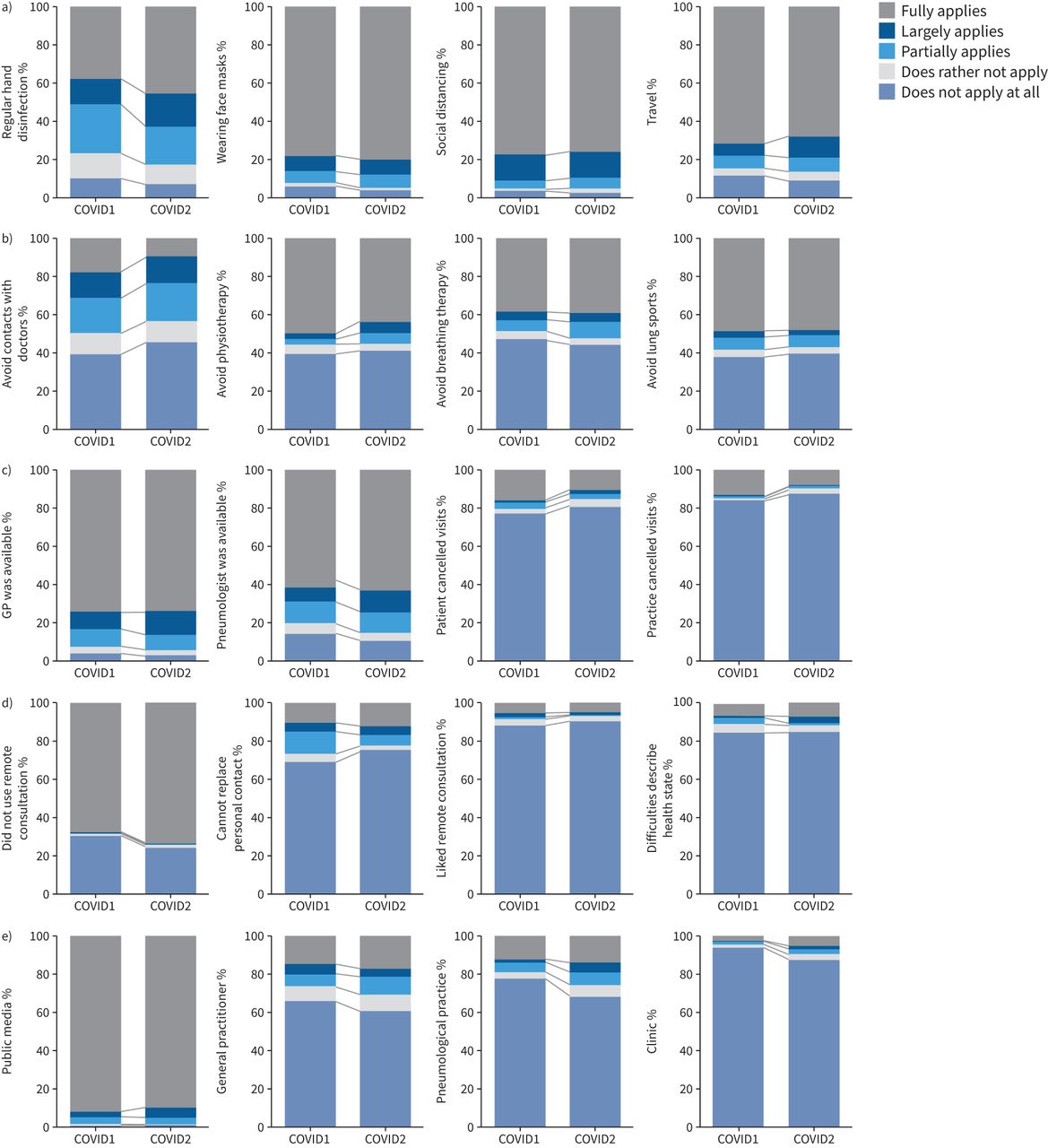
Repeated surveys regarding patients’ behaviour. Results of COVID1 and COVID 2 regarding individual measures of hygiene (a), disease-specific behaviour (b), access to medical care (c), video or telephone consultation (d) and information on infection control measures (e). Answers range from “does not apply at all” to “fully applies”.
Disease-specific behaviour
Figure 2b shows the results relating to the avoidance of physicians’ practices, physiotherapy, breathing therapy and pulmonary exercise groups. Interestingly, the level of avoidance of physicians’ practices decreased in COVID2. While 16% of patients gave their full agreement for “avoidance of contact to practices” in COVID1, only 10% of patients gave this answer in COVID2.
Access to practices
Figure 2c shows the results regarding the availability of physicians and specialists as well as the possibility to arrange for appointments at practices. Most patients reported a high accessibility to general practitioners and pulmonologists. Only a minority of patients and practices cancelled scheduled visits, and the number of cancelled visits (answer “fully applies”) decreased from 13% in COVID1 to 8% in COVID2.
Video or telephone consultation
Figure 2d shows the results regarding the frequency of tele-consultation, the attitude towards such consultation and its estimated effectiveness. The majority of patients did not use tele-consultation (68% in COVID1 and 74% in COVID2), did not consider tele-consultation as a suitable substitute for consultation in person (69% in COVID1 and 75% in COVID2) and did not, generally, favour tele-consultation (88% in COVID1 and 91% in COVID2).
Information on infection control measures
Figure 2e shows the results regarding the source of information on infection control measures. Whereas the percentage of patients relying on public media has been high throughout and only slightly decreased in COVID2, the reliance on general practitioners, pneumologists and pneumological clinics as sources of information increased from COVID 1 to COVID2.
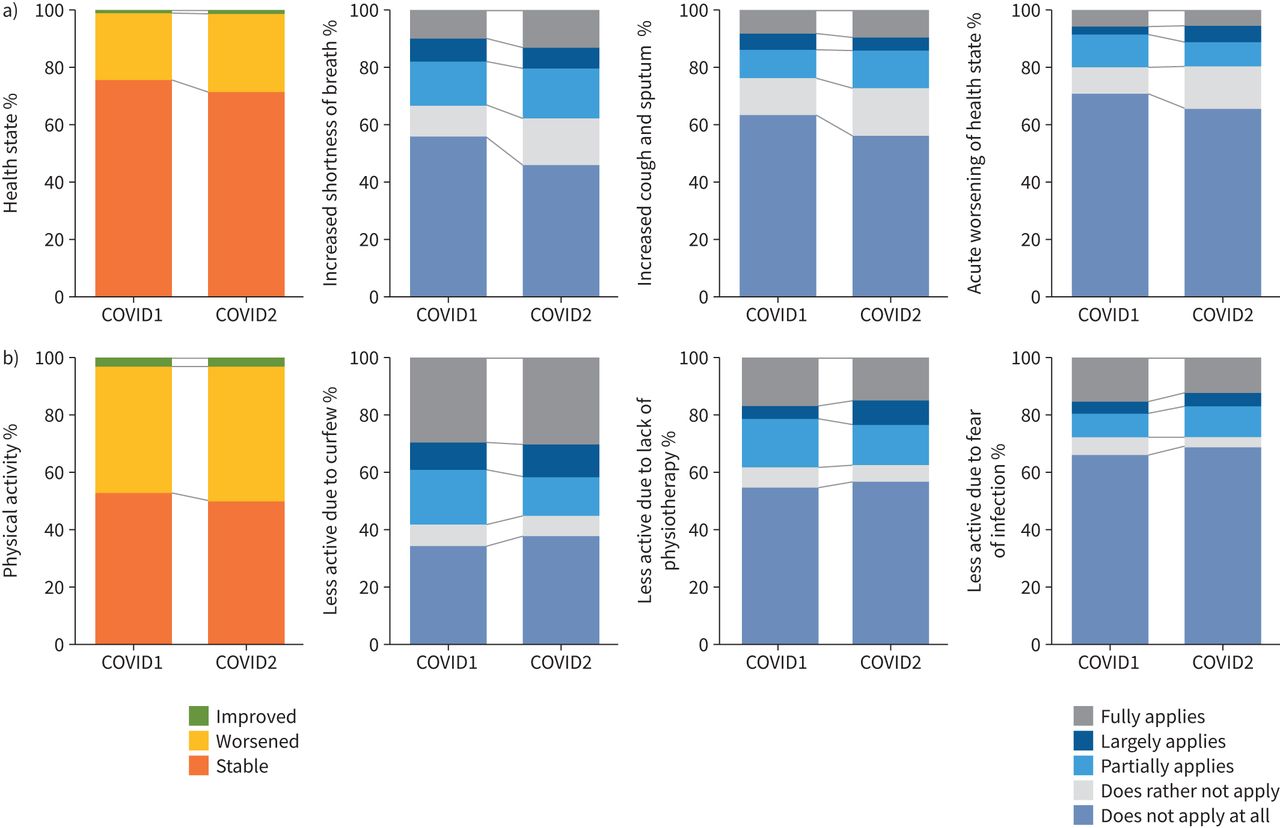
Course of COPD
Figure 3a shows symptoms and clinical state. Overall, from COVID1 to COVID2 patients reported increased dyspnoea (cough and deteriorations in form of exacerbations), as well as a deterioration of their general clinical state. The number of patients who reported no increase in dyspnoea decreased from 56% to 46%, and the number of patients who reported low cough complaints decreased from 64% to 56%. Furthermore, the proportion of patients reporting a stable general health status decreased from 76% to 71%.

Repeated surveys regarding health status and physical activity. Results of COVID1 and COVID 2 regarding the course of COPD: a) health status and b) physical activity. Answers range from “does not apply at all” to “fully applies”.
Physical activity
Figure 3b shows physical activity as self-reported in COVID1 and COVID2. Reductions of general physical activity were attributable to the restrictions on free movement and scheduled physiotherapy. However, there were only minor changes between COVID1 and COVID2 with an increase of 3% of patients reporting low general physical capacity. Regardless, general physical capacity was generally considered lower by patients.
Additional changes in the COVID3 assessment
When extending the scope of assessments to COVID3, we observed stable results for most of the items presented above, except for general physical capacity and physical condition, which significantly deteriorated, as reflected in increased cough and dyspnoea (see figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Additional changes in the COVID3 assessment. Answers for “increased cough and sputum production” range from “does not apply at all” to “fully applies”.
When repeating the comparison of COVID1 and COVID2 responses for this subpopulation, the results were compatible with those initially reported, especially for higher adherence to hand disinfection, less avoidance of contact to practices and increasing level of accessibility to general practitioners and pulmonologists for COVID2 compared to the COVID1 answers.
Relationship between pre-COVID state and COVID1 results
Responses to COVID1 were in a first step compared with the last COSYCONET visit and in a second step with the responses to COVID2 (table 2). The comparison between pre-COVID and COVID 1 showed a slight increase of total CAT score (p<0.05), corresponding to increases in CAT items 4, 6 and 8 (dyspnoea/stairs, confidence leaving home and energy), and a decrease in CAT item 3 (chest tightness). Accordingly, mMRC was higher and the relative frequency of elevated PHQ-9 scores (upper three categories) was higher, as reflected in higher rates of moderate and severe depression (table 2). Further information on the comparison of physical characteristics and specific COVID survey items, as well as their relationship to the annual decline of lung function, can be found in the supplementary material.
Discussion
In the present study, we assessed the impact of infection control measures against COVID-19 on medical treatment, protective behaviour, symptoms, exacerbations and clinical state of COPD patients. We also analysed whether the results depended on the individual clinical history, which was possible as the study was performed within the long-term COSYCONET follow-up framework. Overall, patients showed high adherence to protective measures and over time increasingly relied on information from medical professionals. Generally, adherence was higher in women, but interestingly, adherence was lower in patients with higher education. Symptoms slightly increased and self-estimated physical capacity decreased over time. The negative impact of infection control measures on the clinical state was stronger in patients with a history of frequent exacerbations, while the adherence of such patients to the measures partially even decreased. Similar results were observed for patients with comorbidities described as risk factors for COVID-19, such as diabetes, obesity or coronary artery disease. Although changes were small, these findings indicate deteriorations of self-reported clinical state in patients with COPD despite an increasing adherence to protective measures against COVID-19.
In our study cohort, only a small fraction of patients was amenable to tele-consultations. For the vast majority, personal contact with physicians was still important. This was reflected in the tendency over the course of the study to obtain more information from physicians and increase face to face contact with them. This suggests that irrespective of the advantages of remote care, patients rely on the personal contact with physicians at regular intervals, especially as there are differences between physicians and patients regarding the perception and evaluation of clinical state [14]. On the other hand, in our study COPD patients with high symptom burden and exacerbation risk reported avoiding contact with physicians in favour of tele-consultation. This indicates that remote care should be tailored to the specific needs of a certain group of patients.
While several studies reported that the number of exacerbations leading to hospitalisation decreased during the COVID pandemic [15, 16], two studies showed an increase or at least frequent exacerbations during the first phase of COVID-19 in the UK and Spain [4, 17]. Our data showed an increase in symptoms indicative of mild exacerbations. This may result from different definitions. Also, stronger protection against infectious agents may have prevented moderate and severe exacerbations, whereas the reduction in medical care led to a slight deterioration over time. Despite reductions in medical care, patients did not report increased impediments to access respiratory medication and denied a decrease in the quality of respiratory care (see supplementary figure S1). The numbers of appointments cancelled by either physicians or patients also decreased over time, which indicates that both sides got accustomed to the new situation. Regardless, the self-reported physical capacity of the patients decreased, in accordance with objective measurements [18].
The assumption that the protective measures against COVID-19 were effective is in line with the observation that only five of 564 patients became infected with COVID-19. Considering that severe exacerbations are known to have a major impact on the course of the disease [3, 19], it could be argued that in the future COPD patients might benefit from some of the protective measures established during the pandemic, such as a careful selection of contacts and the wearing of face masks under specific conditions. While a previous analysis of COSYCONET data showed an association between better lung function and higher educational status [13], the present study found lower levels of adherence to infection control measures among patients with higher education. This should be considered when advising patients on infection control measures.
Limitations
Owing to the low number of patients with COVID-19, our data does not allow to draw conclusions on the impact of this disease in COPD. By contrast, the data reflects the impact of protective measures against COVID-19 on these patients, which is particularly relevant for the majority of our study population who did not suffer from COVID-19. Although the initial response rate to the questionnaires of 95% was rather high, the number of responses decreased with each iteration of the questionnaire, especially between COVID2 and COVID3 (see table 1). Except for a higher prevalence of asthma, gastrointestinal disorders and the use of oral corticosteroids, the characteristics were very similar between the dropouts and the patients having at least the first two assessments. Regarding the occurrence of increased symptoms and deteriorations compatible with mild exacerbations, we had to rely on patients’ answers as we naturally could not include functional measurements or physical examinations that were avoided by a significant number of patients. The assessment of single CAT items has not been validated so far. Nevertheless, we analysed the single CAT items as a proxy of COPD-specific symptoms, which was shown to be an effective approach in previous COSYCONET investigations [20]. This also allowed a direct comparison of the pre-COVID and COVID era.
Conclusion
When monitoring the potentially disease-relevant behaviour and clinical state of well-characterised COPD patients from May 2020 to the beginning of 2021 through the responses to three repeated questionnaires, we observed slight deteriorations of clinical state and self-reported exercise capacity despite high and partially increasing adherence to the protective measures and at the same time decreasing limitations in the access to medical care. According to most patients, the personal treatment by physicians could not be adequately substituted by remote care. However, women and COPD patients with high symptom burden and exacerbation risk reported an increased avoidance of personal contacts with physicians, while all patients did not favour tele-consultation. Therefore, the results suggest that in particular women and GOLD D patients should be actively contacted by the physician for the diagnosis of deteriorations.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00242-2021.SUPPLEMENT
Survey questionnaire 00242-2021.questionnaire
Figure S1 00242-2021.figureS1
Acknowledgements
We are grateful to the COSYCONET study group and study centres that contributed in patient recruitment and data collection, as well as to all patients participating in this study.
Footnotes
COSYCONET study group: Andreas, Stefan (Lungenfachklinik, Immenhausen); Bals, Robert Universitätsklinikum des Saarlandes); Behr, Jürgen and Kahnert, Kathrin (Klinikum der Ludwig-Maximilians-Universität München); Bahmer, Thomas (Universitätsklinikum Schleswig-Holstein) and Bewig, Burkhard (Städtisches Krankenhaus Kiel); Ewert, Ralf and Stubbe, Beate (Universitätsmedizin Greifswald); Ficker, Joachim H. (Klinikum Nürnberg, Paracelsus Medizinische Privatuniversität Nürnberg); Grohé, Christian (Ev. Lungenklinik Berlin); Held, Matthias (Klinikum Würzburg Mitte gGmbH, Standort Missioklinik); Behr, Jürgen and Henke, Markus (Asklepios Fachkliniken München-Gauting); Herth, Felix (Thoraxklinik Heidelberg gGmbH); Kirsten, Anne-Marie and Watz, Henrik (Pneumologisches Forschungsinstitut an der Lungenclinic Grosshansdorf GmbH); Koczulla, Rembert (Schön Klinik Berchtesgadener Land); Kronsbein, Juliane (Berufsgenossenschaftliches Universitätsklinikum Bergmannsheil, Bochum); Kropf-Sanchen, Cornelia (Universitätsklinikum Ulm); Herzmann, Christian (Forschungszentrum Borstel); Pfeifer, Michael (Klinik Donaustauf); Randerath, Winfried J. (Wissenschaftliches Institut Bethanien e. V., Solingen); Seeger, Werner (Justus-Liebig-Universität Gießen); Studnicka, Michael (Uniklinikum Salzburg); Taube, Christian (Ruhrlandklinik gGmbH Essen); Timmermann, Hartmut (Hamburger Institut für Therapieforschung GmbH); Alter, Peter, Schmeck, Bernd and Vogelmeier, Claus (Universitätsklinikum Gießen und Marburg GmbH, Standort Marburg); Welte, Tobias (Medizinische Hochschule Hannover); Wirtz, Hubert (Universitätsklinikum Leipzig)
Study nurses: Doris Lehnert, Evangelische Lungenklinik Berlin; Birte Struck, Bergmannsheil Berufsgenossenschaftliches Universitätsklinikum Bochum; Lenka Krabbe, Medizinische-Klinik Borstel; Barbara Arikan, Julia Tobias, Klinik Donaustauf; Gina Spangel, Julia Teng, Ruhrlandklinik gGmbH Essen; Kornelia Speth, Universitätsklinikum Gießen; Jeanette Pieper, Universitätsmedizin Greifswald; Margret Gleiniger, Britta Markworth, Zaklina Hinz, Petra Hundack-Winter, Pneumologisches Forschungsinstitut Großhansdorf; Ellen Burmann, Hamburger Institut für Therapieforschung Hamburg; Katrin Wons, Sylvia Wagner Medizinische Hochschule Hannover; Ulrike Rieber, Beate Schaufler, Thoraxklinik am Universitätsklinikum Heidelberg; Martina Seibert, Universitätsklinikum des Saarlandes, Homburg/Saar; Katrin Schwedler, Lungenfachklinik Immenhausen; Sabine Michalewski, Sonja Rohweder, Universitätsklinikum Schleswig-Holstein, Campus Kiel; Patricia Berger, Universitätsklinikum Leipzig; Diana Schottel, Krankenhaus Lindenbrunn, Coppenbrügge; Manuel Klöser, Universitätsmedizin der Johannes Gutenberg-Universität Mainz; Vivien Janke, Universitätsklinikum Marburg; Rosalie Untsch, Asklepios Fachkliniken, München-Gauting; Jana Graf, Klinikum der Universität München; Anita Reichel, Klinikum Nürnberg; Gertraud Weiß, Erich Traugott, Barbara Ziss, Schön Klinik Berchtesgadener Land; Ilona Kietzmann, Wissenschaftliches Institut Bethanien für Pneumologie e.V, Solingen; Michaela Schrade-Illmann, Beate Polte, Universitätsklinikum Ulm; Cornelia Böckmann, Gudrun Hübner, Lena Sterk, Anne Wirz, Klinikum Würzburg Mitte gGmbH, Standort Missioklinik, Würzburg.
This article has supplementary material available from openres.ersjournals.com
The COSYCONET framework is registered at www.clinicaltrials.gov with identifier number NCT01245933 [5]. The basic data are and available upon request. There is a detailed procedure for this at www.asconet.net. Specifically, the data can be obtained by submission of a proposal that is evaluated by the steering committee. All results to which the manuscript refers to are documented by the appropriate in the text, figures or tables.
Ethics approval and consent to participate: All assessments were approved by the central (Ethikkommission FB Medizin Marburg) and local (Bad Reichenhall (Ethikkommission bayerische Landesärztekammer); Berlin (Ethikkommission Ärztekammer Berlin); Bochum (Ethikkommission Medizinische Fakultät der RUB); Borstel (Ethikkommission Universität Lübeck); Coswig (Ethikkommission TU Dresden); Donaustauf (Ethikkommission Universitätsklinikum Regensburg); Essen (Ethikkommission Medizinische Fakultät Duisburg-Essen); Gießen (Ethikkommission Fachbereich Medizin); Greifswald (Ethikkommission Universitätsmedizin Greifswald); Großhansdorf (Ethikkommission Ärztekammer Schleswig-Holstein); Hamburg (Ethikkommission Ärztekammer Hamburg); MHH Hannover/Coppenbrügge (MHH Ethikkommission); Heidelberg Thorax/Uniklinik (Ethikkommission Universität Heidelberg); Homburg (Ethikkommission Saarbrücken); Immenhausen (Ethikkommission Landesärztekammer Hessen); Kiel (Ethikkommission Christian-Albrechts-Universität zu Kiel); Leipzig (Ethikkommission Universität Leipzig); Löwenstein (Ethikkommission Landesärztekammer Baden-Württemberg); Mainz (Ethikkommission Landesärztekammer Rheinland-Pfalz); München LMU/Gauting (Ethikkommission Klinikum Universität München); Nürnberg (Ethikkommission Friedrich-Alexander-Universität Erlangen Nürnberg); Rostock (Ethikkommission Universität Rostock); Berchtesgadener Land (Ethikkommission); Schmallenberg (Ethikkommission Ärztekammer Westfalen-Lippe); Solingen (Ethikkommission Universität Witten-Herdecke); Ulm (Ethikkommission Universität Ulm); Würzburg (Ethikkommission Universität Würzburg)) ethical committees, and written informed consent was obtained from all patients. The additional examination of patients with the COVID questionnaire was also approved by the Ethics Committee (COSYCONET study, Amendment 11, AZ 200/09).
Consent for publication: Within the ethical approval the participants of the study gave their consent to publish the data collected during the study period.
Conflict of interest: K. Kahnert has nothing to disclose.
Conflict of interest: J.I. Lutter has nothing to disclose.
Conflict of interest: T. Welte reports grants from German Ministry of Research and Education during the conduct of the study.
Conflict of interest: P. Alter has nothing to disclose.
Conflict of interest: J. Behr has nothing to disclose.
Conflict of interest: F. Herth has nothing to disclose.
Conflict of interest: H-U. Kauczor reports other support from Bayer and Siemens during the conduct of the study; and personal fees and other support from Philips, and personal fees from AstraZeneca, Merck Sharp Dohme and Boehringer Ingelheim, outside the submitted work.
Conflict of interest: S. Söhler has nothing to disclose.
Conflict of interest: M. Pfeifer has nothing to disclose.
Conflict of interest: H. Watz has nothing to disclose.
Conflict of interest: C.F. Vogelmeier reports grants, personal fees and other support from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline and Novartis, personal fees and other support from CSL Behring, Chiesi, Grifols and Nuvaira, and personal fees from Berlin Chemie, outside the submitted work.
Conflict of interest: R. Bals reports grants from BMBF during the conduct of the study; COSYCONET is supported by the German Centre for Lung Research (DZL) grant number 82DZLI05A2 (COSYCONET), German Federal Ministry of Education and Research (BMBF) grant number 01GI0881, and is furthermore supported by unrestricted grants from AstraZeneca GmbH, Boehringer Ingelheim Pharma GmbH & Co. KG, GlaxoSmithKline GmbH&Co. KG, Grifols Deutschland GmbH, and Novartis Deutschland GmbH; and grants and personal fees from AstraZeneca and Boehringer Ingelheim, personal fees from GlaxoSmithKline and Grifols, grants and personal fees from Novartis, personal fees from CSL Behring, grants from BMBF Competence Network Asthma and COPD (ASCONET), Sander Stiftung, Schwiete Stiftung, Krebshilfe and Mukoviszidose eV, outside the submitted work; and a leadership or fiduciary role in the Alpha-1-Center.
Conflict of interest: R.A. Jörres has nothing to disclose.
Conflict of interest: F.C. Trudzinski has nothing to disclose.
Support statement: This investigation was supported by Chiesi GmbH. The study was conducted within the COSYCONET framework. COSYCONET is supported by German Centre for Lung Research (DZL) grant number 82DZLI05A2 (COSYCONET), BMBF grant number 01GI088,1 and is furthermore supported by unrestricted grants from AstraZeneca GmbH, Boehringer Ingelheim Pharma GmbH & Co. KG, GlaxoSmithKline GmbH&Co. KG, Grifols Deutschland GmbH, and Novartis Deutschland GmbH. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received April 8, 2021.
- Accepted June 8, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










