





Abstract
Background Risks associated with video-assisted surgical lung biopsy (VASLB) for interstitial lung disease (ILD) with endotracheal intubation and mechanical ventilation are not nil. Awake video-assisted surgical lung biopsy (Awake-VASLB) has been proposed as a method to obtain a precise diagnosis in several different thoracic diseases.
Objectives To compare clinical outcomes of Awake-VASLB and Intubated-VASLB in patients with suspected ILDs.
Methods From June 2016 to February 2020, all patients submitted to elective VASLB for suspected ILD were included. Differences in outcomes between Awake-VASLB and Intubated-VASLB were assessed through univariable, multivariable-adjusted, and a propensity score-matched analysis.
Results Awake-VASLB was performed in 66 out of 100 patients, while 34 underwent Intubated-VASLB. The Awake-VASLB resulted in a lower post-operative morbidity (OR 0.025; 95% CI 0.001–0.35; p=0.006), less unexpected intensive care unit admission, less need for rescue therapy for pain, a reduced surgical and anaesthesiologic time, a reduced chest drain duration, and a lower post-operative length of stay.
Conclusion Awake-VASLB in patients affected by ILD is feasible and seems safer than Intubated-VASLB.
Abstract
Awake surgical lung biopsy in patients affected by ILD is feasible and safer than intubated surgical lung biopsy https://bit.ly/2SnMATh
Introduction
Interstitial lung diseases (ILDs) include a number of pulmonary diseases, either restricted to lungs or characterised by pulmonary involvement of a systemic disease. They are grouped together because of similar clinical, radiographic, physiological or pathological features and are classified as idiopathic or secondary (related to a known aetiology). Among the idiopathic ILDs, the most frequent and severe is idiopathic pulmonary fibrosis (IPF) [1]. It follows that IPF should be confirmed or excluded in all subjects presenting with unexplained progressive dyspnoea, chronic cough, and/or Velcro-like crackles on chest examination, especially if aged ≥65 years. Moreover, early and accurate diagnosis of IPF is advisable because its natural history, treatment options, and prognosis greatly differs even in the context of ILDs. In particular, anti-fibrotic drugs have proved most effective in IPF and in a subgroup of other ILDs with a clear demonstrated progressive fibrosing pattern [2, 3]; early application of appropriate treatment reduces either disease progression or even allows a better quality of life [4, 5]. In other words: an early and highly confident diagnosis is always the key to good clinical practice. In the meantime, particular attention must be paid to optimising the risk–benefit ratio of the diagnostic procedures employed.
The diagnosis of IPF can be obtained in most cases with high-resolution computed tomography (HRCT) scan evidence of definite usual interstitial pneumonia (UIP) pattern [1, 6]. Alternatively, the results of clinical evaluation, laboratory tests, imaging and pulmonary function tests are often discussed in a multidisciplinary team (MDT) setting, eventually deciding whether surgical biopsy is deemed necessary or not.
Histological diagnosis can be obtained by transbronchial biopsy, transbronchial cryobiopsy, or surgical lung biopsy (SLB), either through thoracotomy or by video-assisted surgical lung biopsy (VASLB). The American Thoracic Society clinical practice guidelines suggest the use of SLB in patients with newly detected ILD of unknown cause, clinically suspected of having IPF and displaying an HRCT pattern of probable UIP, indeterminate for UIP, or an alternative diagnosis [1]. There is increasing awareness that a considerable proportion of histological confirmed UIP had a previous HRCT pattern of “inconsistent UIP” and “alternative diagnosis”.
Undeniably, VASLB with endotracheal intubation and mechanical ventilation is associated with a risk of mortality and morbidity that is far from nil [7, 8]. Nevertheless, in recent years a VASLB approach performed in awake subjects under loco-regional anaesthesia (Awake-VASLB) has been suggested as an effective method to obtain a highly confident diagnosis in several different thoracic diseases [9].
Given that post-anaesthesia burden not negligible, especially in fragile patients, there is clear evidence in the literature that avoidance of neuromuscular blocking agents [10], intra- and post-operative strong opioids [11], and injurious mechanical ventilation [12–14] could improve outcomes.
The objective of the present study was to compare the clinical outcomes of Awake-VASLB and Intubated-VASLB in patients undergoing SLB for suspected ILDs.
Methods
All patients undergoing elective pulmonary biopsy via video-assisted thoracoscopic surgery (VATS) for suspected ILD in the Department of Thoracic Surgery of the ‘Città Della Salute e Della Scienza’ University Hospital in Torino (Italy) between June 2016 and February 2020 were enrolled. The decision to approach the procedure using Intubated-VASLB or Awake-VASLB followed a multidisciplinary discussion including the thoracic surgeon, anaesthesiologist and pulmonologist. Exclusion criterion was the precognition of difficult endotracheal intubation.
The study protocol was approved by local Institutional Review Boards.
Awake-VASLB anaesthesia management
Local anaesthesia was induced in all cases with aerosolised Lidocaine 10 mL (20 mg·mL−1). Sedation from 2 to 3 on the Ramsay Scale was obtained through a target-controlled infusion of propofol (mean target 0.8 μg·mL−1) and remifentanil 0.05 μg·kg−1·min−1. Oxygen was administered through an air-entrainment mask (oxygen saturation measured by pulse oximetry (SpO2) target >92%). Arterial pressure was invasively monitored in all cases. Locoregional anaesthesia was achieved through epidural catheter or local injection of lidocaine 2% 20 mL performed by the surgeon under direct vision supplemented, when needed, with subsequent bolus of 10 mL of local anaesthetic. After the collapse of the lung on the surgical side induced by artificial pneumothorax, the inhaled oxygen concentration was set to maintain SpO2 >90%.
Intubated-VASLB anaesthesia management
Following intravenous remifentanil 0.05–0.15 μg·kg−1·min−1 ideal body weight (IBW), propofol 1.5–2 mg·kg−1 recommended body weight (RBW) and rocuronium 0.6–1.2 mg·kg−1 adjusted body weight (ABW), a double-lumen tracheal tube was inserted under direct laryngoscope use as soon as train-of-four (TOF)=0. Breathing parameters on a Dräger Zeus anaesthesia machine (Drägerwerk AG & Co., Lübeck, Germany) were set as tidal volume (VT) 6–8 mL·kg−1 IBV during dual lung ventilation and VT 4–6 mL·kg−1 IBW and respiratory rate as 12–14 times per min during one-lung ventilation, respiration rate according to arterial blood gases or end-tidal carbon dioxide tension, in volume-controlled ventilation mode. Positive end-expiratory pressure was always set at 5 cmH2O. Arterial pressure was invasively monitored in all cases. Anaesthesia was maintained through inhaled desflurane 0.8–1.3 times minimum alveolar concentration (MAC), remifentanil 0.05–0.15 μg·kg−1·min−1, and rocuronium according to neuromuscular monitoring (moderate block). Sugammadex was routinely given for antagonisation.
Post-operative management
In both groups, lung recruitment manoeuvres were performed according to Tusman protocol [15]. After the procedure, patients were discharged to the ward with a standardised therapy consisting of paracetamol 1 g i.v. every 8 h. Rescue therapy for pain (e.g. ketorolac, parecoxib or tramadol, as appropriate) was administrated in the case patients complained of pain grade 3 or more according to the numeric rating scale. Chest radiography was routinely performed on post-operative day 1 and after chest drain removal. Chest drain removal included favourable chest radiograph, no air-leak for at least 24 h, overall fluid output not higher than 250 mL per day, and drained fluid neither chylous nor haemorrhagic [16].
Patients’ discharge was planned for the day after chest tube removal if no clinical or radiological contraindications were observed.
Statistical analysis
Baseline patient characteristics are summarised by the mean and standard deviation or number and percentages, as appropriate. Between-group differences were evaluated by t-test (continuous variables) or Chi-squared test or Fisher's exact test (categorical variables), as appropriate.
As the aim of the study was to have at least 90% power to detect a decrease of the 90% post-operative complication incidence after VASLB reported in the literature (25%) [17, 18], a sample size of at least 99 patients (enrolment ratio 2:1) was computed (significance level of 0.05). The secondary outcomes were chest drain duration, unexpected intensive care unit (ICU) admission (defined as a non-scheduled admission to ICU after the surgical procedure), reintervention, post-operative death (i.e. at 30 days from surgery), rescue therapy administration for pain, hospital length of stay, number of biopsies achieved, and surgical and anaesthesiologic time.
Univariable and multivariable-adjusted logistic regression models were used to evaluate categorical outcomes, while different continuous outcomes were compared by means of the unpaired Wilcoxon–Mann–Whitney test.
The variables in the adjusted models were age, sex, smoking habit, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status classification, pre-operative corticosteroid therapy, pre-operative oxygen therapy, and pathological diagnosis of UIP.
Differences in outcomes between the two surgical approaches were also assessed using a propensity score-matched (PS) analysis using genetic method. PS was estimated using a priori selected variables that have been associated with Awake-VASLB: age, sex, smoking habit, BMI, ASA, pre-operative corticosteroid therapy, pre-operative oxygen therapy. After the matching, outcomes were evaluated with the same methods described above.
All statistical tests were two-sided and p-values of 0.05 or less were considered statistically significant. Data analysis was performed using Stata software version 15.1 (Stata-Corp, College Station, TX, USA) and R software version 3.5.1 (R Foundation for Statistical Computing, www.r-project.org/).
Results
Awake-VASLB was performed in 66 (66.0%) out of 100 patients who underwent SLB for suspected ILD, while 34 (34.0%) underwent Intubated-VASLB. Most patients were male (62.0%) and the mean±sd age at the time of surgery was 60.7±15.4 years. The UIP pattern was the most observed at histology (30.0%), followed by hypersensitivity pneumonitis (19.0%), nonspecific interstitial pneumonia (16.0% and sarcoidosis (8.0%) (table 1). The majority of operations were performed via bi-port VATS (n=55, 55%), followed by single-port VATS (35, 35%), and three-port VATS (10, 10%). Mean±sd surgical time was 51±37 min, mean±sd anaesthesiologic time was 51±35 min, the mean±sd number of biopsies obtained during surgery was 2.5±0.7, mean±sd chest drain duration 2.7±3.5 days and mean±sd post-operative length of stay 4.3±5.8 days. No cases of conversion from Awake-VASB to Intubated-VASLB were observed. Sixteen (16.0%) patients need rescue therapy for pain. In the whole cohort, 9 (9.0%) major complications, 5 (5.0%) unexpected admissions to ICU, 2 (2.0%) reinterventions and 1 (1.0%) post-operative death were observed.
Baseline characteristics in the overall population
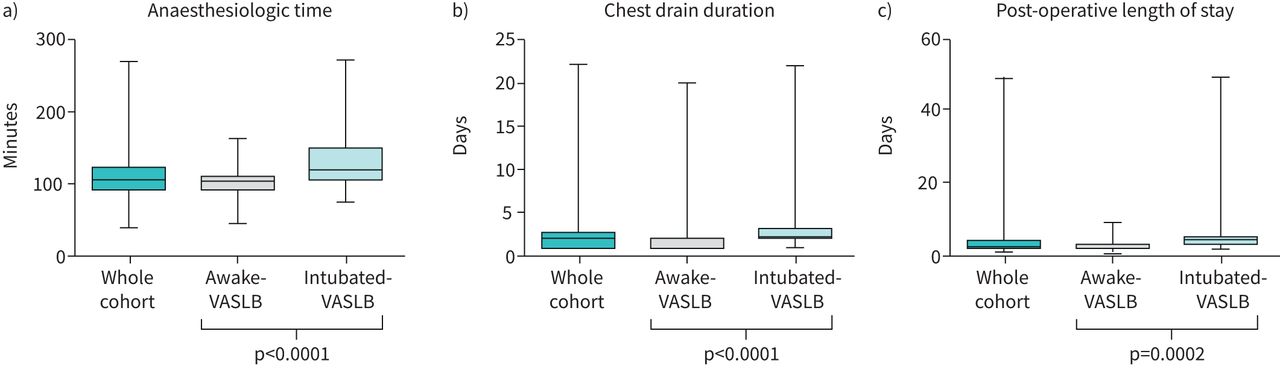
At the univariable analysis (figures 1 and 2), the Awake-VASLB group showed a significant lower post-operative morbidity rate (2 (3.0%) versus 7 (20.6%), OR 0.12, 95% CI 0.024–0.62; p=0.011). Moreover, patients submitted to Awake-VASLB showed less unexpected admission to ICU (1 (1.5%) versus 4 (11.8%), OR 0.12, 95% CI 0.012–1.08; p=0.058), less need of a rescue therapy for pain (6 (9.1%) versus 10 (29.4%), OR 0.24, 95% CI 0.079–0.73; p=0.012), a reduced surgical time (38 min versus 77 min; p <0.0001), a reduced anaesthesiologic time (97 versus 132 min; p<0.0001), a reduced chest drain duration (2.3 versus 3.5 days; p= 0.015) and a shorter mean post-operative length of stay (3.1 versus 6.7 days; p= 0.0002). The unexpected admissions to ICU were imputable to pneumonia (two cases in the Intubated-VASLB group), Type 1 respiratory failure (one case in the Intubated-VASLB group), Type 2 respiratory failure (one case in the Intubated-VASLB group), failure of epidural analgesia, and poor pain control immediately after the procedure (one case in the Awake-VASLB group). Patients submitted to Awake-VASLB had an increased number of biopsies obtained during the surgical procedure (2.6 versus 2.1; p<0.0001). No case of reintervention or post-operative death was observed in the Awake-VASLB group, while 1 (2.9%) reintervention and 1 (2.9%) post-operative death were observed in the Intubated-VASLB group.

Awake-video-assisted surgical lung biopsy (VASLB) versus Intubated-VASLB: a) crude, b) multivariable-adjusted and c) propensity score-matched analysis for post-operative morbidity, unexpected admission to ICU, and rescue therapy for pain.

{kind=link}
{kind=link}
Awake-video-assisted surgical lung biopsy (Awake-VASLB) versus Intubated-VASLB: Box-and-whisker plots illustrate the distribution of a) anaesthesiologic time, b) chest drain duration, and c) hospital post-operative length of stay.
At the multivariable analyses (figures 1 and 2), the Awake-VASLB was an independent protective factor for post-operative morbidity rate (OR 0.025, 95% CI 0.001–0.35; p=0.006) and unexpected admission to ICU (OR 0.042, 95% CI 0.002–0.70; p=0.027). A slight reduction [19] of the need for a rescue therapy for pain was also observed (OR 0.30, 95% CI 0.088–1.00; p=0.050).
Propensity score-matched analysis
Propensity score matching was used to create a cohort of 94 patients. The resulting two groups were well-matched regarding demographic and clinicopathological characteristics (table 2).
Awake-video-assisted surgical lung biopsy (VASLB) versus intubated-VASLB: baseline characteristics before and after propensity score matching
After matching (figures 1 and 2), the Awake-VASLB group was associated with a lower post-operative morbidity rate than the Intubated-VASLB group (OR 0.11, 95% CI 0.022–0.61; p=0.011), less unexpected admission to ICU (OR 0.092, 95% CI 0.009–0.87; p=0.037), a reduced need for rescue therapy for pain (OR 0.25, 95% CI 0.07–0.81; p=0.021), a reduced surgical (p=0.002) and anaesthesiologic time (p=0.0001), a reduced chest drain duration (p=0.008), a shorter post-operative length of stay (p=0.0006), and an increased number of biopsies obtained during surgery (p=0.0011).
Discussion
SLB is still considered the standard approach when a confident diagnosis of UIP cannot be obtained by imaging features and after a MDT discussion, as is still endorsed by the last evidence-based international guidelines [1].
Nevertheless, SLB, including the use of Intubated-VASLB, is affected by an elevated morbidity (up to 30%) and mortality rate (up to 4%), which is difficult to accept in routine clinical practice for a pure diagnostic scope [20]. By contrast, transbronchial cryobiopsy is generally a safer procedure showing a lower morbidity (pneumothorax rate 9.8%, severe bleeding rate 0.3%, moderate bleeding rate 8.7%) and mortality rate (0.3–0.5%) [21]. Even considering its lesser diagnostic efficacy in ILDs compared with SLB, the use of transbronchial cryobiopsy for this purpose has gained increasing attention, mostly because of its safety compared with the high morbidity and mortality risk associated with traditional Intubated-VASLB [21]. Moreover, its attractiveness resides in its easy applicability to most thoracic endoscopy facilities, especially compared with the strong anaesthesiologic and operative room expertise that are considered essential for successful application of Awake-VASLB.
The present prospective study showed that Awake-VASLB: 1) presents a consistent reduction of post-operative morbidities; 2) results in a reliable decrease of both post-operative mortality and reintervention rates, and also a reduction in the use of rescue therapy for pain; 3) saves hospital resources in terms of post-operative drainage time, as well in terms of hospital length of stay and minimising the use of unplanned ICU admissions; and 4) provides at least the same amount of lung tissue biopsies as Intubated-VASLB.
Any thoracic surgical procedure in ILD patients represents a challenge for thoracic surgeons and anaesthesiologists [22]. Nevertheless, the thoracic surgery domain is incessantly developing, and anaesthesiologists and thoracic surgeons should maintain a continued focus on minimising procedure-related morbidity and, at the same time, maximising therapeutic and diagnostic benefits in such frequently fragile patients (e.g. age, type of disease, frequent comorbidities). In this context, Awake-VASLB has been recently proposed for SLB in suspected ILDs [23].
Undoubtedly, feasibility and patient safety are major issues in ILD patients referred for SLB. In particular, the reported morbidity and mortality rate could follow respiratory dysfunction induced by mechanical ventilation (barotrauma). This has been clearly reported in the literature [10, 12–14]. In particular, muscle relaxants are known to produce adverse respiratory effects by residual muscle block, including weakness of upper airway muscles, airway obstruction, and diaphragmatic dysfunctions [10]. Consequently, a surgical approach based on spontaneous ventilation, avoiding the use of neuromuscular blocking agents, is expected to reduce intraoperative lung injury and, therefore, to be associated with less post-operative adverse events, representing a valid strategy in high-risk ILD patients. Indeed, our study seems to confirm that patients undergoing Awake-VASLB were found to be associated with a remarkable reduction of post-operative morbidity and mortality (odds ratio for post-operative complications in VASLB: 8.1, p=0.011). Remarkably, we also observed a decrease in anaesthesiologic time and unanticipated post-operative use of ICU. This is also in line with a more favourable post-operative period characterised by a reduction in length of thoracic drain maintenance and post-operative length of stay. These results are consistent with current literature reporting the use of Awake-VASLB in the context of other thoracic disease [24] and the observed rate of complication is not dissimilar to that reported for cryobiopsy performed in expert centres [21].
The MDT (which usually comprises clinicians, thoracic radiologists and thoracic pathologists) is considered the best way to manage the diagnostic pathway as well as other aspects of management of patients affected by an ILD [25, 26]. Moreover, an acceptable risk–benefit ratio should be considered as a guide during the multidisciplinary discussion (including thoracic surgeons) for the choice of either the Awake-VASLB or intubated surgery. Indeed, the decrease of the risk–benefit balance together with an enhanced diagnostic yield represents the goal to be reached in each patient, taking into account the disease severity per se, the patient's comorbidities, and the possible deadly outcome of potential acute exacerbations related to the intubated procedure. Consequently, in our institution, throughout the MDT discussion, a careful evaluation of the risk–benefit ratio was carried out, tailoring the technique for every single patient. Interestingly, we observed is a trend towards lower diffusing capacity of the lung for carbon monoxide in the Awake-VASLB group. This data could suggest that in our cohort patients with more severe ILD more likely underwent awake surgery in order to minimise the risk of possible complications and, in particular, acute exacerbations.
One of the major concerns during the diagnostic procedure in ILD is to obtain sufficient material for an accurate diagnosis. In our study, we observed a slightly increased number of biopsies performed in the Awake-VASLB group. A possible explanation could be related to the surgeon's preference to perform an “extra biopsy”, influenced by the awake patient setting, and to be sure to obtain sufficient material for diagnosis. However, in both groups, the mean number of biopsies performed was in accordance with the most recent guidelines (i.e., at least two biopsies), and the difference observed (0.5 biopsies in favour of Awake-VASLB) was in our opinion not of clinical or practical relevance. However, is important to note that our study demonstrated that the Awake-VASLB procedure did not imply an inferior number of biopsies achieved, as compared to Intubated-VASLB.
Almost certainly, patients undergoing thoracic surgery could experience post-operative pain, even if submitted to minimally invasive thoracic surgery (e.g. VATS). However, intra-operative and post-operative use of opioids could be related to impaired recovery and readmission after hospital discharge [11]. In recent years, chronic opioid use and addiction have emerged as a public concern, even if more perceived in the USA than in Europe. A correct therapeutic approach to acute pain relief certainly plays a major role in this context [27]; even so, the use of spontaneous ventilation in the Awake-VASLB group led to a significant reduction in rescue therapy administration. Further studies are needed to better define the advantage of spontaneous ventilation surgery on pain control.
Finally, as our results also had a positive impact on the optimal management of hospital resources, it follows that the encouraging clinical results obtained and the minimal use of hospital resources could, in the near future, facilitate the spread of Awake-VASLB, even outside high-volume academic centres.
Our study has several limitations, principally related to the lack of randomisation to prevent selection bias [28]. However, the prospective nature of the study permits real-life adherence, warrants good data reliability, and therefore, seems to confirm the findings [29]. Moreover, we performed a propensity-matched analysis that was employed to minimise patient selection bias.
In conclusion, the results obtained from the analysis of our prospective series suggest that Awake-VASLB is feasible and safe in patients affected by ILD, significantly reducing post-operative complications, unexpected ICU admission, reintervention, and mortality. Awake-VASLB had the same diagnostic yield as Intubated-VASLB. We hope that the results obtained, to date, will lead to more widespread use of Awake-VASLB and stimulate further prospective comparison studies with other procedures presenting similar post-procedural complication rates (such as transbronchial cryobiopsy). The emerging evidence regarding the effectiveness of this approach, including that obtained in the present study, should be considered in the next guidelines on the management of ILD patients.
Footnotes
Author contributions: All co-authors are accountable for the criteria for authorship according to the International Committee of Medical Journal Editors.
Conflict of interest: F. Guerrera has nothing to disclose.
Conflict of interest: L. Costardi has nothing to disclose.
Conflict of interest: G.L. Rosboch has nothing to disclose.
Conflict of interest: P. Lyberis has nothing to disclose.
Conflict of interest: E. Ceraolo has nothing to disclose.
Conflict of interest: P. Solidoro has served as investigator in clinical trials, consultant or speaker for Alfasigma, AstraZeneca, Boehringer Ingelheim, GSK, Menarini, Novartis, Chiesi, Guidotti & Malesci and ABC Farmaceutici outside this work.
Conflict of interest: C. Filippini has nothing to disclose.
Conflict of interest: G. Verri has nothing to disclose.
Conflict of interest: L. Brazzi has nothing to disclose.
Conflict of interest: C. Albera has nothing to disclose regarding this work, but has served as investigator in clinical trials, consultant, speaker, steering committee or scientific advisory board member for Bayer, Boehringer Ingelheim, FibroGen, Gilead, Grifols, GSK, Roche, MSD, Sanofi Aventis outside this work.
Conflict of interest: E. Ruffini has nothing to disclose.
- Received August 31, 2020.
- Accepted April 29, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










