





Abstract
The aim of this study was to determine if there is a difference in 6-min walk test (6MWT) distance when the assessor accompanies the patient to continuously measure peripheral oxygen saturation (SpO2) compared to the patient walking unaccompanied.
We conducted a randomised crossover study to evaluate the impact of the assessor walking with the patient during the 6MWT (6MWTwith) versus the patient walking alone (6MWTwithout). At the end of a pulmonary rehabilitation programme, each patient performed two 6MWTs in random order and separated by a 30-min rest.
49 patients with chronic obstructive pulmonary disease (COPD) (Global Initiative for Obstructive Lung Disease classification II–IV) were included. In a regression model adjusting for period and subject, accompanying the patient resulted in a lower walking distance (mean difference −9.1 m, 95% CI −13.9– −4.3, p=0.0004). Notably, six patients walked more than 30 m farther (minimal important difference) in one of the two conditions (6MWTwith: n=1, 6MWTwithout: n=5). There were no between-sequence-group differences in heart rate, dyspnoea, leg fatigue and SpO2. The median (interquartile range) number and duration of SpO2 signal artefacts were high but not different between the experimental conditions (6MWTwith: 17 (4–24), 34 s (7–113 s); 6 MWTwithout: 11 (3–26), 24 s (4–62 s)).
At a study population level, we observed a statistically significant difference in 6MWT distance between the two experimental conditions; however, the magnitude of difference was small and may not be clinically relevant. Nevertheless, in a clinical setting, unaccompanied walking resulted in a substantially higher walking distance in individual patients, pointing towards strictly standardised testing methodology, in particular in pre–post study designs.
Abstract
Accompanied walking during a 6MWT versus unaccompanied walking results in shorter walked distance (mean difference −9.1 m, 95% CI −13.9– −4.3 m). No differences in nadir SpO2 or oximetry artefacts were noted between accompanied and unaccompanied walking. https://bit.ly/3tBjfCq
Introduction
The 6-min walk test (6MWT) is a field walking test to assess functional exercise capacity [1]. It is a widely used functional capacity test to evaluate a person's physical fitness, to assess effects of interventions such as rehabilitation programmes and for prognostic purposes [2]. The test is commonly used to measure the lowest peripheral oxygen saturation (SpO2) during self-paced exercise [3]. Exercise-induced hypoxaemia is frequently observed in patients with pulmonary disorders [4, 5] and the lowest SpO2 does not necessarily occur at the end of the test [6, 7]. Moreover, the extent of oxygen desaturation is important for determining the indication for supplemental oxygen during daily life activities and exercise therapy [4], and to gain indicators for the prognosis in chronic obstructive pulmonary disease (COPD) [8].
In 2002, the American Thoracic Society published a technical standard on the 6MWT suggesting that the assessor must not walk with the patient [9]. In an update published in 2014 by the European Respiratory Society and the American Thoracic Society, the document highlights the importance of the continuous measurement of SpO2 during the 6MWT in pulmonary disorders [1]. Therefore, it has been recommended that the assessor accompanies the patient during the 6MWT to continuously monitor SpO2 (i.e. to be able to capture the lowest (nadir) value during the test) [1].
Precise standardisation of testing methodology is of critical importance when conducting a 6MWT. It has been shown that small changes in the testing methodology (e.g. changes in track length, track layout, supplemental oxygen or verbal instructions) and learning experience due to repeated tests affect 6MWT distance [3, 10–13]. No study has evaluated the impact of the assessor walking behind the patient versus standing aside on the 6MWT distance, the primary outcome measure in a 6MWT test, in people with COPD.
This study was designed to assess the impact of the assessor accompanying the patient compared to the patient walking alone (i.e. unaccompanied) on 6MWT distance and nadir SpO2.
Material and methods
Study design and study subjects
We conducted a randomised crossover trial at the Berner Reha Zentrum AG, a specialised rehabilitation clinic located in Bern, Switzerland.
Patients with COPD and Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification II–IV (forced expiratory volume in 1 s (FEV1)/forced vital capacity (FVC)<0.7, FEV1<80% predicted) were included [14]. We calculated % predicted values and z-scores for FEV1 and FVC based on equations by Quanjer et al. [15]. We excluded patients who were physically unable to perform a 6MWT (e.g. owing to unstable cardiac disease) or who were unable to understand the instructions for the 6MWT (e.g. owing to cognitive impairment or insufficient knowledge of the language in which the instructions were given).
The study protocol was approved by the Cantonal Ethics Committee Zurich (2019-00827) and the study was registered at clinicaltrials.gov (NCT04033783).
Patients gave their written informed consent to participate in the study, after they were given at least 24 h to decide [16]. The recruitment was performed consecutively between September and December 2019. All data were collected in REDCap (Research Electronic Data Capture; Vanderbilt University, Nashville, TN, USA [17]), a secure, web-based application designed to support data capture for research studies, hosted at the Clinical Trials Center at the University Hospital of Zurich.
Randomisation and allocation concealment
We used simple randomisation (1:1 ratio) to randomly allocate patients into either one of two sequence groups: first assessment 6MWT with the assessor walking behind the patient (6MWTwith) and second 6MWT with the patient walking alone (6MWTwithout), or vice versa. The randomisation list was created with R software [18] (coded as 0=starting with 6MWTwithout or 1=6MWTwith, n=60 to account for potential dropouts) using the R package blockrand [19]. The list was compiled by a biostatistician (SRH) who was not involved in the study recruitment, randomisation or study-specific assessments. A person not involved in the study implemented the randomisation list into the database (REDCap [17]) to ensure complete concealment of random allocation. Randomisation within REDCap was always performed by the same person, after inclusion and exclusion criteria were evaluated.
6MWT
The 6MWT was performed on a 30 m floor according to a recent technical standard [1]. All assessments were performed at the end of the inpatient pulmonary rehabilitation programme (1–7 days before leaving the clinic) and supervised by the same assessor (TFR) throughout the entire study. Patients and assessor were not blinded to the experimental condition. All included patients had already performed at least one and up to three 6MWTs prior to the study assessments, thus accounting for possible learning effects [3].
Prior to the study assessments, each patient had at least 1 h of rest before starting the first allocated walking test. After randomisation, each patient conducted two 6MWTs. Between the two tests, there was a resting phase of 30 min to allow heart rate and SpO2 to reach pre-testing values [1]. Before each 6MWT patients received the standardised instruction for the test as described by Holland et al. [1], which has been translated by our research group into German. Additionally, all 6MWTs were monitored with pulse oximetry, using a handheld pulse oximeter (Covidien Nellcor PM10N, Dublin, Ireland). The sensor was attached to the patient's left middle finger and fixed with tape (figure 1a).

Sensor fixation with tape and experimental conditions. a) Sensor fixation with tape. b) 6-min walk test (6MWT) in which the patient walked alone with the pulse oximeter around the trunk (6MWTwithout). c) 6MWT in which the assessor walked behind the patient (6MWTwith).
In the 6MWTwith, the pulse oximeter was held by the assessor who walked 1 m behind and did not “pace” the patient, as recommended (figure 1c) [1]. The 6MWTwithout condition was performed without the assessor walking with the patient (i.e. the assessor was standing at the 15 m mark of the 30 m test course). In this condition, the pulse oximeter was placed around the trunk of the patient and fixed with a strap (figure 1b). Walking aids and/or supplemental oxygen dose, if needed, were identical during both experimental conditions.
After completion of the two 6MWTs, patients filled out a self-administered questionnaire to report their subjective perception with regards to preferences, velocity and safety during both 6MWTs.
Analysis
The sample size calculation was performed using a predefined difference of 30 m between the 6MWTs under the two conditions, which is the established minimal important difference (MID) for patients with COPD [3]. We assumed a standard deviation of the change scores of the 6MWT of 73 m [3], which equals an effect size of 0.41. To achieve a power of 80% to detect a difference of 30 m with an assumed standard deviation of 73 m, 49 patients were required, assuming a two-sided significance level of 0.05. The sample size calculation was performed with G*Power 3.1.9.2 [20].
For the primary endpoint (6MWT distance in metres), a linear regression model adjusting for the experimental condition (6MWTwith versus 6MWTwithout, coded as 1, 0), period (first test or second test) and subject was performed [21].
Secondary outcomes were patient-reported perception of different aspects such as feeling of safety, self-perceived influence on gait velocity or interfering factors during the two versions of the 6MWT.
Exploratory outcomes were pre- and post-test heart rate, dyspnoea and leg fatigue (0–10 Borg scale), and pulse oximetry data from the two 6MWTs per subject. Pulse oximetry data were used to quantify measurement artefacts and the lowest SpO2 (nadir value) during the 6MWT. Pulse oximetry data were downloaded as csv data sheets from the pulse oximeter using Nellcor Analytics Tool (version 1.6.0). The lowest SpO2 values were manually corrected, if needed, to obtain the true SpO2 nadir without measurement artefacts. Exploratory outcomes were evaluated using the same adjusted linear regression model as for the primary endpoint.
Statistical analyses were performed using IBM SPSS Statistics version 26.0 [22] and R version 3.6.3 [18].
Results
Patients
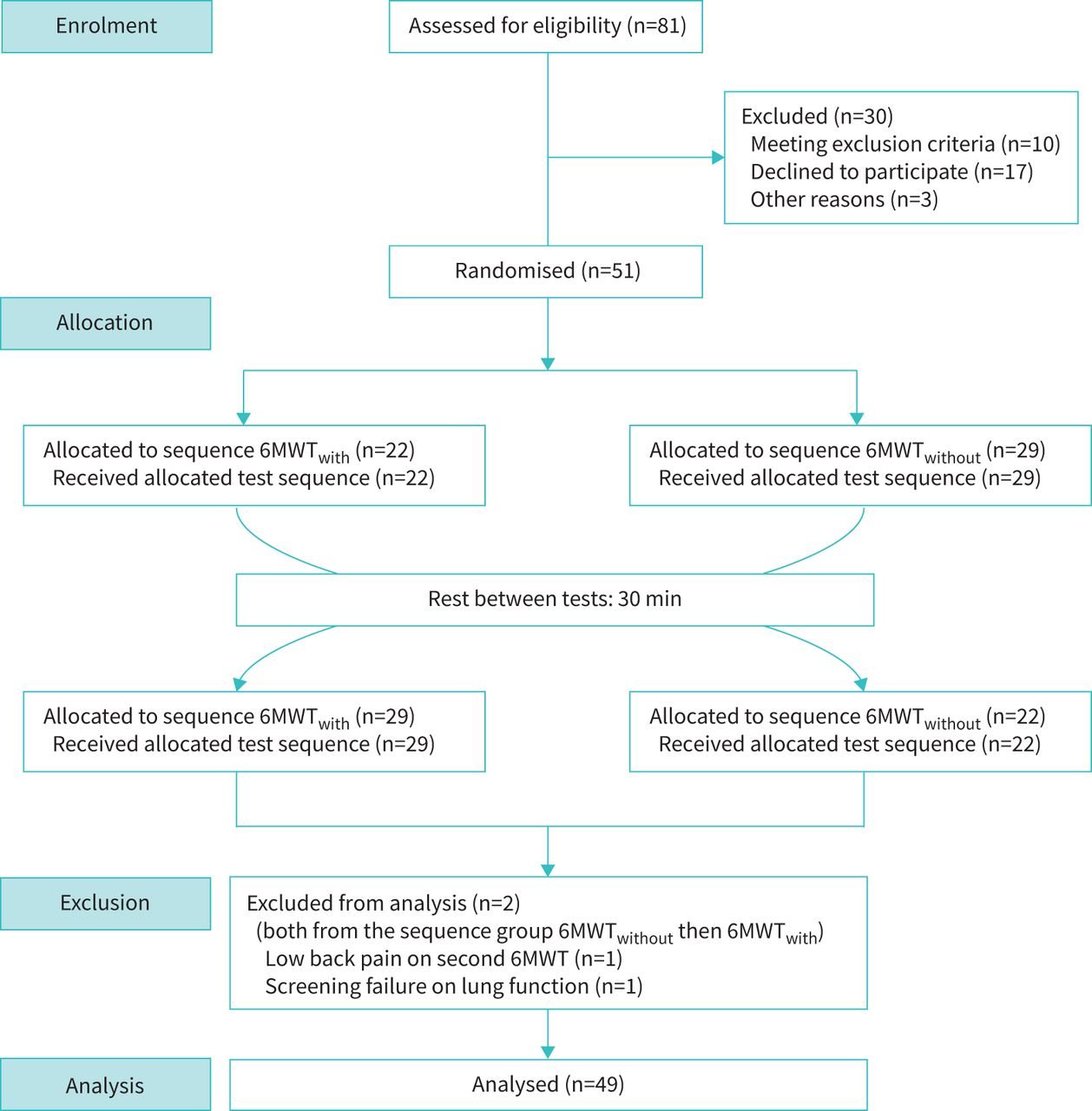
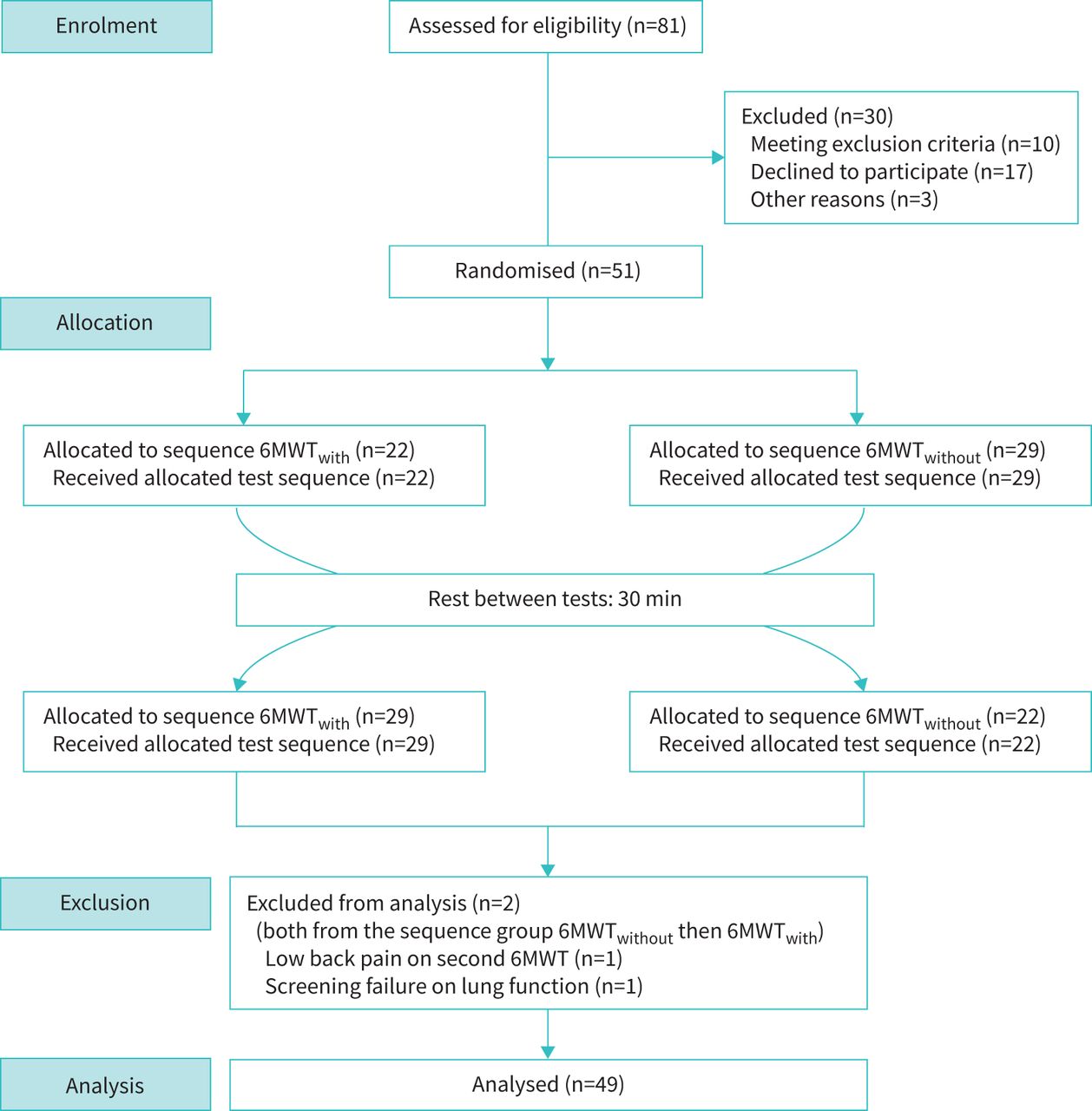
51 patients were included in the study. Of those, 22 patients were randomised to the sequence group 6MWTwith followed by 6MWTwithout and 29 were randomised to the sequence group 6MWTwithout followed by 6MWTwith. Two patients of the 6MWTwithout then 6MWTwith group were excluded from the analysis. One patient reported that he had to walk slower on the second 6MWT because of low back pain. The other patient was excluded because of a screening failure (i.e. lung function data did not adhere to inclusion criteria). In total, data from 49 patients were analysed (figure 2) [23].
{kind=link}
{kind=link}
Study flow chart. 6MWT: 6-min walk test.
Baseline characteristics are shown in table 1. Pre- and post-walking test values for heart rate, SpO2 and perceived dyspnoea and leg fatigue are given in supplementary table S1. Overall, 6% (n=3) used a walking aid, 6% (n=3) used supplemental oxygen (ranging from 1 to 10 L·min−1), 37% (n=18) used both a walking aid and supplemental oxygen and 51% (n=25) used neither a walking aid nor supplemental oxygen during the 6MWTs. The used walking aids and oxygen dose were the same during both experimental conditions.
Patient characteristics
6MWT distance
Walking behind the patient during the 6MWT (6MWTwith) resulted in a shorter walking distance of −9.1 m (95% CI −13.9– −4.3, table 2). On the individual level, with regards the MID, five patients (10%) walked a distance that was ≥30 m longer when walking alone (6MWTwithout). In contrast, one patient (2%) walked a distance that was ≥30 m longer when the test was accompanied (supplementary figure S1).
Differences in walking distance and oxygen saturation between the two experimental conditions
Pulse oximetry: SpO2 and signal artefacts
There were no significant differences in SpO2 nadir and pulse oximetry artefacts in absolute numbers and duration between the two experimental conditions (table 2). The median (interquartile range) number and duration of SpO2 signal artefacts were not different between the two experimental conditions (6MWTwith: 17 (4–24), 34 s (7–113 s); 6 MWTwithout: 11 (3–26), 24 s (4–62 s)). The nadir SpO2 during all 6MWTs was in 61–69% of cases lower than the post-test SpO2 (6MWTwith: 30 out of 49 cases; 6MWTwithout: 34 out of 49 cases). Among a total of 98 walking tests, a difference of ≥3% between SpO2 post-test and SpO2 nadir values was found for 15 tests (15%), while a difference of ≤2% was observed in 83 tests (85%).
Patients’ perceptions
Patients’ perceptions during the 6MWTwith are summarised in supplementary table S2.
59% (n=29) of patients stated no preference for either of the two 6MWTs, whereas 25% (n=12) preferred the 6MWTwith and 16% (n=8) preferred the 6MWTwithout.
Patients favouring the 6MWTwith noted “safety and supervision” (n=4), “less loneliness” (n=1), “easier walking” (n=2), “test goes by faster” (n=3), “self-induced reminder on breathing technique” (n=2) and “more motivating to walk together” (n=2) as reasons. Patients preferring the 6MWTwithout reported feeling “more free and having no pressure while walking” (n=4), “choosing their own tempo” (n=3) and “being used to walk alone” (n=2) as their preferential reasons.
In addition, two patients who reported feeling “stressed” by the assessor accompanying them mentioned the “cable of the pulse oximeter” (n=1), “proximity of the assessor” (n=1) and “feeling a lower velocity of the assessor” (n=1) as reasons.
Discussion
This randomised crossover study investigated the impact of the assessor walking behind the patient compared to the patient walking alone on the distance covered during a 6MWT in people with COPD. We observed a shorter walking distance in the test condition in which the assessor accompanied the patient (6MWTwith) than in the condition in which the patient was walking alone (6MWTwithout). No differences between study conditions were observed in nadir SpO2 or the number and duration of signal artefacts during pulse oximetry measurements. The majority of patients had no preference for either test condition.
6MWT distance
In this study, accompanying the patient resulted in a shorter 6MWT distance of −9.1 m (95% CI −13.9– −4.3) compared to the patient walking alone. Our data suggest a systematic difference resulting in a shorter 6MWT distance when the assessor walks behind the patient. At a population level, the magnitude of the observed difference of −9.1 m is small (about 2–3% of the total walking distance) and below the well-established MID for the 6MWT [3]. However, at an individual level, we noticed that about 10% (n=5) of the patients walked ≥30 m farther when walking alone. In comparison, only one participant walked farther when accompanied. Unfortunately, the authors are not aware of any previous studies assessing the intra-day variability in 6MWT distance in people with (cardio)respiratory diseases that would facilitate the interpretation of the magnitude of observed effects. Numerous studies have investigated the impact of changes in testing methodology on 6MWT distance, e.g. additional verbal encouragement [24], use of different test instructions [13], walking with walking aids [25–30], supplemental oxygen [31–35] or compressed air [36], carrying oxygen devices [35, 37], different track layouts [11, 12] and track lengths [10], which have led to differences in 6MWT distance ranging from −49.5 m to 109 m. Considering the huge variability arising from changes in testing methodology, our between-test difference seems small when interpreted at a population level. However, it is unclear to what extent additive or multiplicative interaction could occur when other additional methodological changes are applied. It is important to note that, in contrast to research settings, the risk for methodological changes might be even greater in clinical settings, e.g. when different assessors supervise walking tests.
Pulse oximetry: SpO2 and signal artefacts
In our study, no differences between the two walking test conditions were observed in nadir SpO2 or the number and duration of signal artefacts during pulse oximetry measurements.
Oxygen desaturation is common in chronic lung diseases, especially during exercise [4, 5], and the extent of desaturation during a 6MWT can provide important information regarding disease severity, prognosis [8] and supplemental oxygen titration. It must be noted that the lowest SpO2 does not always occur at the end of the 6MWT [6]. This is one reason (among others) that continuous pulse oximetry monitoring during the 6MWT is recommended [1]. In general, pulse oximetry during the 6MWT is a reliable measurement under the condition that a high-quality and stable signal is received [1, 3]. Pulse oximeters need the pulse waveform to calculate the correct SpO2 value [38]. In this study, the assessor held the pulse oximeter in order to clearly see the pulse waveforms. To ensure an adequate pulse wave signal we fixed the sensor with tape around the left middle finger and on the back of the hand. However, despite additional fixation we observed a high number and long duration of signal artefacts in each single walking test (table 2). Nonetheless, there were no differences in SpO2 signal artefacts between the two experimental conditions, suggesting that the assessor carrying the pulse oximeter when walking behind the patient did not introduce measurement bias.
We observed differences between the nadir and post-test SpO2 values in 64 out of 98 (65%) of the 6MWTs. Overall, the differences in SpO2 recordings ranged from 0% to 12%. In 15 out of 98 tests a ≥3% difference between post-test and nadir SpO2 was observed, whereas in 83 out of 98 tests the difference was ≤2%. Our results indicate little difference between the post-test SpO2 and nadir SpO2. Our data confirm previous studies [6, 7] demonstrating differences between nadir SpO2 and post-exercise SpO2 values, underlying the need to continuously monitor SpO2 during the 6MWT [1].
Patients’ perceptions
Most patients did not state a preference for either of the two experimental conditions. If they preferred one condition over the other, it was mostly due to personal preference and experience (e.g. favourably walking alone at home).
Similarly, a majority of the patients did not feel their walking speed was negatively affected by the assessor walking behind them during the test. Slightly more dispersion was observed in the answers concerning if the patients felt driven. However, this contradicts the lower mean walking distance in the 6MWTwith condition.
Interestingly, one third of patients felt safer when the assessor walked behind them.
Strengths and limitations
One strength of our study is the randomised crossover design [23], which minimises inter-subject variability and confounding factors. Furthermore, all study assessments were conducted at the end of a pulmonary rehabilitation programme when patients were in stable clinical condition and potential learning effects for the 6MWT were diminished [39]. The latter is supported by the fact that all patients had performed at least one 6MWT and 72% of patients had performed two or three walking tests before inclusion into the study.
Limitations of the study include lack of masking of the outcome assessor, which was not possible because of the design. However, all assessments were performed and supervised by the same person and followed a standardised testing protocol, thus lessening measurement bias. With respect to pulse oximetry measurements, we acknowledge that finger probes, compared to forehead sensors, are more prone to inaccurate measurements owing to motion artefacts or poor perfusion of fingertips. Additionally, pulse oximetry devices with Bluetooth connection already exist to assess SpO2 remotely. However, Bluetooth devices may not be readily available in every clinical setting and additional time is required to analyse SpO2 recordings to be able to determine the nadir value. Therefore, the chosen measurement methodology in our study may best reflect the typical clinical setting, in which handheld pulse oximeters are being used.
In conclusion, walking behind the patient during a 6MWT, compared to the patient walking alone, results in a shorter walking distance in the range of −13.9 to −4.3 m. This difference is considered small but supports the need for strict standardisation of testing methodology, especially in repeated measures study designs, clinical settings and between-group comparisons.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material 00921-2020.SUPPLEMENT
Footnotes
This article has supplementary material available from openres.ersjournals.com
ClinicalTrials.gov identifier: NCT04033783. Ethical approval number: 2019-00827.
Data availability: Our dataset has been deposited with Dryad (https://doi.org/10.5061/dryad.gmsbcc2n7).
Conflict of interest: T.F. Riegler has nothing to disclose.
Conflict of interest: A. Frei has nothing to disclose.
Conflict of interest: S.R. Haile has nothing to disclose.
Conflict of interest: T. Radtke has nothing to disclose.
- Received December 7, 2020.
- Accepted March 13, 2021.
- Copyright ©The authors 2021
This version is distributed under the terms of the Creative Commons Attribution Non-Commercial Licence 4.0. For commercial reproduction rights and permissions contact permissions{at}ersnet.org
References










