





Abstract
Introduction COPD affects the small airways and is associated with ventilation heterogeneity. There are little data on the multiple-breath washout (MBW) in patients with COPD, particularly the variability over 8 weeks, using a shortened sulfur hexafluoride (SF6) washout. This work evaluated the repeatability of the lung clearance index (LCI)1/40 and LCI1/20 among subjects with COPD and compared to spirometry and clinical markers.
Methods The MBW was performed on patients with COPD to determine ventilation heterogeneity globally (LCI), at conductive (Scond) and acinar (Sacin) levels. The LCI was repeated in triplicate and measured at a traditional 1/40th washout and retrofitted to a shortened 1/20th end tidal SF6 concentration washout. Tests were repeated after 20 min and 8 weeks to determine within and between visit repeatability and compared with spirometry.
Results Eighty-four subjects were recruited to perform LCI and spirometry with 20 subjects performing the repeatability protocol. There were weak correlations between forced expiratory volume in 1 s ( FEV1) per cent predicted and LCI1/40th r=−0.311 (p=0.02), and LCI1/20th r=−0.40 (p<0.01). The LCI demonstrated excellent within and good between visit repeatability for both a 1/40th and 1/20th washout (intraclass correlation coefficient (ICC)≥0.80). There was a statistically significant strong correlation between LCI1/40th and a shortened LCI1/20 of 0.86 (p<0.01).
Conclusions The LCI is repeatable within and between visits. There are weak correlations with measures of spirometry. A shortened LCI1/20th starting concentration correlates highly with a 1/40th washout, which may encourage clinical use.
Abstract
It is feasible to shorten the LCI to a 1/20th washout in patients with COPD, and this leads to a time saving of 32% and therefore may allow for easier use in clinical settings https://bit.ly/3v9UsXd
Introduction
COPD is a small airways disease leading to gas mixing abnormalities [1]. The multiple-breath washout (MBW) test is used to determine the lung clearance index (LCI), and further analysis of phase III slopes may enable partitioning of conductive and acinar zone heterogeneities (Scond/Sacin) [2, 3]. A recent study identified that LCI measured with sulfur hexafluoride (SF6) as a tracer gas was sensitive to early disease in patients with COPD that had preserved spirometry [4]. It is therefore possible that LCI is a useful early disease and therapeutic biomarker in COPD.
Recently standardisation of the MBW technique has been reported to enable comparison across clinical studies and standardised reporting [5]. LCI is calculated by measuring the number of turnovers of functional residual capacity (FRC) to reduce the end tidal tracer gas concentration (Cet) to 1/40th of its original concentration. The termination point of the test requires at least three consecutive breaths to have a Cet<1/40th. Although the 1/40th stopping point is traditionally deployed in testing, its choice is arbitrary and often mandates longer testing times in patients with established lung disease, e.g. COPD.
Given that, the Association of Respiratory Technology and Physiology (ARTP, UK based) suggests that high-quality spirometry takes ∼20 min, a shortened LCI to ≤20 min may be more appealing [6]. The combination of reduced testing time and greater disease sensitivity could render LCI a clinically viable tool in COPD management. Additionally, the use of the LCI as a primary outcome in COPD interventional studies is limited and could be increased with knowledge of required sample sizes.
A recent study in cystic fibrosis identified that shortening of the LCI led to significant test time saving without compromising the accuracy of the test [7]. LCI1/20th was shown to have high intra-test repeatability and accuracy for cystic fibrosis discrimination from health when compared to LCI1/40th. Similar results have been observed in asthma, where LCI1/20th demonstrated a similar within-visit coefficient of variation and diagnostic sensitivity compared to the 1/40th test [8].
We hypothesised that a shortened (1/20th) LCI is as repeatable as conventional LCI (1/40th) both within visit and over 8 weeks in patients with established COPD. Eight-week repeatability was used to generate sample size calculation for experimental medicine studies with LCI1/40th as an outcome measure. Furthermore, we aimed to explore the correlation of LCI1/20th with clinical markers of COPD, specifically Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage spirometry and COPD Assessment Test (CAT) scores.
Methods
This study was performed at the NIHR Biomedical Research Centre – Respiratory at the University Hospital of Leicester, UK during 2017–2018. This study was part of a larger feasibility and randomised controlled trial (ISRCTN 81979106 and ISRCTN45695543); ethical approval was obtained by the National Health Service Health Research Authority and Local Research Ethics Committee (17/EM/0156). Participants were recruited through research databases and outpatient COPD and Pulmonary Rehabilitation clinics and were representative of patients with COPD attending secondary care. Patients were ≥40 years old with a confirmed diagnosis of COPD in accordance with the 2017 Global Initiative for Lung Disease (GOLD) recommendations [12]. This includes a current smoking history of ≥10 pack-years with at least one of the following symptoms: productive cough, dyspnoea or wheeze and evidence of airflow obstruction (forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC) ratio of <0.7). Patients were included irrespective of their smoking status.
MBW was measured using a modified photoacoustic Innocor® device as manufactured by Innovision ApS, Denmark. This is an open circuit using 0.2% SF6 during wash-in and room air for the washout phase. The MBW was performed in line with the European Respiratory Society/American Thoracic Society recommendations [5]. In upright sitting, participants were instructed to perform tidal breathing (7–12 mL per kg of their weight) for the duration of the test with a nose clip in situ and performed in triplicate. The procedure was performed at baseline (V1) repeated after a 20-min interval (V2) to determine within-visit repeatability and again after an 8-week interval (V3) to determine between-visit repeatability of the MBW. Analysis was performed using a custom MATLAB algorithm (software version Open_analysis_12 m) updated November 25, 2016. A modification was made to the coding to identify when the concentration reached <1/20th starting concentration over three tidal breaths. The phase III slope analysis was programmed between 1.5 and 6 turnovers of FRC to enable a reliable calculation of Scond; this has been previously reported in the literature [9]. At least two tests must be within 10% of the highest FRC to be included in the analysis. The LCI is calculated as the cumulative exhaled volume/FRC. The mean averages of the included tests were used at each time point. Phase III slope analysis was performed to determine the Scond and Sacin measurements with Scond calculated by a pooled slope analysis, using the pooled breaths from each included test per time point (two or three tests depending on FRC variability). A previously reported two-compartment lung washout model was used to generate LCIvent (ventilation) and LCIds (dead space) with a view to understanding the relative contribution of these factors to LCI. The model outputs report proportional increase in LCI above its ideal value due to specific ventilation inequality (LCIvent) or due to increased respiratory dead space (LCIds) [9, 13]. Shortening the LCI to a 1/20th washout was performed in the data analysis phase for direct test comparisons; this was performed using a customised MATLAB algorithm and used a predefined 1/20th cut-off (of three consecutive breaths) and corresponding FRC from the 1/20th washout.
Spirometry was performed according to the European Respiratory Society/American Thoracic Society recommendations using a Vitalograph Alpha touch spirometer. The 2012 Global Lung Initiative reference values were used [14]. Spirometry was performed as a screening tool prior to the first MBW and again on participants’ second visit prior to their final MBW, ∼1 h before MBW testing. The peak test was used for the analysis as this is an effort-dependent test. Participant's height and weight were collected in order to calculate spirometry per cent predicted measures and body mass index (BMI). LCI and spirometry were performed at the same time of day across the two visits.
Data were analysed using SPSS statistics for Windows V25 (IBM, New York, USA) (version 24). Correlations between LCI and spirometry were performed using Pearson's correlations. Repeatability of the LCI and spirometry was determined by using Cronbach's α and is presented as an intraclass correlation coefficient (ICC). ICC was calculated using a two-way mixed effects analysis of absolute agreement for single raters. A correlation coefficient of <0.5, between 0.5 and 0.74, between 0.75 and 0.9 and values above 0.9 are considered poor, moderate, good and excellent repeatability, respectively [15]. Bland–Altman plots were derived and assessed for systematic bias [16, 17]. A one-way ANOVA with post hoc tests (Tukey's) was used to assess the LCI and GOLD staging and a negative binomial regression was used in the exacerbation analysis. There was no formal power calculation for this study; however, a minimum of 20 subjects were required for the repeatability data analysis.
Results
Clinical study populations
Eighty-four subjects with COPD were recruited to complete MBW-SF6, spirometry and CAT scores. A sub-set of 20 subjects completed repeatability analysis of LCI1/40th and ICI1/20th over 8 weeks (table 1). Clinical characteristics of the study populations are outline in table 1.
Clinical characteristics of study populations
LCI repeatability
Nineteen out of 20 completed the protocol and were eligible for repeatability analysis, and 80 out of 84 tests in the correlation cohort were suitable for analysis (5% fell outside of acceptable±10% variation of FRC). Baseline characteristics can be seen in table 1. The LCI1/20th showed good repeatability both within and between visits (8-week) (ICC ≥0.8). This was comparable to LCI1/40th and FEV1 (table 2). In addition, the between visit repeatability of LCI1/20th was comparable to spirometry. Sacin phase III slope measures were also repeatable (ICC≥0.80) within and between visit; however, Scond measures were not repeatable over 8 weeks in keeping with previous observations in asthma [9]. There is a poor ICC for LCIvent and LCIds between visits (0.10 and 0.05, respectively). The LCIvent and LCIds were calculated to assess the proportionate changes in ventilation and dead space. The measured LCIds was 1.37 (0.32) and LCIvent 1.59 (0.23). There was a 2% decrease and 11% increase in LCIvent and LCIds, respectively. The coefficient of variation for the LCI1/40th was 15% and for the LCI1/20th was 12%. The mean per cent change within-visit (V1 and V2) was −1.12% for the LCI1/40th and −2.18% for the LCI1/20th and r between visit (V1 and V3) was −1.39% for LCI1/40th and −3.24% for LCI1/20th.
Intraclass correlation coefficients for within and between visit measures of the lung clearance index
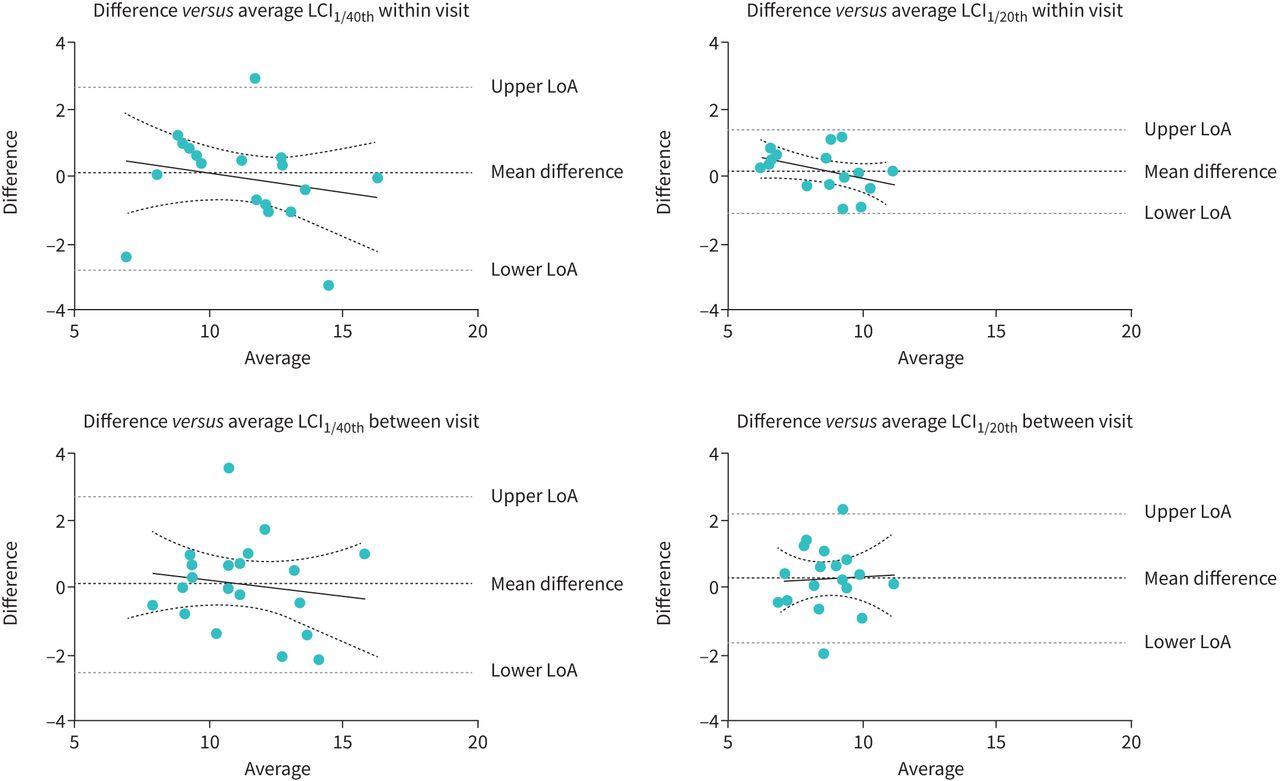
Bland–Altman plots demonstrating potential proportionate systematic bias for LCI1/40th and LCI1/20th are presented in figure 1.

Bland–Altman plots for lung clearance index (LCI)1/40th and LCI1/20th within and between visits. Bland–Altman plots for LCI1/40th within visit repeatability, LCI1/20th within visit repeatability, LCI1/40th between visit (8 week) repeatability and LCI1/20th between visit (8 week) repeatability. LoA: limits of agreement 95% confidence interval.
LCI 1/20th did not demonstrate significant systematic measurement bias both within visit and between visit over 8 weeks (within-visit bias slope (mean±sd) 0.19±0.6), p=0.13, R2=0.16, between visit bias slope (mean±sd) 0.29±0.98, p=0.85, R2<0.01). Numerical bias slopes were small and similar for LCI1/20th and LCI1/40th within and between visits (LCI1/40th within-visit bias slope (mean±sd) −0.07±1.40, p=0.44, R2=0.04, between-visit bias slope (mean±sd ) 0.15±1.35, p=0.56, R2=0.02).
Relationship between LCI1/40th and LCI1/20th
In keeping with an earlier study [4] in COPD, LCI1/40th and LCI1/20th were highly correlated with numerically smaller values for LCI1/20th, Pearson correlation of 0.86 (p<0.01), 1. The LCI1/40th and LCI1/20th Bland–Altman plots show a bias slope of 3.02 (0.70). There were statistically significant proportionate biases when comparing LCI1/40th and LCI1/20th; however, the magnitude of this was small (p<0.01, R2=0.26) (figure 2).
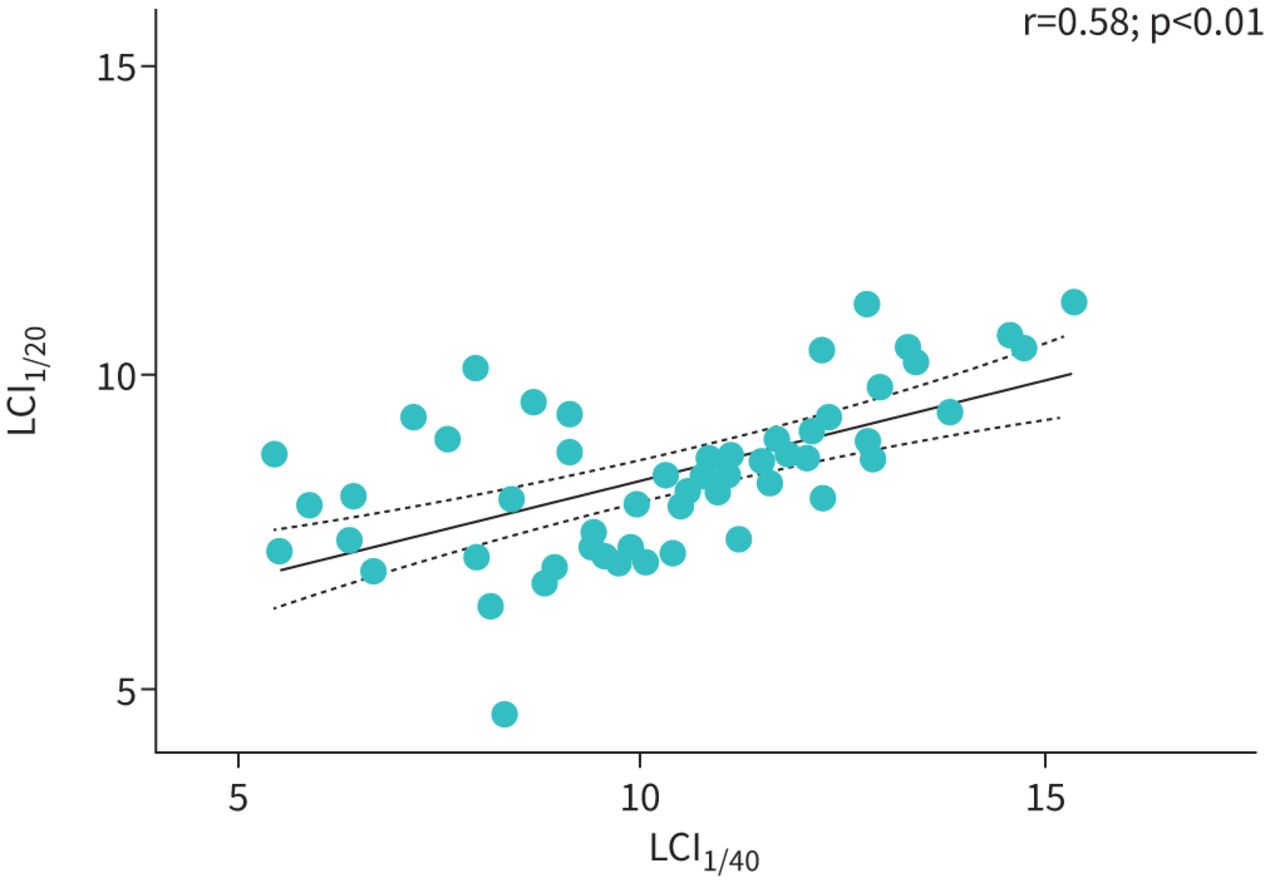
Correlations between lung clearance index (LCI)1/20th and LCI1/40th washout test. Correlations between lung clearance index and 1/40th and 1/20th washout concentrations. Plotted with a line of best fit and the confidence intervals (dotted line).
Testing time and clinical feasibility of LCI1/20th
The mean±sd test time for a 1/40th washout test was 3.40±1.55 min (204±93 seconds) and 10.22±4.63 min (613±278 seconds) if performed in triplicate. A shortened washout to 1/20th starting concentration has a mean±sd test time of 2.33±1.02 min (140±61 seconds) or 7.00±3.05 min (420±183) if performed in triplicate, using a 1/20th washout results in a shortened test of 31.5% than a 1/40th washout test. All patients with COPD were able to perform a triplicate LCI test; however, n=1 was unsuitable for analysis as it was outside the accepted variance of 10%.
Sample size estimate for experimental medicine studies
There is no known minimal clinically important difference (MCID) available for the LCI in COPD. We have therefore estimated the treatment effect with LCI as an outcome measure in an experimental medicine study based on mean group changes above the reported limits of agreement.
Table 3 shows the sample size estimates based on superiority at 80% and 90% powered (ß) and a 5% Type I error (α) using standard deviations seen in our within-visit and 8-week repeatability cohort study (2.25 and 2.03, respectively). The power calculations were based on the mean change above the limits of agreements. σ is the standard deviation.

Sample size calculation for within and between visit (V) study designs
Clinical association studies of LCI1/20th and spirometry GOLD stage
LCI1/20th and LCI1/40th were associated with COPD GOLD spirometry stage (figure 3, table 4). There were no significant differences between GOLD staging and Scond or Sacin.

{kind=link}
{kind=link}
{kind=link}
Correlations between forced expiratory volume in 1 s (FEV1) % predicted and a) lung clearance index (LCI)1/20th, b) LCI1/40th, c) Scond conducting zone and d) Sacin acinar zone. Correlations between measures of multiple-breath washout and forced expiratory volume in 1 s per cent predicted (FEV1 %). GOLD: Global Initiative for Chronic Obstructive Lung Disease.
One-way ANOVA for COPD GOLD staging
Correlation matrix of LCI1/20th and other physiological indices
There were statistically significant strong correlations between LCI1/20th and LCI1/40th, which remained significant with multivariate linear regression. There were weak correlations with LCI1/20th, LCI1/40th and spirometry properties, which were statistically significant (p<0.01 and p=0.02, respectively) (table 5).
Univariate correlation of LCI1/20th and physiological indices
LCI /20th association with CAT, mMRC symptoms scores and exacerbation frequency
There were no significant differences for the LCI1/20th stratified by their mMRC score or CAT total score. There were no significant correlations between symptoms (mMRC or CAT) with LCI1/20th (0.21 and 0.20, respectively). Participants were stratified on severity of MRC (>3) and CAT (>10) and analysed using receiver operating characteristics. The area under the curve stratified by MRC score for the LCI1/20th was 0.50, LCI1/40th 0.41 and FEV1 % predicted 0.61. The area under the curve for the CAT total score for LCI1/20th is 0.35, LCI1/40th 0.45 and FEV1 % predicted 0.73. Negative binomial regression demonstrated no association between exacerbation frequency in the year prior to the first study visit and LCI (data not shown).
Discussion
This study explores the use of the LCI across all severities of patients with COPD as the use of a potential outcome measure. The aims of this study were to understand the repeatability of using a shortened MBW within a study visit and over 8 weeks. Testing was conducted across the range of COPD severities without test failure or dropout. The performance of the MBW can be affected if patients experience a chronic, irritable cough, and this may explain some of the tests that were excluded from the analysis; this was also the case in patients with bronchiectasis [10].
In order to use the LCI as a potential therapeutic outcome measure, it is necessary to understand repeatability. The repeatability was assessed following a 20-min rest period within visit and after 8 weeks, as these are common time points in therapy treatment. The use of the LCI1/40th, LCI1/20th, FRC, Scond and Sacin were all highly repeatable after 20 min of rest. The LCI1/40th, LCI1/20th, FRC and Sacin were highly repeatable over an 8-week period; however, there was moderate–poor repeatability of the Scond and LCIvent over this time period. This may be explained by the instrument noise associated with this measure or variability in the condition and is similar to results seen in patients with asthma [9]. The LCI1/20th demonstrated an increased variability compared to LCI1/40th when comparing relative change and coefficient of variance between visits. This may be due to the reduced testing time that limits the assessment of the smaller airways and that could be assessed on a 1/40th washout; however, the ICC for both the LCI1/40th and LCI1/20th were similar at 8 weeks (0.88 and 0.80, respectively). The use of LCI using a nitrogen washout has demonstrated an increased LCI in patients with mild to moderate COPD, which is comparable to the data shown in this work [4]. Compared to healthy control literature on LCI, the patients in this study demonstrated an increased LCI; however, this literature is predominantly in a younger population than this study. Grillo et al. [10] demonstrated an LCI of 7.36±0.99 in patients with bronchiectasis a mean±sd age of 49.9±13.42. Age can increase the LCI, which may have contributed to the increased LCI in this study; however, it is likely that the level of airflow obstruction predominantly contributed to this increase [18, 19]. The coefficient of variation of the LCI1/40th was higher than reported in the literature, which could be due to the inclusion of all disease severities from GOLD stage one through to four [4]. Analysis of the LCIvent and LCIds using a previously reported two-compartment model enabled exploration of ventilation and dead space contributions to ventilation heterogeneity [13]. We observed poor within and between visit repeatability of these measures. There are a number of plausible explanations for this observation. A two-compartment model assumes that the LCI can be described by the weighted sum of two exponential decay rate constants, whereas in COPD there may be many heterogeneous compartments all emptying according to their own rate constants due to altered local parenchymal tissue mechanics as a consequence of emphysema, small airways disease and mucous plugging. The poor within visit repeatability of both Scond and LCIvent/LCIds in this study could also be explained by stochastic variation of peripheral airway diameters and acinar volumes in COPD or, both [17].
We observed similar repeatability with a 1/20th test to the traditional 1/40th washout. This was demonstrated through the analysis phase, and therefore testing would need to occur prospectively with a shortened test (stopping at 1/20th of the wash-in gas concentration) to demonstrate the feasibility of performing a shortened washout. The shortening of the multiple-breath washouts may improve its clinical application [6]; however, as this study performed LCI1/20th in the analysis phase, the duration of a shortened wash-in has not been explored. The use of a shortened LCI to 1/20th of the starting concentration has been shown to be feasible and repeatable in patients with cystic fibrosis [11]. Shortened LCI tests have been shown to be sensitive in patients with cystic fibrosis compared to healthy controls [7]; however, there are few studies that explore the response of the LCI1/20th in COPD or in response to an intervention in these conditions [10].
Power calculations using the repeatability study data have established potential sample sizes for LCI as an end-point which are relatively modest and support the use of LCI as a potential mechanistic or secondary end-point in trials designed to target ventilation heterogeneity. The use of a shortened LCI may reduce the sensitivity, and therefore its application should be justified by the specific research or clinical question [11].
Our study has several potential limitations. The conduction of spirometry an hour before MBW testing may affect the washout, and the impact of this was not explored in this study. There is a weak correlation between MBW measures and clinical outcomes as measured by the CAT, mMRC score and prior exacerbation frequency. The CAT and mMRC are subjective measures of symptoms that are influenced by biological, psychological and social factors. Whilst a worsened LCI may indicate an increased severity of diseased lung and greater disease heterogeneity within the lung, it is not a direct measure of clinical severity and does not account for other factors that can contribute to patient symptoms in COPD. Additionally, reporting of prior exacerbations is variable, and subject to recall bias. Our study did not confirm exacerbation events through primary care record analysis of rescue pack medication. Future work could evaluate the LCI across COPD treatment strata that are classified by both symptoms (mMRC or CAT scores) and exacerbation frequency.
The results of this work support the use of the LCI as a potential tool in experimental medicine studies targeting ventilation heterogeneity in patients with stable COPD. Our demonstration of high within and between visit repeatability of LCI1/20th suggests that prospective use of this marker needs to be explored in clinical studies of COPD to identify clinically important treatment effect sizes alongside testing feasibility.
Footnotes
Author contributions: E. Daynes: protocol development, data collection, data analysis and manuscript preparation. N. Greening: protocol development, data analysis and review of the manuscript. J. Owers-Bradley: data analysis and review of the manuscript. S. Singh: protocol development and review of the manuscript. S. Siddiqui: protocol development, data analysis and review of the manuscript.
This study is registered at www.isrctn.com with identifier number ISRCTN45695543. Individual anonymised participant data will be shared between 9 and 36 months after publication for the purposes of meta-analysis. Proposals may be submitted up to 36 months following publication by contacting the corresponding author, after which, you will be redirected to another researcher that may be able to help with your query. Data will be made available upon reasonable request to the authors.
Conflict of interest: E. Daynes reports that Actegy Ltd funds a commercial trial from which the present data were obtained.
Conflict of interest: N. Greening has nothing to disclose.
Conflict of interest: J. Owers-Bradley has nothing to disclose.
Conflict of interest: S. Singh reports that Actegy Ltd funds a commercial trial from which the present data were obtained.
Conflict of interest: S. Siddiqui reports advisory boards for and speaker fees from AstraZeneca, GSK, Novartis, Roche, Boehringer Ingelheim, Owlstone Medical, Mundipharma and ERT Medical, outside the submitted work.
Support statement: This study is supported by the National Institute for Health Research (NIHR). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. This study was funded by Actegy Ltd. Funding information for this article has been deposited with the Crossref Funder Registry.
- Received June 15, 2020.
- Accepted May 16, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










